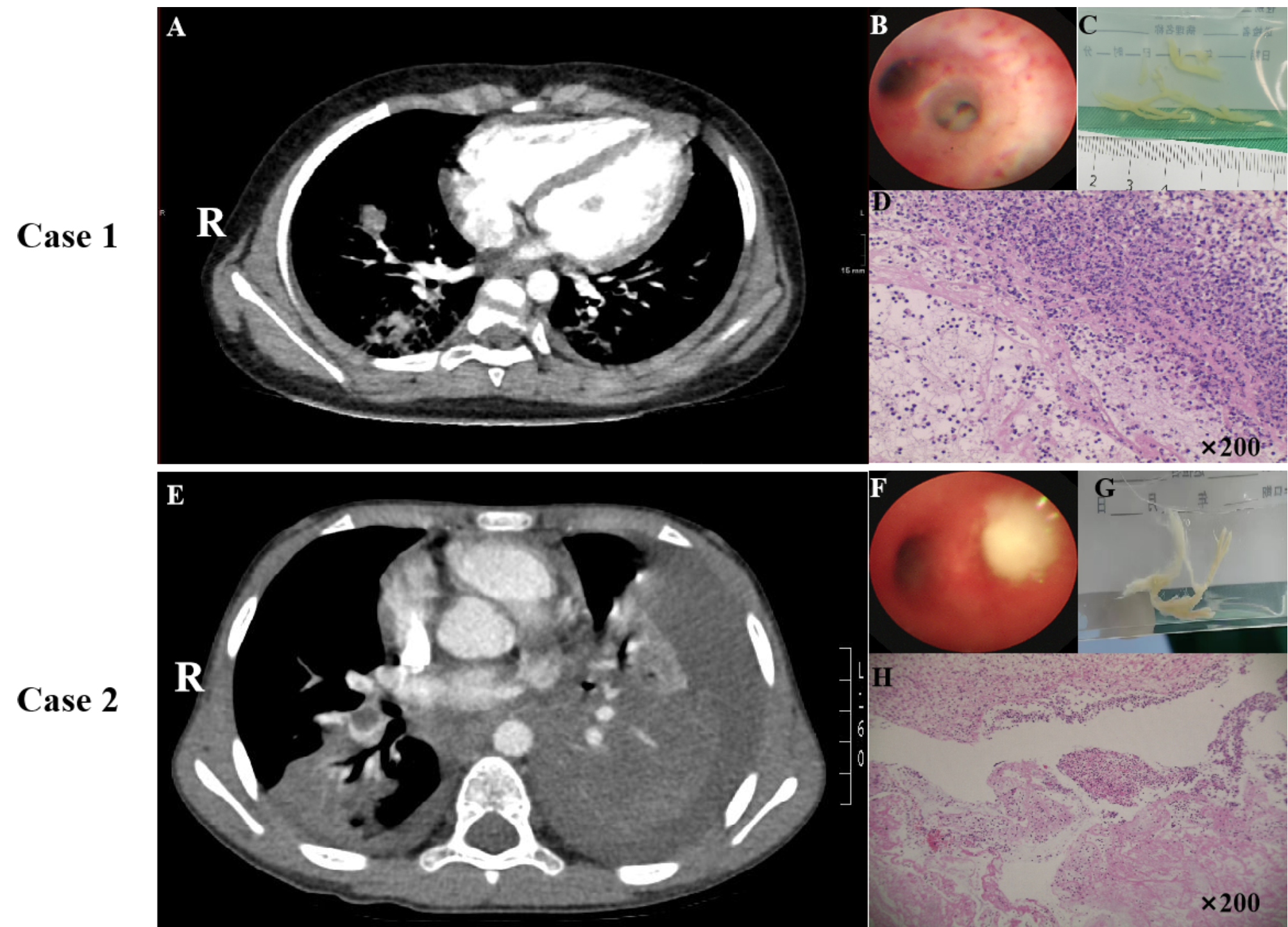
Diquat (DQ) is a non-selective, fast-acting biocidal herbicide and a paraquat co-pyridine. No antidotes are currently available to treat patients suffering from DQ poisoning, and available treatments remain limited in efficacy such that the case fatality rate remains relatively high.After 2 h of ingestion, diquat concentrations can reach peak blood levels [1]. In this report, we discuss two cases of DQ poisoning in children admitted to the Second Hospital of Lanzhou University. These children were provided with rapid treatment, but in Case B the child was not provided with hemoperfusion in a timely manner and presented with obvious abnormalities. Otherwise, the treatment path for both children was quite comparable, but the follow-up imaging and laboratory testing conducted for Case B revealed pronounced abnormalities. Studies have demonstrated that hemoperfusion effectively removes diquat from the bloodstream [2]. However, there are few reports on whether prompt and early renal support therapy (e.g., hemoperfusion) in the setting of diquat poisoning has a protective effect on organ function damage. This report provides a summary of our experiences diagnosing and treating these children, together with recommendations for the diagnosis and treatment of DQ poisoning in children in an effort to improve their prognostic outcomes.
