Inclusion and exclusion criteria
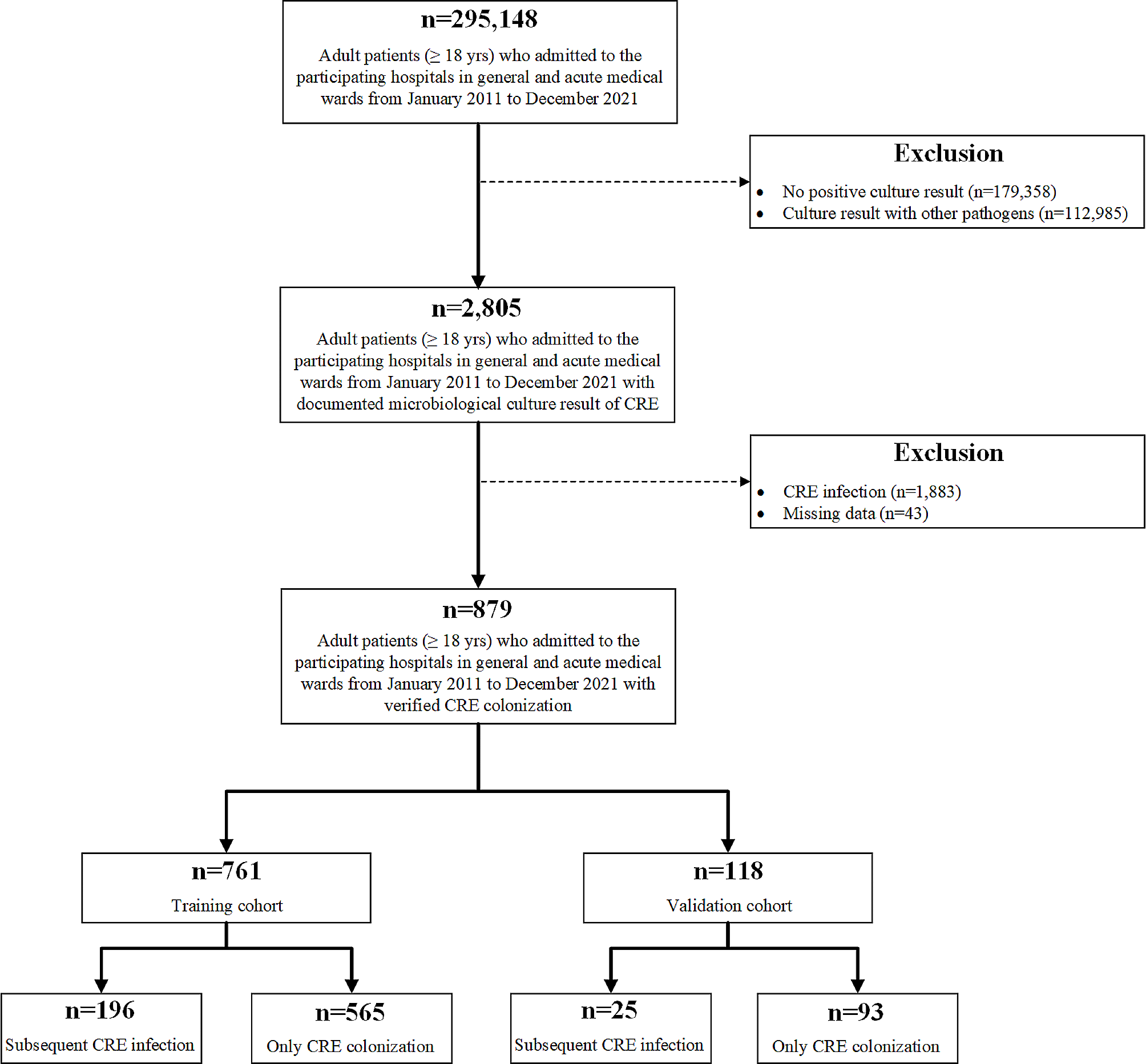
Inpatients who tested positive for COVID-19 according to nasopharyngeal swab PCR between January 1 and July 31, 2023 in a tertiary hospital in China were included. This hospital serves a population of more than nine million people and provides tertiary referral services to the surrounding regions. The exclusion criteria were as follows: [1] patients under 18 years of age [2], had a hospital stay less than three days, and [3] repeated patients.
