Neonatal teach clean training intervention
TEACH CLEAN is an education intervention aimed at improving environmental hygiene by training cleaning staff, with an initial focus on maternity units in low-resource settings. It was made publicly available in 2018 after piloting in The Gambia, India, and Cameroun and evaluation in Tanzania [7]. Key features of the training materials include participatory methods and pictorial guidelines to facilitate learning for cleaners with low education and literacy levels [15]. At the time of TEACH CLEAN's release, no training programmes were available for this cadre. This programme has since been adapted and used in many low-income countries and was recently adopted by the WHO as the basis for their own cleaners’ training resources [16, 17]. The TEACH CLEAN program consisted of seven modules covering crucial topics like personal hygiene, dress code, hand hygiene, PPE, housekeeping, waste handling, and linen handling. The program was designed to be taught by a designated trainer in the health facility, who was usually a healthcare professional in a leadership role in a clinical area. The trainer would receive training from a supervisor, also known as the 'master trainer,' from the district or regional level, using a "train the trainer" approach. In 2018, after the initial pilot of TEACH CLEAN, three additional modules were added to the original seven. These modules aimed to assist trainers and master trainers in learning to train, supervise, and establish quality improvement. In all applications of TEACH CLEAN and now the WHO resource, there is a crucial local adaptation phase when the generic guidance on frequency of cleaning and priority surfaces are contextualised to the specific healthcare setting, both to be consistent with existing IPC protocols in place and to allow for human resources availability. The adaptation is informed by the conduct of a local needs assessment exercise to identify existing practices, guidelines, previous training, numbers and literacy of cleaners, etc.
For the current study an additional training module was created for the original TEACH CLEAN package, focussing specifically on the peculiarities of surface cleaning in a neonatal unit. For ease of access, this is available in the Supplementary material for the paper. Healthcare professionals conducted local adaptation from a local NGO (Horizons Trust Gambia; HTG) that had previously worked with TEACH CLEAN. The participatory training included modules that covered not only cleaning practices for specific surfaces and preparation of cleaning fluids and materials but also priority surfaces for cleaning and frequency within a daily