
記住我
Between April 2019 and December 2022, a total of 252 patients were included at 15 sites in the Netherlands, Belgium, Canada, and the UK. Baseline patient demographics are reported in Table 1. The median age was 82 [25th–75th percentile, 78–85] years, 53% were female, and the median Society of Thoracic Surgeons Predicted Risk of Mortality (STS-PROM) score was 2.2% [25th–75th percentile, 1.6–3.3]. Overall, 3936 transfemoral TAVI procedures were performed at the 15 participating sites during the study period.
Table 1 Baseline characteristicsProcedural data are summarized in Table 2. An ACURATE Neo or Neo 2 was implanted in 98% of patients. Reasons for a different transcatheter platform than ACURATE were as follows: anatomical mismatch (n = 2), emergency surgery (n = 1), and no on-site availability of the proper ACURATE valve size (n = 1). In two patients, no clear reason was provided. Overall, two patients required conversion to surgery and three patients needed more than one transcatheter heart valve (due to two valve migrations, one severe aortic regurgitation [AR] due to high implant).
Table 2 Procedural characteristicsLocal anesthesia or conscious sedation was used in 153 (61%) and 97 (38%) patients respectively. Escalation to general anesthesia was required in the 2 patients (1%) because of conversion to surgery. A filter-based cerebral embolic protection device was used in 99 (39%) patients. Routine post arteriotomy closure angiography was performed in 9/15 sites. The other 6 sites made femoral angiography when clinically indicated.
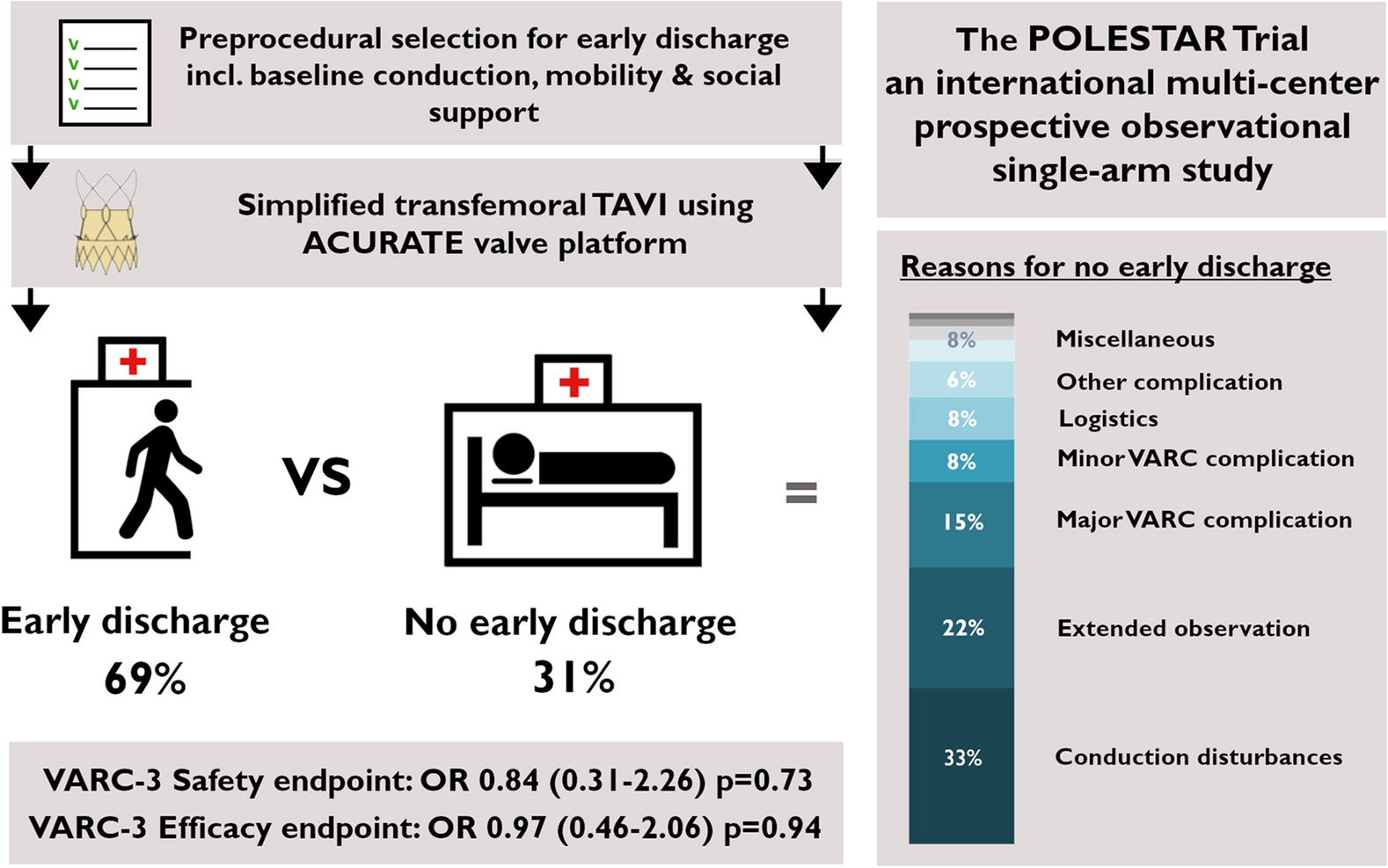
Early discharge was achieved in 173 patients (69%), and in 79 patients (31%), discharge was delayed. Reasons for ED failure are tabulated in Fig. 1. Conduction disturbances with prolonged rhythm monitoring were needed in 33%, and extended (clinical) observation for the likes of fever and/or elevated CRP levels was reported in 22% and (major) VARC-defined complications in 15%. In the overall population, the median length of hospital stay was 2 [25th–75th percentile, 1–3] days. ED was more common in the 2nd half of the enrollment period (79/126 vs. 94/126, p = 0.04).
