
記住我



The characteristics of LTCFs of both groups are summarized in Table 1.
During the study, 326 UTI episodes were recorded, 161 in the intervention group and 165 in the control group. In the pre-intervention phase, we recorded 71 UTI episodes. During the intervention and post-intervention period, 167 and 88 episodes were documented, respectively. In the control group, 55/165 (33%) of UTIs were recorded in patients with an indwelling urinary catheter compared to 22/161 (14%) in the intervention group (p < 0.004). There was a statistically significant difference in the method of communication between LTCF and physicians. In the intervention group, the physician was present at the LTCF in 26/161 (16%) of cases of UTI compared to 72/165 (44%) in the control group. In contrast, physicians were contacted by phone or fax 135/165 (84%) in the intervention group and in 93/165 (56%) in the control group (p < 0.001).
Patient characteristicsUTIs were diagnosed in 194 patients. There were no significant differences between the study populations, i.e. patients with UTIs, in terms of age, sex, history of allergies to antimicrobial substances, history of renal impairment or urologic diseases (Table 2). There was a statistically significant difference in reported weight (control group median 66 kg (range 38–135 kg) vs. intervention group median 59 kg (range 38–143 kg), p = 0.014).
Intervention reachDuring the intervention period (April 12, 2021– November 3, 2021), 30 onsite trainings were conducted by ICP team. Overall, 209 nursing staff members took part in these trainings. On October 31, 2021, the number of nursing staff employed by the four LTCFs of the intervention group was 205. The discrepancy between team members who took part in the trainings and the number of employees as of October 31, 2021 can be explained by staff turnover. All physicians received written information about the project during their visits at the LTCFs including the guideline and information on the website at five time points throughout the study. They were invited to the online educational sessions on the UTI program. Half of the physicians (15/ 30) attended at least one of the online sessions.
Primary outcomeInter-reviewer consistency was high for the primary outcome (ĸ = 0.98; 95%CI 0.96-1.00). Out of 326 UTI episodes 323 (99.1%) were evaluated the same. Only in three UTI episodes discordant evaluations were observed. Due to the high level of agreement between the two reviewers, the two evaluations were combined for analysis. Therefore, adequate prescription was defined as follows: both reviewers evaluated the prescription adequate.
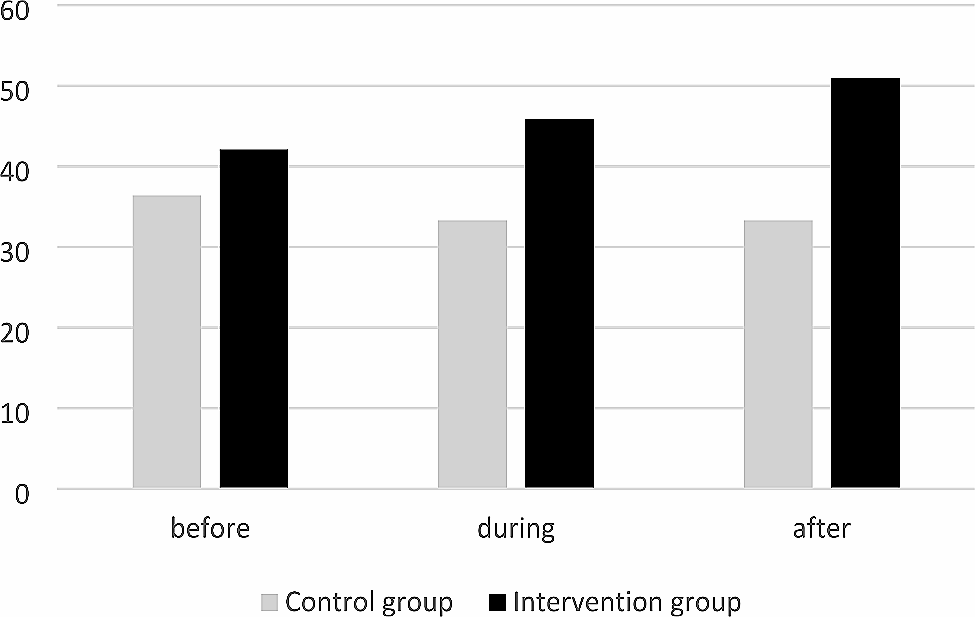
In the intervention group, the proportion of adequate antibiotic choices increased from 42.1% in the pre-intervention period, to 45.9% during the intervention and to 51% in the post-intervention period (absolute increase of 8.9%). In the control group, the proportion was 36.4%, 33.3% and 33.3%, respectively (Fig. 1). Therefore, the numerical difference between intervention group and control group in the post-intervention period was 17.7%. However, the differences between intervention group and control group did not reach statistical significance (Tables 3 and 4).
Table 4 Summary of results (raw numbers and proportions)Fig. 1
Proportion of adequate antimicrobial treatments (adequate in terms of choice) before, during and after interventions
Secondary outcomesBecause agreement in secondary outcomes was also high (ĸ = 0.97; 95%CI 0.93-1.00; concordant evaluations: 99.1%) the two evaluations were combined for analysis in the same way as for the primary outcome. During the intervention period, the risk ratio (RR) for inadequate indication for treatment was 0.41 (95% CI 0.19–0.90), p = 0.025 (Fig. 2; Table 3). In the post-intervention period, there was no difference between intervention group and control group, due to an increase in adequate indications for treatment in the control group (from 72.0% in the intervention period to 89.7% in the post-intervention period).
Fig. 2
Proportion of adequate antimicrobial treatments (adequate decision to treat) before, during and after the interventions. *p < 0.05 comparing intervention and control group during the intervention period
During the study, 227 (69.6%) UTI episodes without an indwelling urinary catheter were recorded, 133 in the intervention group and 94 in the control group. Before and after the intervention period, the risk ratio (RR) for use of quinolones for UTI without indwelling urinary catheters were significantly reduced (RR: 0.17, 95%CI: 0.04–0.72; and 0.18; 95%CI: 0.04–0.89, respectively. Tables 3 and 4).
During the study period, 28 (8.6%) urinary cultures were performed (326 UTI episodes recorded). Throughout the study, more urinary cultures were ordered in the IG compared to control group. This difference was statistically significant during the intervention period (RR 6.89, 95%CI 1.59–29.83, p = 0.010, Table 3). In the post-intervention period, a statistical analysis was not possible as no cultures were performed in the control group (compared to 7 in the intervention group).
Our safety outcomes were: proportion of clinical failure (defined as need for additional antimicrobial treatment for UTI within 7 days of previous episode), number of hospital admissions due to UTI and adverse events due to antimicrobial treatment. There were no significant differences between the control group and intervention group in the safety outcomes (Tables 3 and 4). Only one adverse event due to antimicrobial treatment was documented during the entire study period (in the intervention group in the pre-intervention period).
留言 (0)