schedule. An additional module was prepared specifically for the neonatal unit, and it adapted the definition of the “patient zone” for the context of newborn cots. After the training, the cleaners were followed up with supportive supervision by the trainer and the senior staff in the neonatal unit. Pictorial guidelines on cleaning practices and frequency were also made available to them on the ward. These partners provided one master trainer to train four healthcare professionals from the neonatal unit to deliver the entire TEACH CLEAN package, plus the supplementary module for neonatal units. The training of cleaners from this clinical area was then conducted through workshops by the trainers at the participating hospital in October 2021. The master trainer from HTG also attended and provided further support to the trainers, particularly around supportive supervision, during the month after the cleaners’ workshop. According to the study design, the control (labour ward) did not receive training during the intervention. A similar training-the-training approach was delivered by HTG for the control ward after the data collection was completed. The same microbiological samples and qualitative data capture were conducted in the intervention (neonatal unit) and control (labour ward) areas.
Study design, setting and population
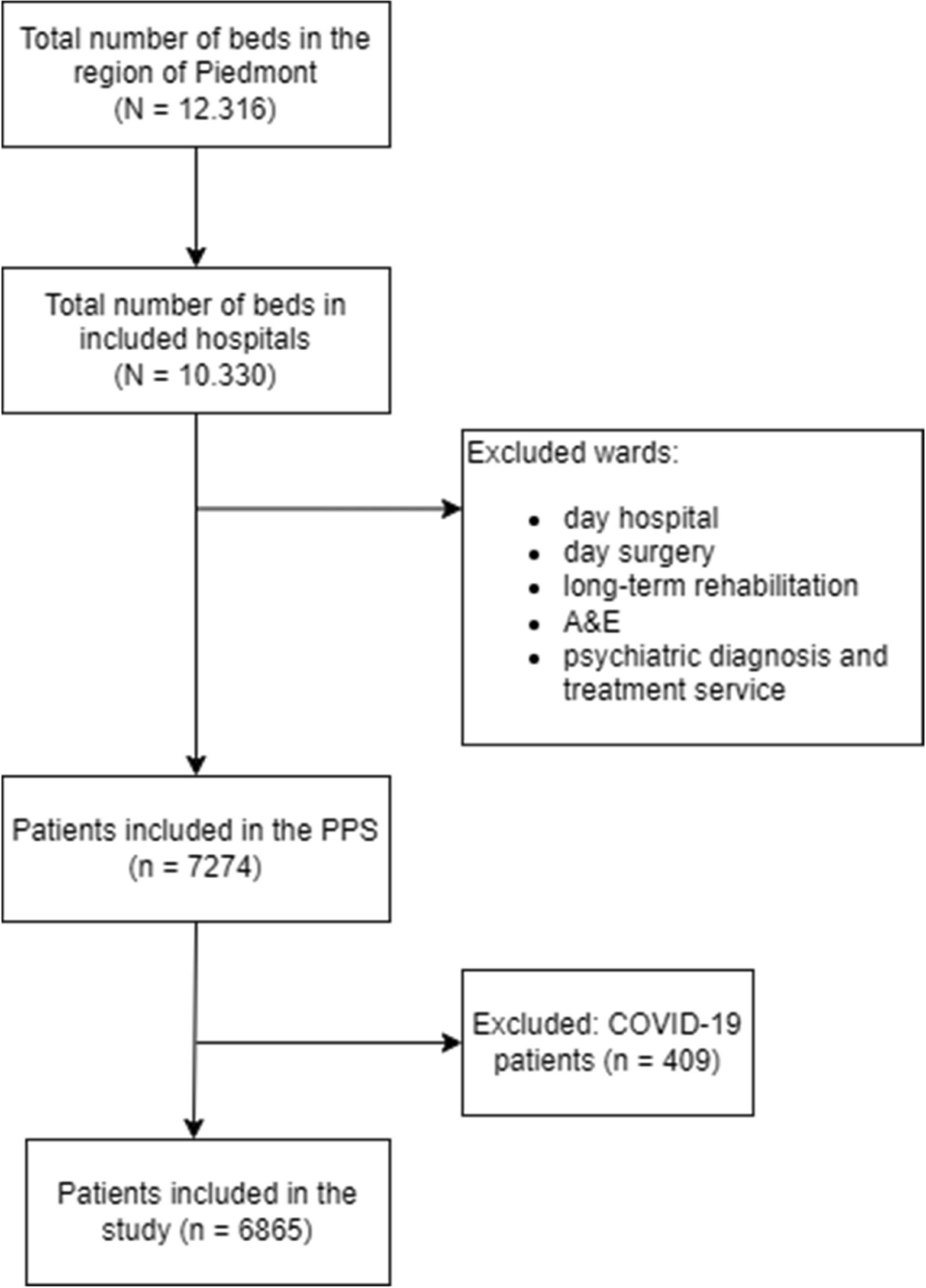
We conducted a mixed-methods study at the neonatal unit of a large government tertiary referral hospital in The Gambia, the Edward Francis Small Teaching Hospital (EFSTH). This work was conducted as a collaboration between the MRC Unit The Gambia at the London School of Hygiene & Tropical Medicine (MRCG at LSHTM), LSHTM and the Epidemiology and Disease Control Unit (IPC Unit) of the Gambian Ministry of Health. The EFSTH is the sole national teaching and tertiary government referral hospital of the Gambia. With approximately 3,000 deliveries per year, the maternity unit at EFSTH has the third-highest annual deliveries nationwide. The neonatal unit at EFSTH has 30 cots, including an acute care ward, two low-risk wards, and a Kangaroo Mother Care (KMC) ward with six beds. During peak admission periods, cot occupancy is often over 200%, since neonates share cots and incubators [18]. This pilot study focused on neonatal acute care, KMC wards, and the labour ward as a comparator area. Our quasi-experimental study design aimed to evaluate the impact of the training intervention on cleaning behaviour and techniques and surface microbiological cleanliness. We also collected qualitative data on health system barriers to ensuring environmental hygiene in the facility and the training experience.