Definitions
According to the CDC/NHSN surveillance definition, healthcare-associated infections, also known as hospital-acquired infections, occur while receiving health care in the healthcare facility or hospital, are usually acquired ≥ 48 h after admission, and are not present or might be incubating on admission [21,22,23,24,25,26].
Healthcare-associated bacterial/fungal coinfections among COVID-19 inpatients: COVID-19 inpatients with signs of bacterial or fungal infection that develop 48 h after admission and have positive cultures are considered healthcare-associated bacterial/fungal coinfections. Our study excludes community-acquired infections [8].
Neurological diseases refer to disorders affecting the brain, spinal cord, and nerves throughout the body, including Parkinson’s disease, Alzheimer’s disease, multiple sclerosis, stroke, epilepsy, migraines, neuralgia, and various types of brain and spinal cord injuries.
Study design and data collection
We have a real-time healthcare-associated infection surveillance system to monitor infections closely. Inpatients’ clinical information is recorded in the real-time surveillance system where clinicians and infection prevention and control professionals (IPCs) could receive early warnings about infections such as fever(> 38℃), elevated inflammatory markers(WBC or neutrophil count, PCT, IL-6, CRP), chest CT showing inflammation, antibiotic use or escalating antibiotic use, and positive cultures. Microbiological isolation is mandatory to confirm a bacterial/fungal infection. According to the symptoms and signs of the patient, clinicians will collect the specimens from suspected infection sites for etiological cultures, such as blood, urine, bronchoalveolar lavage(BAL), sputum, pleural fluid, ascites, and other specimens. Clinicians will diagnose and report healthcare-associated bacterial/fungal infections to the surveillance system. Meanwhile, IPCs will review medical record information to verify the occurrence or absence of infections. In summary, whether a healthcare-associated bacterial/fungal infection has occurred will be determined according to the symptoms and signs of patients and the culture-positive results of the suspected infection site. Based on the real-time surveillance system and microbiology culture, we can identify healthcare-associated bacterial/fungal infections as much as possible.
In this retrospective, single-center cohort study, data including demographic information, comorbidity information and laboratory results at admission were collected directly from the surveillance system. All predictive factors in our study preceded the outcome instead of a random point during the hospital stay. We also collected treatment information such as operation history, invasive ventilation, urinary catheter, meprednisone, dexamethasone, and tocilizumab before the infections occurred.
Data processing and statistical analysis
All the data processing and analysis were conducted using R (version 4.3.0). Missing value were processed for weight (n = 477,26.83%), height (n = 387,27.77%), white blood cell count (n = 6,0.34%), lymphocyte count (n = 9,0.51%), PCT(n = 481,27.05%), CRP(n = 66,3.71%), IL-6(n = 561,31.5%), neutrophil (n = 6,0.34%), albumin(n = 40,2.25%), hemoglobin(n = 9,0.51%), creatinine(n = 82,4.61%), and glucose (n = 6,0.34%) according to multiple imputation method and were conducted for five imputations.
Continuous variables are reported as the medians and inter-quartile ranges (IQRs) and were compared using the Kruskal-Wallis test. Categorical variables are reported as counts and percentages and were compared using the Chi-sq or Fisher’s exact test. We conducted univariate and stepwise multivariate logistic regression analyses to investigate risk factors for healthcare-associated(HA) bacterial/fungal infection. Factors with a P-value less than 0.05 were independently associated with HA infections. Adjusted odds ratios (AORs) and 95% confidence intervals (95%CIs) were estimated.
Model development and internal validation
We randomly divided all the samples into a training set and a testing set at a ratio of 7:3. The training set was used to screen variables and develop models, while the testing set was used for model evaluation. We selected variables for the model development which were statistically significant in our univariate analysis. The models included 14 candidate predictors, as follows: diabetes, kidney disease, neurological disease, ICU admission, PCT_level, albumin (ALB_level), creatinine (Cr_level), IL-6_level, CRP_level, neutrophil percent (Ne_level), central venous catheter (CVC), urinary catheter (UC), invasive ventilation (IV), and dexamethasone (DXM). The variance inflation factors (VIF) were calculated to assess the multicollinearity of the predictors. As all the predictors had a VIF less than 2, indicating no multicollinearity, all the predictors were included in the model development.
A random forest model was established (ntree = 500, mtry = 4) and the importance of the variables was determined. Our study compared the discrimination of models by the area under the receiver operating curve (AUCROC). The calibration slopes were calculated to check the risk of overfitting. Decision curve analyses were performed to evaluate whether the risk models improved clinical decision-making [27].




留言 (0)