
記住我


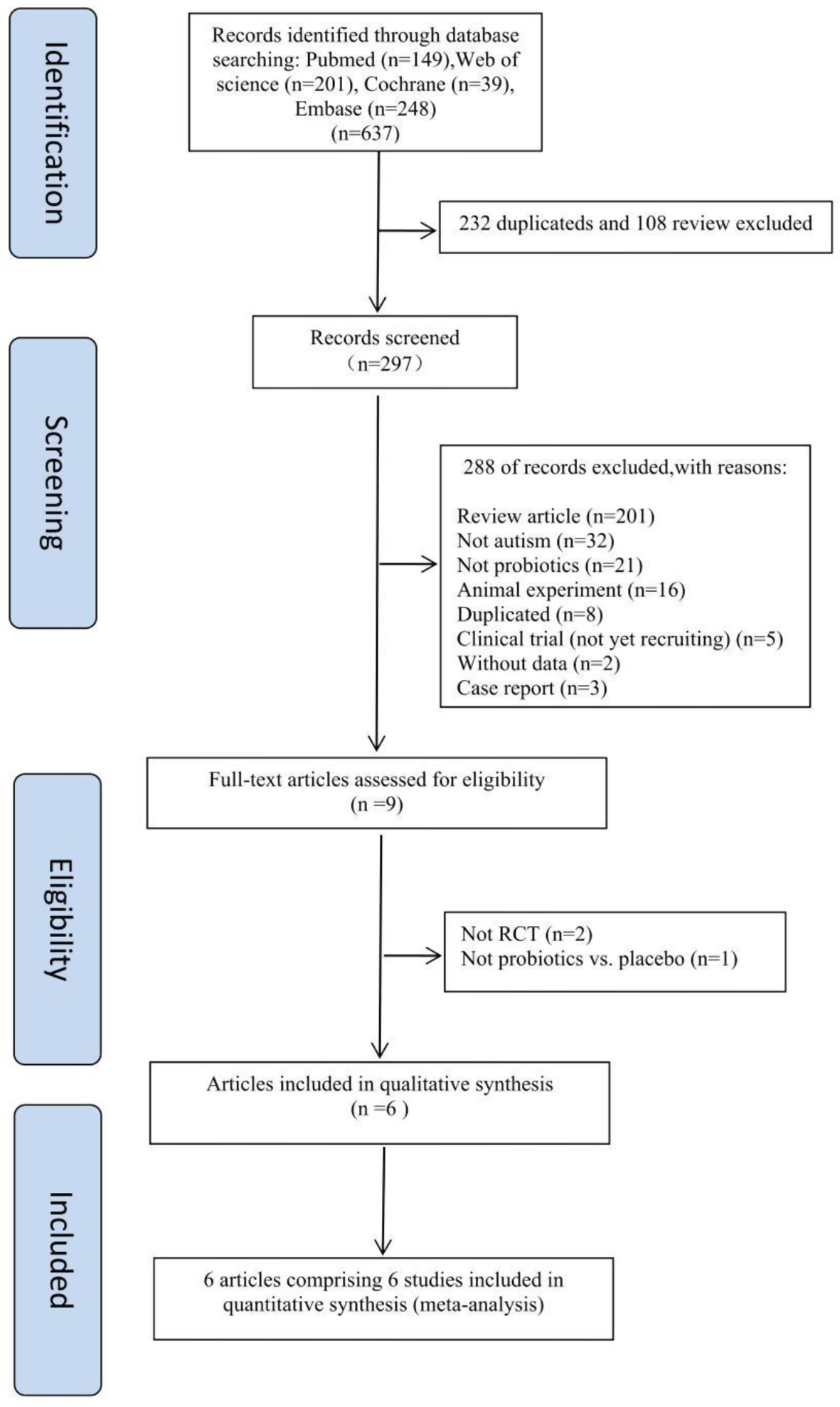
During this 13-year period, 735,887 admissions to our ED were recorded. Through keyword search, 13,586 medical records were obtained. Of these, only 1409 records met the study eligibility criteria (Fig. 1), with an observed incidence of torticollis presentation of 19 cases per 10,000 accesses.
Fig. 1
The clinical and demographic characteristics of the study patients are outlined in Table 1.