Methods used to assess the adequacy of routine environmental cleaning
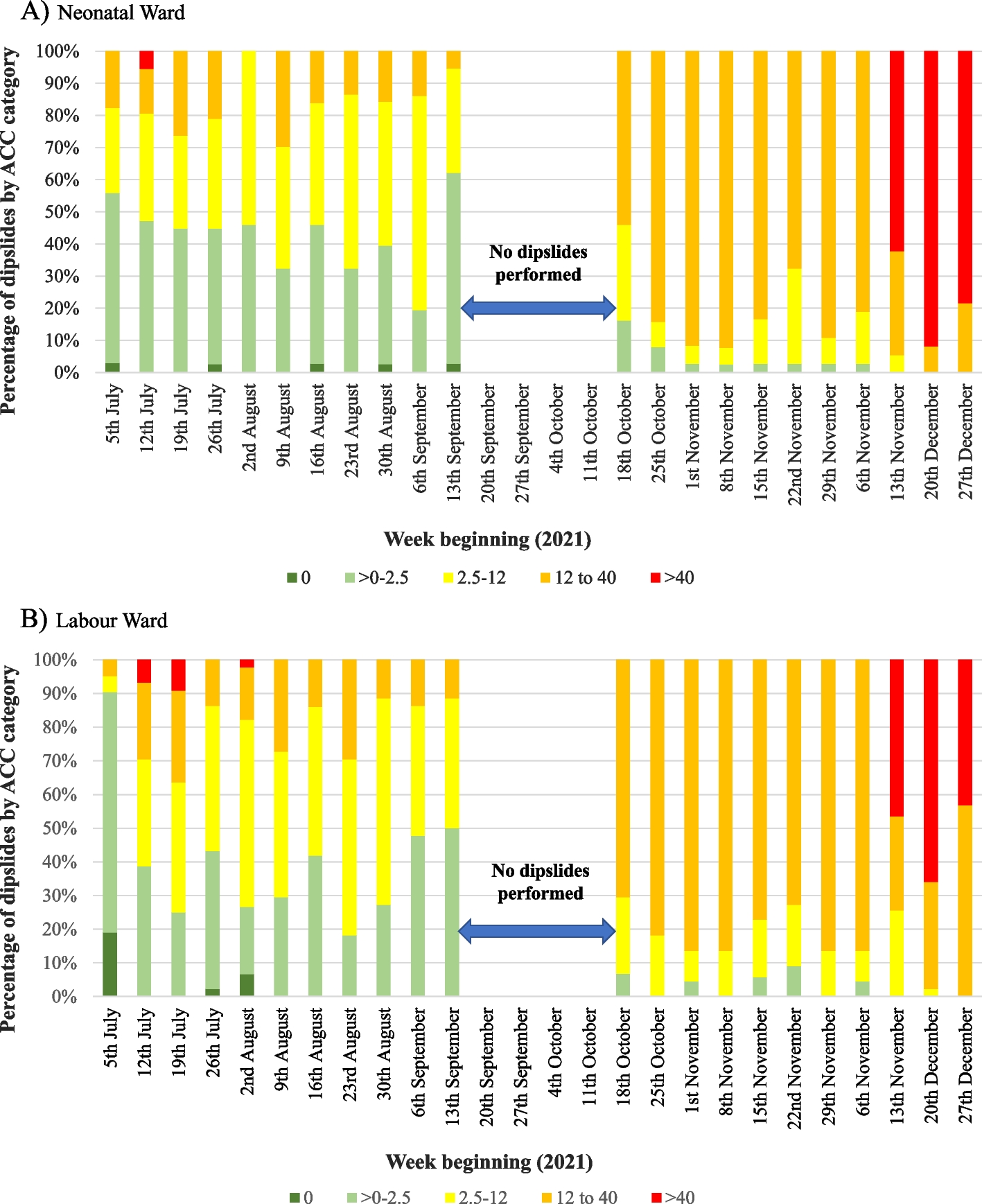
Throughout our study, we monitored the cleanliness of hospital ward surfaces weekly. To accurately measure aerobic colony counts (ACC) and identify Staphylococcus aureus, a key indicator pathogen for neonatal sepsis in sub-Saharan Africa [19], we utilized double-sided dipslides coated with nutrient and staphylococcal selective (Baird-Parker) agars. This was carried out during the baseline period (July to mid-September 2021) and post-training intervention period (mid-October to December 2021) in both intervention and control wards. Before collecting dipslides, we carefully observed hospital staff to determine which surfaces were the most frequently touched by healthcare workers. We then selected sampling locations in advance and created a list of key high-touch surfaces. Samples were taken from the same locations weekly but on a randomly selected day each week. (Supplementary Table A1). We tried to collect samples from equivalent positions of objects, especially cots and beds, every week, although there was some equipment movement around the ward between weeks. The same staff members took the samples weekly and were instructed to approach the sample collection consistently throughout the study. We ensured we did not leave any permanent marks on the objects while collecting samples. We followed the manufacturer's instructions for sample collection, after which dipslides were transported to the MRCG-at-LSHTM microbiology laboratory for processing. They were incubated aerobically at 40ºC for 48 h. Trained staff read dipslides and quantified aerobic growth as follows: 0 CFU/cm2; 0–2.5 CFU/cm2; 2.5–12 CFU/cm2; 12–40 CFU/cm2; ≥ 40 CFU/cm2; and confluent growth. To ensure accuracy, 10% of the dipslides were read by a second reader and 5% by a third reader, with any discrepancies re-evaluated. We searched for the presence of S. aureus based on colonial appearance and subculture on blood agar with a positive coagulase test (Pro-Lab Diagnostics, UK). Confirmatory testing for possible S. aureus was performed with a positive DNAse test. We classified this organism as either "present" or "absent" on each dipslide.
