
記住我



This study was conducted in the adult ICU of Geneva University Hospitals, a tertiary care hospital located in Geneva, Switzerland, with 10 sites, 2008 beds, and approximately 60 000 admissions per year. The adult ICU is a mixed medical-surgical ICU with a total of 32 beds and provides care for approximately 2500 patients annually with an average length of stay of 4 days. All adult patients (> 18 years old) with at least one stay in the ICU from January 1, 2016, to December 31, 2021, were included. All short-term CVCs in situ while the patient was in the ICU were included [10]. All long-term CVCs (e.g., Broviac®), peripherally inserted central catheters, dialysis catheters and arterial catheters were excluded. For validation of the algorithm, we used prospectively collected data from the routine surveillance program in place at the Geneva University Hospitals [11]. For more than 25 years, the Infection Prevention and Control (IPC) team has been conducting hospital-wide prospective surveillance of all healthcare-associated BSIs. For each healthcare-associated BSI episode, data on the source of infection and clinical and microbiological characteristics are routinely collected manually by the IPC team. The IPC team members are alerted to every new positive blood culture result by the central microbiology laboratory, and they prospectively follow-up and investigate the sources of healthcare-associated episodes. All episodes occurring more than 48 h after hospital admission or within 10 days of a previous hospitalization are investigated.
Data sources for the automated surveillance and the manual surveillanceFor the automated surveillance, patient-level data (age, sex, admission and discharge dates, mortality at day 30), individual-level CVC data (date of insertion and removal, ward of insertion, insertion site, and dwell-time) and microbiological data (blood culture results, other culture results, specimen collection dates) were extracted from the EHR. For the comparator (manual BSI surveillance), all BSI data were extracted from the hospital.
DefinitionsBSI were classified according to adapted ECDC definition criteria, as those used in the European point prevalence study [12,13,14]. The primary outcome, CRBSI, was defined as a BSI that occurred at any time point from the day of catheter insertion up to 48 h after catheter removal, and a blood culture result with the same microorganism as a quantitative CVC tip culture of 103 colony-forming units (CFU) per mL or greater [15] (or semiquantitative central venous catheter culture > 15 CFU) [12]. Of note, the following criteria were not included in the automated algorithm for CRBSI: (a) quantitative blood culture ratio CVC blood sample/peripheral blood sample > 5; (b) differential time of blood culture positivity (DTP); (c) positive culture with the same microorganism from pus at the insertion site and (d) clinical criterion of improvement within 48 h of catheter removal. Criteria (a) and (b) were not implemented in the automated algorithm because they were not systematically provided by our microbiology laboratory. Only CRBSI episodes that started 48 h after ICU admission were considered (the initial positive blood culture of the episode was collected after the patient has spent a minimum of 48 h in the ICU).
Secondary outcomes included CLABSI and ICU-onset BSI. CLABSI was defined as a BSI that occurred from day of catheter insertion until 48 h after catheter removal, with the absence of positive culture from other specimens with the same microorganism within an interval of 72 h before/after the first positive blood culture of the episode. This rule was not applied if the microorganism was a common commensal, even though the rule to classify a common commensal as a true pathogen was fulfilled. The types of other specimens considered were restricted to urine, respiratory tract, bone and joint, abdominal, and central nervous system specimens (full list provided in Appendix, Suppl Table 1) based on previous work performed by our group [16]. Only BSI episodes that started 48 h after ICU admission were also considered. Finally, ICU-onset BSI was defined as a BSI episode for which the first positive blood culture of the episode was collected after the patient has spent a minimum of 48 h in the ICU, regardless of the presence of a CVC.
A common commensal was considered as a true pathogen when the same common commensal was present in at least 2 positive blood cultures within 48 h. Common commensal included, among other, coagulase-negative staphylococci, Bacillus species, Propionibacterium species, Corynebacterium species, or Micrococcus species (as defined by the CDC NHSN [“NHSN Organism Category”] [17]).
A BSI episode was defined as any positive blood culture with the same pathogen within a time-window of 14 days (counted in hours). To limit complexity, polymicrobial blood cultures were considered as separate episodes. Negative blood cultures were not considered to define an episode. A set of blood cultures (two vials) was counted as one blood culture. Catheter days were counted in hours. CVC days of two or more concurrent CVCs were all counted. Catheter insertion and removal dates were replaced with ICU admission and discharge dates, respectively, when missing.