Fig. 1
Reasons for no early discharge. Left histogram shows the total population. Right histogram shows the no early discharge subgroup. Complications are defined according to the Valve Academic Research Consortium (VARC)-3
Compared to the ED group, patients with no ED had lower BMI and more often a history of previous stroke (Table 1). Regional differences were observed, with the highest ED rate in the UK and lowest in the Netherlands (Supplementary Table 2). After discharge, one patient withdrew from study participation.
Overall, all-cause mortality was 1% at 30 days with a stroke rate of 2%. Major vascular complications occurred in 4% of patients. A total of 34 (14%) patients reached a safety endpoint at 30 days. In the landmark analysis after 2 days, 7% and 9% of patients with ED and non-ED reached the safety endpoint respectively (OR 0.84 [25th–75th percentile, 0.31–2.26], p = 0.73) (Table 3). Clinical event rates decreased per year (OR 0.64 [25th–75th percentile, 0.41–0.99], p = 0.04). A total of 39 (16%) patients reached the efficacy endpoint at 30 days. The 2-day landmark analysis showed that 15% of patients with ED and non-ED reached the efficacy endpoint between 2 and 30 days (OR 0.97 [25th–75th percentile, 0.46–2.06], p = 0.94). Procedure year did not affect the efficacy endpoint (OR 0.86 [25th–75th percentile, 0.62–1.20], p = 0.38). No other covariates were included due to low number of events.
Table 3 Primary outcomes at 30 daysSecondary outcomes at 30 days are reported in Table 4 and Supplementary Table 3. Overall, 9 patients (4%) received new permanent pacemaker implantation (PPI). Reasons for PPI were total atrioventricular block (n = 7) or new left bundle branch block with increasing PR interval (n = 2). Of these patients, 6 required new PPI during the index hospitalization, all of which were discharged > 48 h after TAVI. Three (2%) patients in the ED group required PPI, which all occurred after discharge, and thus required rehospitalization. Of the 26 patients who had extensive telemetry monitoring beyond 48 h, 6 (23%) received PPI before discharge. Notably, there was no difference in permanent pacemaker, left bundle branch block, or atrial fibrillation between discharge groups at baseline.
Table 4 Secondary outcomes at 30 daysAt 30 days, 18 (7%) patients were readmitted with 10/18 (56%) patients hospitalized for procedure- or valve-related reasons. No significant differences were observed between ED and non-ED groups in terms of all-cause rehospitalization and rehospitalization for procedure- or valve-related causes. (6% vs. 9%, p = 0.48 and 3% vs. 6%, p = 0.29, respectively).
Echocardiography-derived hemodynamic valve performance at 30 days showed a mean AVA of 2.0 ± 0.6 cm and residual mean gradient of 8 mmHg (6–12 mmHg). More than mild AR was present in 3% of patients (Supplementary Table 4). No difference was observed in > mild AR between ACURATE Neo and Neo 2 (3/114 vs. 4/115, p = 0.99).
The median EQ-5D-5L index score improved from 0.83 [0.72–0.91] at baseline to 0.88 [0.80–1.00] (p < 0.01) at 30 days. The KCCQ Overall Summary Score increased from 66 [50–85] to 87 [71–95] (p < 0.01) at 30 days (Supplementary Table 5). KCCQ improved similarly in patients with ED and no ED. EQ-5D-5L VAS improved more in the ED cohort (Supplementary Table 6). Data for TAVI with ACURATE Neo and Neo 2 are reported in Supplementary Table 7.
留言 (0)