Diquat (DQ;1,1’-ethylene-2,2’-bipyridinium ion) is a bipyridinium herbicide with the molecular formula C12H12Br2N2-H2O. This broad-spectrum fast-acting herbicide can non-selectively kill stems and leaves on contact. It is hydrophilic and a pesticide with moderate toxicity. When ingested, DQ can rapidly disseminate systemically through the bloodstream, accessing tissues other than the brain and spinal cord [3]. The half-life of DQ ranges from 2 days in the air to 2–10 days in the water and 3450 days in the soil [4], and exposure can cause toxicity, fetal malformation, and other forms of reproductive toxicity in mammals [5–6].
Wilks et al. classified the severity of DQ poisoning based on the ingested dose as follows: (1) Mild poisoning [ingestion of < 1 g of diquat cation, such as < 0.35mL of a 20% solution (100 g dibromide salt / 500 ml)], resulting in gastrointestinal symptoms and potential renal insufficiency that are reversible; (2) Moderate to severe poisoning (ingestion of 1–12 g of diquat cation [9.36-112.2mL]), resulting in multi-organ dysfunction characterized by prominent renal failure from which approximately two-thirds of children can recover; (3) Fulminant poisoning (ingestion of > 12 g of diquat cation, tor > 112.2mL of a commercial preparation), resulting in rapidly progressive multiple organ failure and death within 24–48 h. The World Health Organization’s International Programme on Chemical Safety defines the lethal dose of DQ as 6–12 g, and DQ poisoning-associated mortality rates are significantly positively correlated with the ingested dose.
In 2018, the European Union decided not to approve DQ and most developed nations curtailed or eliminated the use of this herbicide. However, in developing nations including China, it remains in widespread use, and cases of DQ poisoning in children are rarely reported. After the banning of paraquat in China in 2016, DQ emerged as the most prominent herbicide used in agricultural settings and the number of DQ poisoning cases rose annually. However, the Codex Committee on Pesticide Residues (CCPR) exhibited a lack of toxicological data pertaining to diquat dipyridone [7]. In patients admitted to the hospital, it is vital to assess the type and concentration of DQ in the urine or plasma. DQ poisoning cases are also typically concentrated in rural areas, however most developing countries’ county hospitals and community hospitals generally lack sufficient testing for poisons and nowadays guidelines regarding the treatment of these poisoning cases are lacking. Clear laboratory results cannot be given, and clear indicators for performing hemoperfusion are lacking.
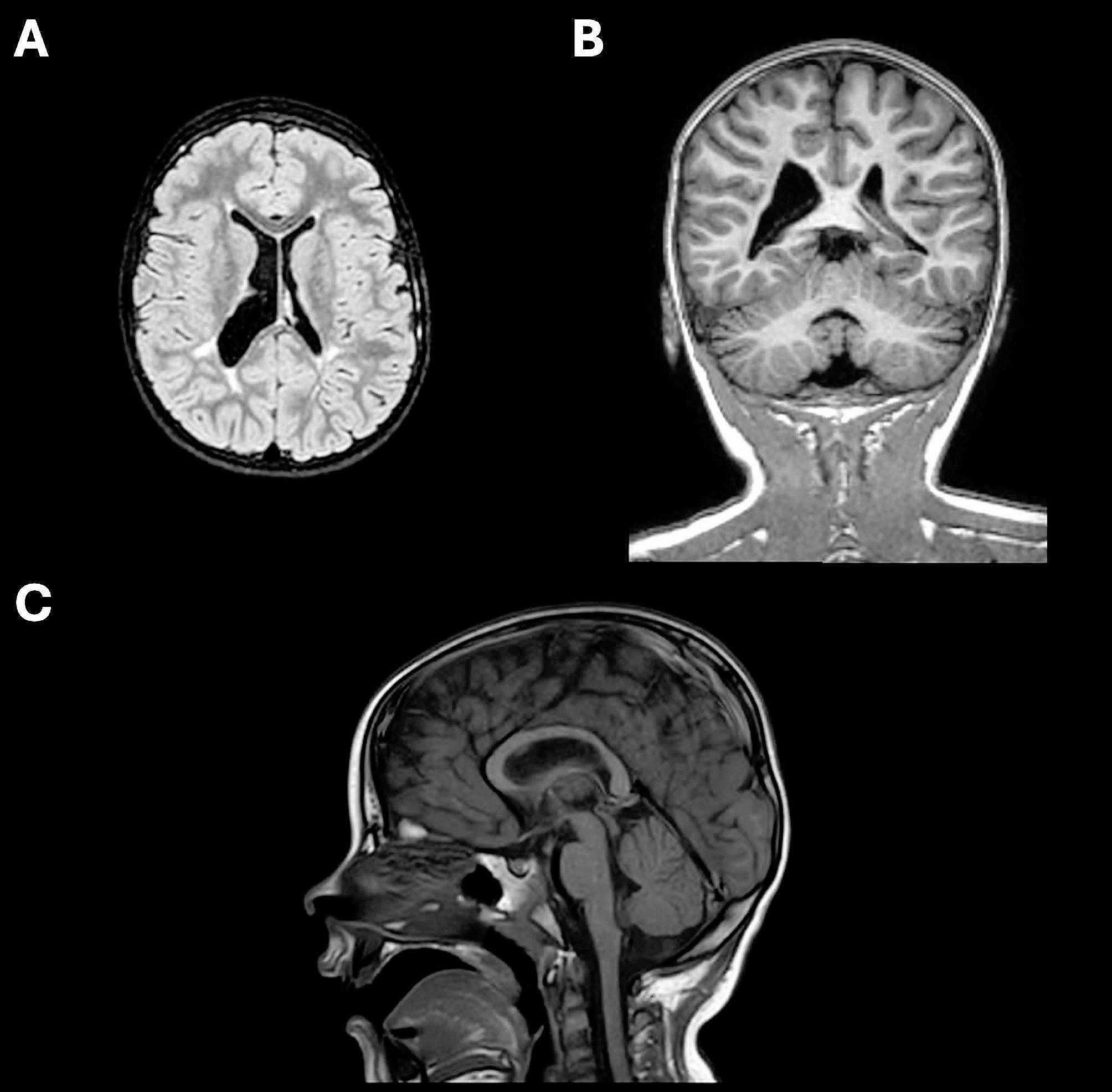
