This study described a region-wide assessment of the level of implementation of multimodal IPC practices among 42 acute-care hospitals of Northern Italy. A standardized questionnaire based on the WHO IPCAF Core component 5 was employed, for which a significant correlation with HAI prevalence was found.
In Italy, antimicrobial resistance (AMR) is a relevant health concern [1, 12]. To address this issue, two Italian National Action Plans to contrast AMR (PNCAR) were issued, in 2017 and 2022 [17, 18]. IPC and HAI surveillance are included among strategic objectives of both plans, and together with appropriate antibiotic use are recognized as the three pillars sustaining the national strategy and coordinated governance of the latest PNCAR.
As the Italian national health system is decentralized, the provision of healthcare within each of the 21 Regions of Italy, including the local implementation of the PNCAR, is consigned to Regional Health Authorities [11]. In the Region of Piedmont, a series of policy measures, quality-driven strategies, and an indicator-based performance evaluation program have been employed to promote surveillance of HAIs and strengthen IPC activities since 2008, within a regional framework. Performance indicators are updated each year by a multidisciplinary working group, and have been targeted towards the objectives outlined in the PNCARs since 2018.
Several aspects of IPC programs have been assessed through the regional indicator system throughout the years, however multimodal strategies, a relatively novel concept, had not yet been systematically investigated. The WHO IPCAF is based on evidence-based guidelines for the implementation of Core components of IPC [19]. Importantly, an inverse correlation between a score based on Core component 5 and HAI prevalence was found in this study, supporting the relevance of the multimodal approach and the validity of the IPCAF score in measuring IPC programs, in terms of effectiveness of preventing HAI transmission.
Our study found a high overall level of implementation of multimodal strategies for IPC (median score 11/14), with the majority of facilities implementing all elements defined by the WHO. Previous evaluations performed in Germany, Austria, and Korea found lower scores for multimodal strategies compared to those assigned to other Core components, leading the Authors to conclude that efforts to strengthen IPC in high-income countries should place further focus on multimodal strategies [20,21,22].
However, in our Region safety climate and culture of change and system change were identified as areas for improvement. Further efforts should be directed towards empowering teams and individual healthcare professionals so that they perceive ownership of interventions. This issue is particularly relevant in our country, given the lack of accountability and tendency by several stakeholders to avoid taking charge recognized by the ECDC in their country visit to Italy to discuss AMR [23].
According to results of our study, IPC staffing levels are in line with minimum requirements defined by the WHO [24], and the number of IPC doctors and nurses per 1000 beds have slightly increased since the previous edition of the PPS conducted in Piedmont [25]. The majority of hospitals indicated their participation in surveillance networks coordinated within the regional framework: namely surgical site infections, antibiotic resistance, and antibiotic use. A lower degree of participation was found for surveillances outside this system, such as C. difficile infections.
Alcohol-based handrub consumption has considerably increased, from a median of 11.1 L per 1000 PDs in 2016 to 24 in the current study [25]. This finding is in line with previous national and international reports of increased consumption of alcohol-based handrub following the COVID-19 pandemic, however efforts should now be dedicated to maintaining high consumption levels beyond the pandemic context [26, 27]. Interestingly, a multimodal approach to promoting hand hygiene practices was adopted by our region, in line with WHO guidelines and through the Hand hygiene self-assessment framework (HHSAF) proposed by the WHO, which has been included among performance indicators of our region since 2014 [28].
Concerning patient-level data, a HAI prevalence of just over 8% among non COVID-19 patients was identified in this study, which was similar to results of the previous edition of the PPS in Italy (8.03%) and in our region (7.26%), even though patients were slightly older in the current edition [7, 25]. As in the previous edition, the most frequent HAI types were pneumonia, UTIs, and BSIs. In light of the high level of implementation of IPC practices, further research is necessary to evaluate possible explanations for the lack of improvement in HAI prevalence, such as changes in patient case-mix or the impact of the COVID-19 pandemic on HAI transmission.