Observation of cleaning practice
A single data collector observed cleaning episodes once a week for 14 weeks in the neonatal unit (intervention) and labour ward (control) after the intervention. These observations were conducted early on Wednesday mornings to ensure consistency. We attempted to conceal the study's true purpose from staff by framing it as an assessment of overall care quality. We recorded various aspects of cleaning techniques, such as whether the cleaning staff covered all regions of the patient zone during the cleaning process, used a fresh cloth, and allowed the area to dry before use (Supplementary Table A2). The observation was explicitly concentrated on cleaning the patient zone, including the bed and other items designated for that area. It focussed on the same surfaces and practices each week.
Qualitative interviews and group discussions
We conducted key informant interviews with several individuals to gain insight into the factors affecting the cleaning of hospital wards. These included the chief matron, the matron responsible for the neonatal unit, the head of domestic services (also known as cleaners or orderlies), and the head of the hospital's IPC Unit.
Statistical methods
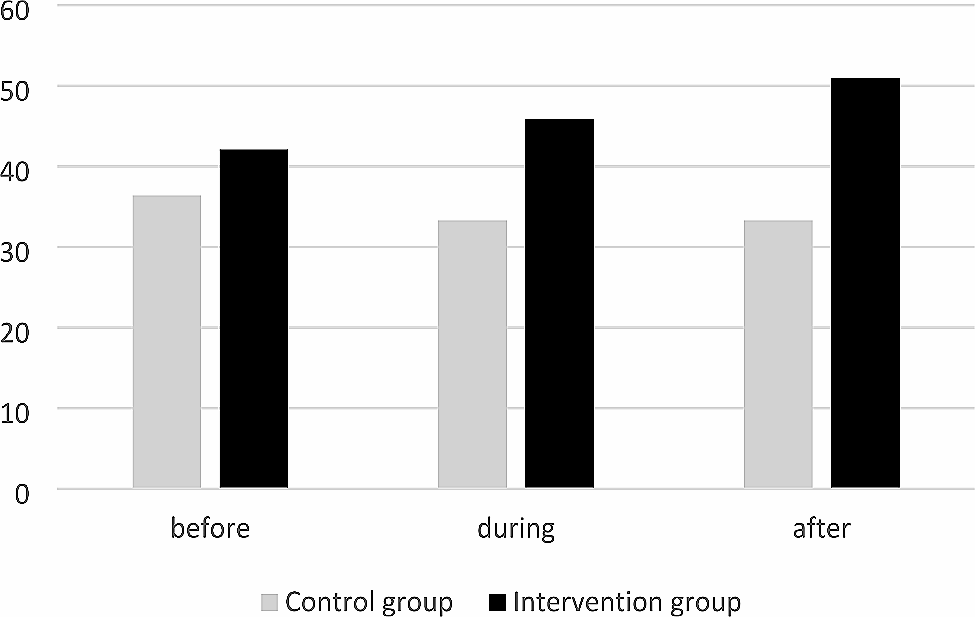
Based on previous work conducted in maternity wards in Tanzania, we anticipated that the training intervention would enhance the dipslide ACC "pass" rate from approximately 25% to approximately 50% [7]. The sample size used in this study had more than 99% power to detect a change in that scale. It was intentionally overpowered to detect changes in underlying trends, including the Hawthorne effect. The data were cleaned to ensure accuracy, consistency, and completeness before being analysed using Stata software. The degree of surface cleanliness was categorised into five groups following the laboratory classifications. Based on previous research, we also categorised the ACC results into "pass" for those below 2.5 CFU/cm2 and "fail" for those at ≥ 2.5 CFU/cm.2 [20]. Key informant interviews were recorded in English and one of the local languages (Mandinka) using a digital recorder. We used NVivo 12 software to manage and code transcripts of the audio recordings. The thematic analysis process involved several steps: familiarisation with the data by relistening to the audio recordings and/or re-reading the transcripts and observation field notes; initial coding and searching for themes; and review, definition, and naming of themes [21].




留言 (0)