Table 1 Characteristics of study sample*The median age of patients was 5.7 (IQR 5.8; 5th-95th, 0.5–13.9) years. Most patients were male (54%), with a female-to-male ratio of 1:1.2. Access priority was considered intermediate/high based on triage (code red-yellow until 2019, red-orange-blue from 2020 onward) in 130 patients (9.2%). A history of trauma was present in 393 patients (27.9%). The median time from onset of torticollis to DEA admission was less 24 h (range 0–14 days), with 822 children brought to the ED in the first 24 h after the onset of torticollis. The side of head deviation was specified in 1179 patients (83.7%), divided into leftward in 745 (63.2%) and rightward deviation in 434 (36.8%) children. The signs and symptoms most frequently reported were pain (83.5%), pharyngodynia (16%), fever (11.3%) and laterocervical tumefaction/lymphadenopathy (6.4%). Less frequently encountered symptoms included headache (5.1%), earache (4.9%), vomiting (3.1%), and dizziness (1.3%). A complete blood count was available for 220 patients. The median leukocyte count of these patients was 9520/µl (with a median neutrophil percentage of 57.7%) but 30.9% of the patients had leukocytosis. The C-reactive protein assay was performed in 213 patients, and 106 (49.8) reported a value above 0.5 mg/dl. Imaging was performed in 663 patients (47.1%). Of these, 28%, 12.4% and 11.7% of patients underwent radiography, CT or ultrasound of the head and neck region, respectively. At least one pathological finding was found in 5.4 to 7.9% of these exams. An MRI was performed in a minority of patients (5.4%). Consultation with a specialist was necessary in 359 cases (25.5%), mainly an orthopedic (16.4%), followed by a neurologist (7.9%). Treatment included prescription of ibuprofen in 1121 patients (79.6%), antibiotics in 125 (8.9%) and acetaminophen in 111 (7.9%). A cervical collar was applied in 806 patients (57.2%). Eighteen patients (1.3%) required surgery. Hospitalization was required in 156 cases (11.1%), with a median duration of 4 days (IQR 4, 5th-95th 1–22). Most patients were discharged without further sequelae (97.9%).
The etiology of torticollis by main categories is shown in Table 2.
Table 2 Etiology of torticollisA postural cause was recognized in 607 (43.1%) of patients. For 415 patients (29.5%) torticollis was attributed to a traumatic cause. Of these, 62.7% suffered direct trauma to the head-neck district, resulting in atlantoaxial subluxation in 17 patients (6.5%) and vertebral fracture in 5 patients (1.9%). Abnormal cervical motion (sprain, whiplash, hyperextension, etc.) caused torticollis in 37.3% of patients, resulting in atlanto-axial subluxation in 12 patients (7.7%). No vertebral fractures were documented as a result of abnormal neck movements. An infective/inflammatory etiology involved 19.1% of patients, with pharyngo-tonsillitis as the main cause (48%), followed by laterocervical lymphadenitis (26.4%), and otitis media (13%). The etiology of torticollis was neurological in 46 patients (3.3%), with benign paroxysmal torticollis being the most frequent cause (73.9%). Secondary causes were dystonic drug reactions (6.5%) and dystonia with a probable genetic basis (4.3%). There were 35 patients with congenital torticollis (2.5%), caused by muscular contracture (77.2%), plagiocephaly/postural deformity (14.3%) and Klippel-Feil syndrome (8.6%). Different tumor types caused oncological torticollis in 17 patients (1.2%), mainly bone marrow or brainstem tumor in 5 patients (29.4%), Langerhans cell histiocytosis in 4 (23.5%), posterior cranial fossa tumor in 3 (17.7%). The remaining causes of torticollis in 20 patients (1.4%) included osteoarticular/rheumatologic disorders in 8 patients (40%) and strabismus in 6 (30%).
The comparison between patients with and without an urgent condition underlying the torticollis is shown in Table 3.
Table 3 Comparison of patients with an urgent and non–urgent condition*Patients with an urgent condition underlying the torticollis were significantly older (median age 6.9 vs. 5.7 years, p = 0.027), more frequently reported a history of trauma (41% vs. 27.2%, p = 0.008), and were admitted to the ED significantly later than patients without an urgent condition (23% vs. 60% in less than 24 h, p < 0.001). Regarding clinical presentation, a left head deviation was more frequent in patients with an urgent condition than in those without (53.2% vs. 35.9%, p = 0.006). Similarly, headache (11.5% vs. 4.7%, p = 0.015), vomiting (12.8% vs. 2.6%, p < 0.001) and dizziness (5.1% vs. 1.1%, p = 0.018) were more prevalent in patients with urgencies. Considering the diagnostic work-up, as expected, instrumental investigations (96.2% vs. 44.1%, p < 0.001) and specialist consultations (88.5% vs. 21.8%, p < 0.001) were performed more frequently in patients with urgent causes of torticollis, with also more frequent pathological findings (see Table 3). Antibiotics (26.9% vs. 7.8%, p < 0.001) and ibuprofen (57.7% vs. 80.8%, p < 0.001) were administered more frequently in patients with urgent and non-urgent conditions, respectively. Hospitalization (78.2% vs. 7.1%, p < 0.001), with a longer median duration (7 vs. 3 days, p < 0.001) was observed more frequently in patients with urgent causes of torticollis. Sequelae were described more in patients with urgent conditions (23.1% vs. 0.8%, p < 0.001).
The logistic regression analysis, adopting urgency of the underlying condition as the dependent variable, is shown in Table 4.
Table 4 Logistic regression analysis (dependent variable: urgent cause of torticollis)We found that time from onset of torticollis to referral to the ED (OR 0.98, p 0.006) was negatively associated with the odds an underlying urgent condition in the logistic model. By contrast, the presence of clinical signs/symptoms such as headache (OR 2.45, p 0.018) and vomiting (OR 3.63, p 0.002)) were the only variables strongly characterized by the presence of an urgent condition, after adjusting for the other clinically and statistically significant variables in the bivariate analysis.
留言 (0)