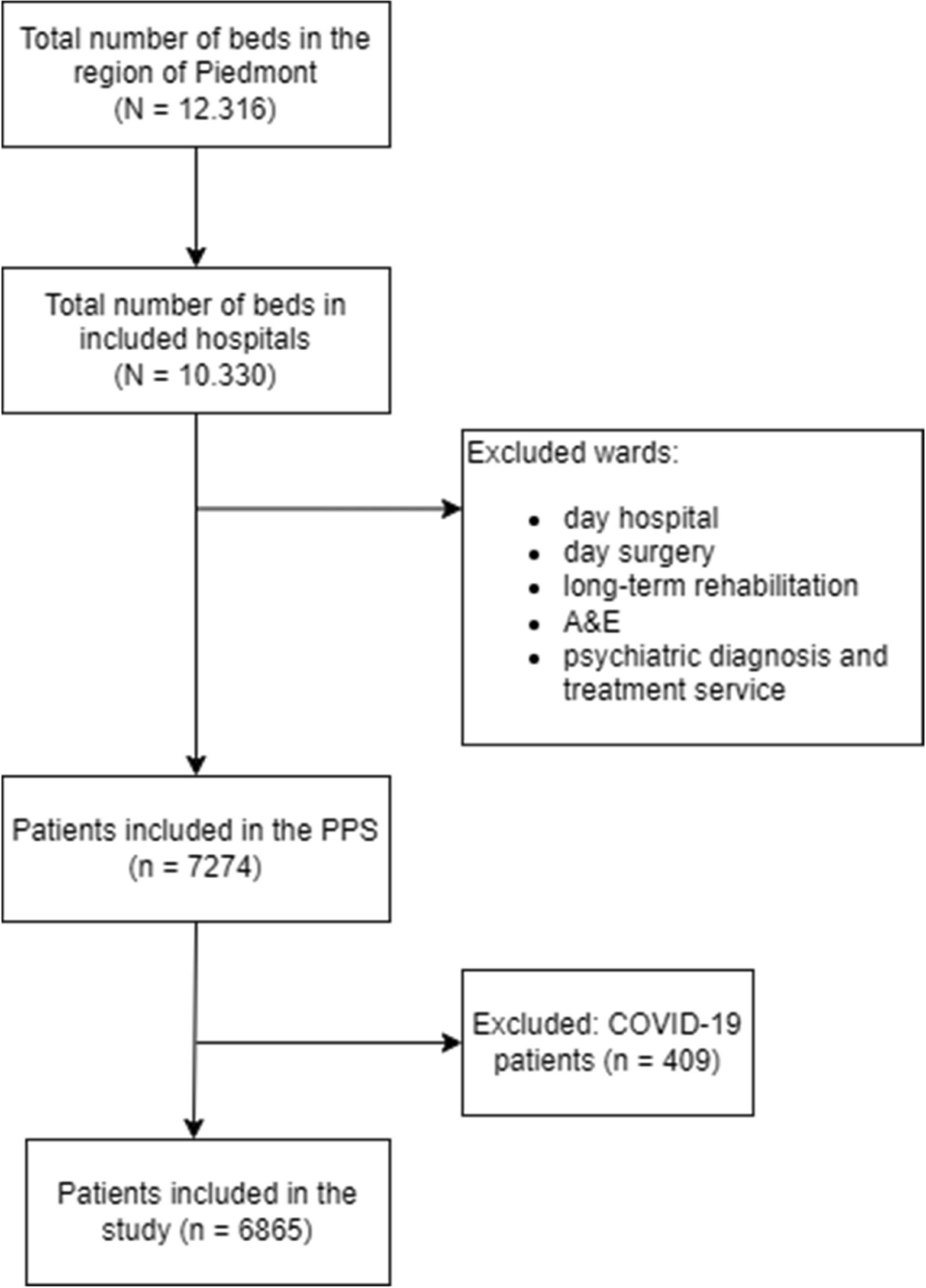
Several limitations should be considered when interpreting results of this study. First, as participation in the PPS was voluntary, hospitals with higher interest in IPC could be overrepresented. Further, the study mainly focused on public hospitals, with a low participation among private and not-for profit facilities (Table 2). However, as shown in Fig. 1, participation in the PPS accounted for over 50% of total acute-care beds. Second, limitations due to study design apply: we did not attempt to determine causal relationships between variables as point data were collected. Third, data were self-reported, and only patient-level variables were validated. A validation survey according to the ECDC PPS 2022–2023 Validation Protocol Version 4.0 was performed among 50 patients of one facility of the Region, which found a sensitivity and specificity in identifying HAIs of 85.71% and 95.45% respectively. Validation was not performed in regards to the IPCAF questionnaire. Concerning the IPCAF questionnaire in particular, a high degree of understanding of the underlying concepts and definitions was required in order to accurately perform facility assessment, therefore we cannot exclude that certain elements may have been misunderstood or that self-reported results may have been distorted by a degree of reporting bias. Finally, as the primary purpose of the IPCAF is self-assessment, and health system structure, policy, and organization could influence implementation levels, we would caution against international comparisons of results.
In conclusion, through this study a baseline assessment of IPC activities in our region was performed, which allowed us to document strengths and areas for improvement. This first assessment will hopefully be useful to define priorities for action and tailored improvement strategies, in particular considering the high prevalence rates for HAI found in our region. Results of this study provide standardized reference data for benchmarking; repeated monitoring and evaluation could help sustain progress over time [19, 29].




留言 (0)