DQ absorption can occur through the digestive or respiratory tract, or via the ocular or mucocutaneous routes, and there have also been reports of poisoning via intramuscular, subcutaneous, and vaginal contact [8–9]. While the rate of DQ absorption via the digestive tract is low, it can be rapidly distributed throughout the body and accumulate in the liver, kidney, gastrointestinal tract, and lungs, reaching peak levels within 2 h and then rapidly decreasing in concentration [4]. Approximately 90–95% of DQ is excreted in the feces in an unmodified form within 24 h, while DQ and its metabolites that are absorbed into the blood are primarily excreted in the urine within 48 h in a manner unrelated to the route of exposure [9–10]. Following poisoning, DQ can cause damage to the liver, kidneys, and lungs, in addition to causing reproductive toxicity [5]. It can even cause the onset of toxic encephalopathy [11]. However, DQ enrichment in the lungs does not occur rapidly such that there is a lag period before DQ-induced pulmonary injury caused by redox reactions [12]. DQ poisoning generates oxygen radicals that contribute to membrane lipid peroxidation and cell death. There have been reports suggesting that dynamic changes in neutrophil and white blood cell counts can help predict survival outcomes in affected patients [13], as in the hemodynamic monitoring performed for Case B in the present report.
Several different mechanisms of DQ poisoning have been proposed. For one, DQ can induce oxidative stress via the dysregulation of normal redox processes, contributing to cellular and mitochondrial dysfunction [14]. In addition, DQ can cause neurodegeneration as evidenced by the axonal degeneration and pontine demyelination evident in some patients. Although the specific mechanism is unknown [15–16], neurological damage has repeatedly been reported [17], with some studies suggesting it is associated with neurodegenerative Parkinson’s disease owing to > 80% reductions in dopamine uptake [4], as these reductions are DQ dose-dependent [14]. DQ can also induce the apoptotic death of exposed cells [14]. There is also strong evidence for the ability of DQ to cause gastrointestinal damage, with one report having demonstrated ht that the chronic intake of low DQ doses resulted in low levels of intestinal inflammation and a corresponding increase in small intestinal activity [18]. Different treatments can be administered based on the mechanistic basis for DQ poisoning. For example, N-acetylcysteine, reduced glutathione, vitamin C, melatonin, and/or melatonin can be administered to mitigate oxidative stress, while symptomatic supportive care is provided in other cases, with a clear time for the application of renal support therapy not yet having been defined.



留言 (0)