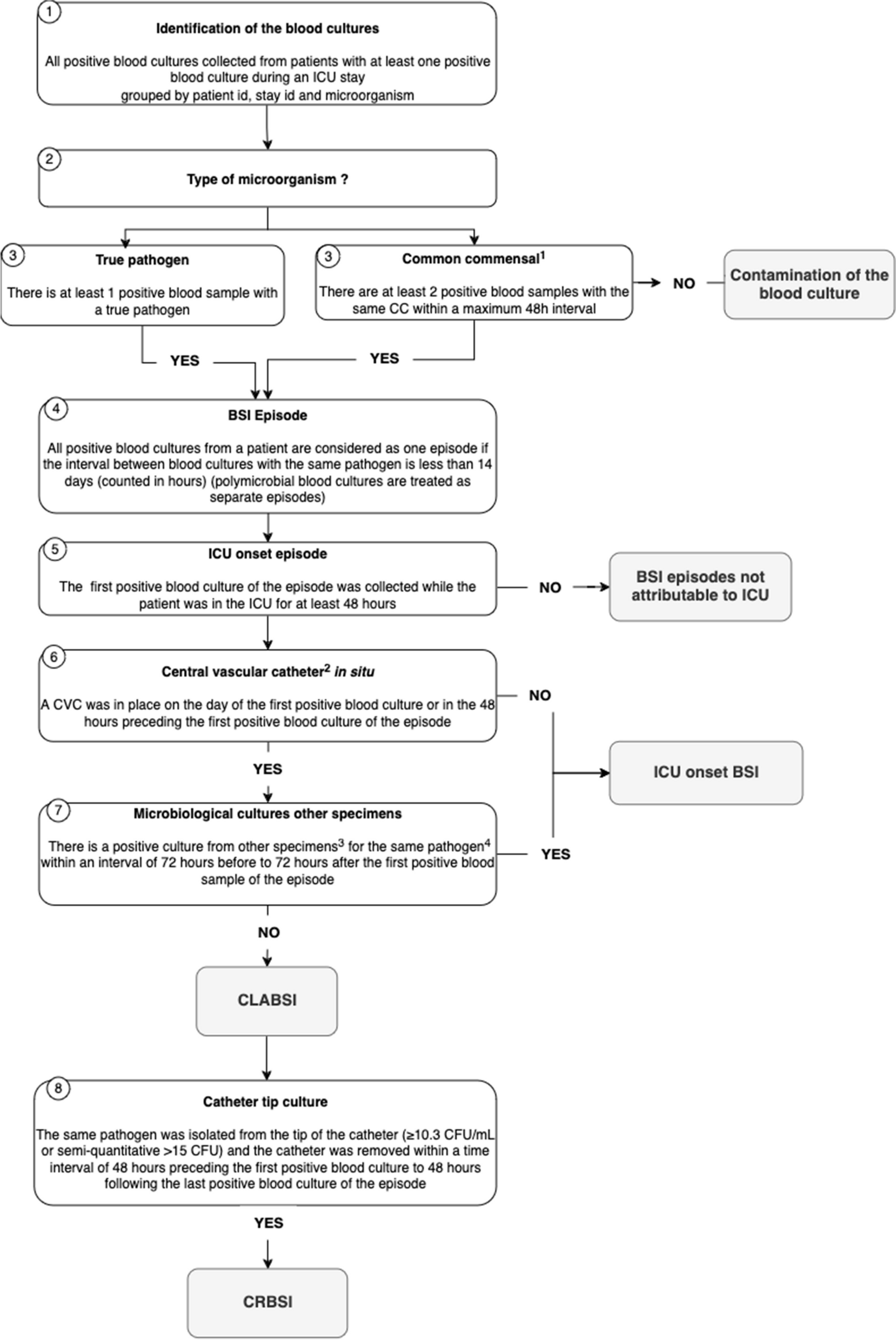
Development of the fully automated algorithmThe IPC team in collaboration with an information technology (IT) team developed a fully automated algorithm for CLABSI/CRBSI detection (Fig. 1), which was based on a systematic review, meta-analysis and meta-regression that identified relevant parameters to be implemented [16]. The algorithm was built through an iterative process with a regular manual check using clinical use cases for each parameter of the algorithm.
Fig. 1
Fully automated algorithm developed for CRBSI, CLABSI and intensive care unit (ICU) onset BSI detection for patients in the ICU. 1. List of common commensals from the CDC NHSN. 2. Only short term central vascular catheters are considered. 3. Specimens included : respiratory samples, urinary samples, central nervous system samples, abdominal samples, bone and joints samples. 4. This rule applies only to true pathogens and not to common commensal (even if classified as true pathogen on step 3). ICU: intensive care unit; BSI: bloodstream infection; CVC: central vascular catheter; CLABSI: central line associated Bloodstream Infection; CRBSI: Catheter related bloodstream infection; CC: common commensals
The primary outcome identified by the algorithm was CRBSI, as described above. CRBSI has been identified as the gold-standard patient-oriented endpoint, as it has the best construct validity to establish causality between a BSI and the catheter and because it is significantly associated with increased mortality [18]. The two secondary outcomes identified by the algorithm were CLABSI and ICU-onset BSI.
Validation and statistical methodsIncidence was calculated using catheter-days as a denominator for CRBSI and CLABSI and patient-days for ICU-BSI. For CRBSI, we calculated estimates of sensitivity, specificity, negative and positive predictive values of the automated algorithm detection compared to the reference standard (manual surveillance using ECDC definitions), from 1 January 2016 to 31 December 2021. Root cause analysis was performed for all discrepancies between the manual and automated monitoring results.
For validation of the secondary outcome (i.e., CLABSI), each episode identified by the algorithm from 1 January 2020 to 31 December 2021 was manually reviewed by an IPC pharmacist (MGH) and/or an ID specialist (GC). Each episode was classified as true positive or false positive, according to the aforementioned definitions. For validation of the ICU-BSI, a random sample of the episodes (10% of the episodes) identified by the algorithm from 1 January 2019 to 31 December 2021 was manually reviewed following the same method.
The calculation of sensitivity, specificity, negative and positive predictive values of the fully automated surveillance system was performed according to standard epidemiological methods [19]. Confidence intervals for the specificity, sensitivity, positive and negative predictive values were performed using the Wilson score interval method. All calculations were performed with R (R foundation, version 4.1.3).
EthicsThis surveillance was conducted as part of the routine quality improvement activities of our infection control program. Thus, institutional review board approval from the Commission Cantonale d’Éthique de la Rercherche de Genève, as well as individual consent, was not required, according to the definition of research in the Swiss Human Research Act. All data were anonymized.
留言 (0)