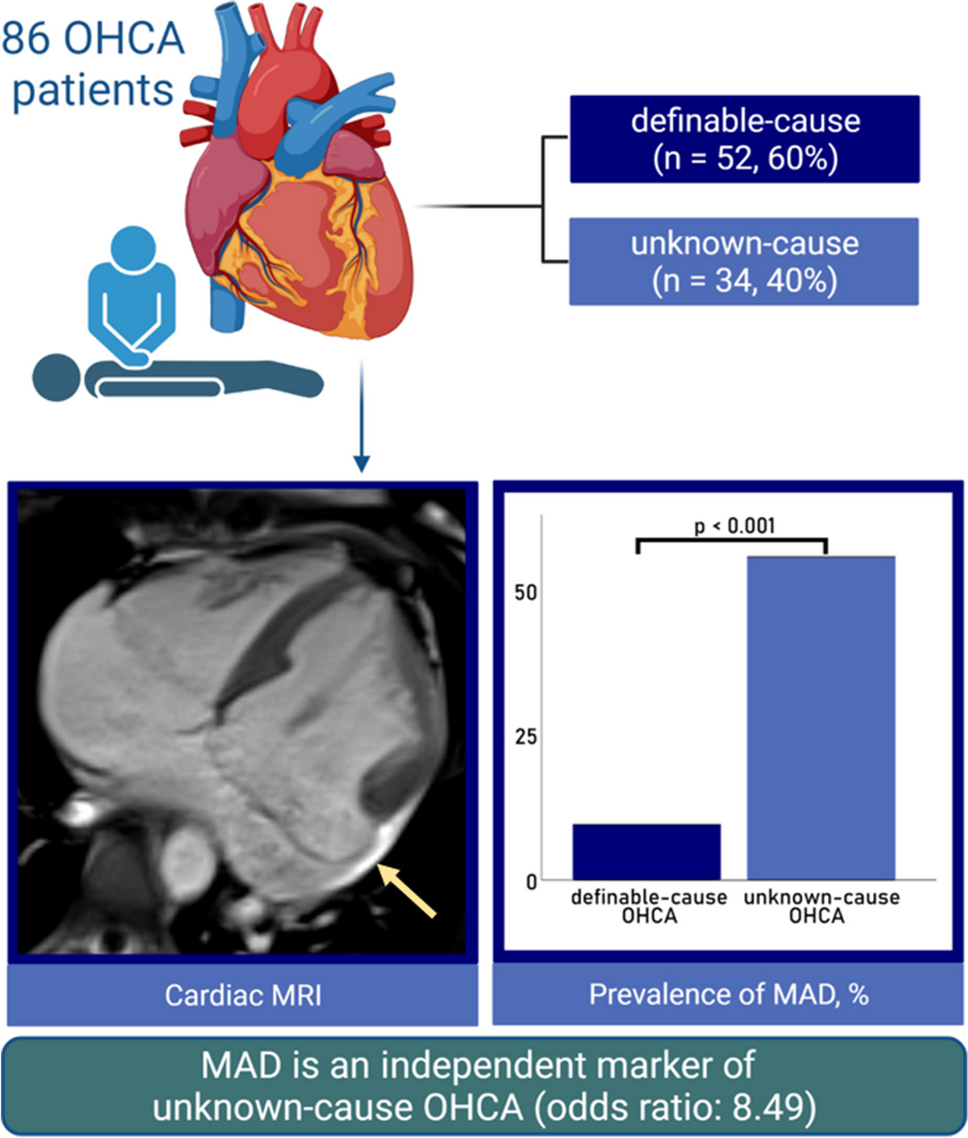
This study is the first to investigate the role of MAD particularly in OHCA patients undergoing CMR imaging. Our results are as follows: when screened and diagnosed via CMR, (a) MAD is common in patients with unknown-cause OHCA, whilst (b) it is far less common in patients with a definable cause of OHCA; (c) MAD patients in our CMR study showed generally less comorbidities for cardiovascular events; however, (d) MAD was revealed to be an independent marker for unknown-cause OHCA after adjustment for age, hypertension, and hypercholesterolemia.
Prevalence of unknown-cause OHCA
In the present analysis, no definite cause for CA could have been found in 40% of OHCA patients despite profound diagnostics. This number exceeds the observations of a German register study investigating 33,772 OHCA patients between 2007 and 2017. In that study, the proportion of unknown-cause OHCA was 17% [16]. A possible explanation for this discrepancy is the fact that in most cases of definable-cause OHCA (e.g. myocardial infarction), there is no general recommendation for further investigation via CMR [17]. Furthermore, due to its limited availability, CMR is usually only performed when the most common reasons for CA can be excluded beforehand. This additionally increases the percentage of unknown-cause OHCA in our study, in which, however, performance of CMR is a central inclusion criterion.
MAD in unknown-cause OHCA
In this study, MAD was defined as end-systolic disjunction extent of at least 1 mm, referring to an important forerunner study by Dejgaard et al. [3]. This approach can currently be regarded as quite strict definition of MAD, as many other studies tended to define MAD as disjunction of any extent [7, 11, 18]. However, in some rare studies, also larger cut-offs can be found, such as 2 mm [19] and 5 mm [20]. As the minimum MAD in this present study was 2.8 mm, shifting the threshold to 2 mm would have had no effect on the outcome; however, a threshold of 5 mm would have decreased the MAD prevalence to 17% (n = 15, 12 with unknown-cause OHCA, 35% vs. 3 with definable-cause OHCA, 6%, p < 0.001). Moreover, a MAD cut-off of 8.5 mm (which was shown to predispose for the development of non-sustained ventricular tachycardia [21]) still yielded a significant result (MAD < 8.5 mm, n = 7: 86% unknown-cause vs. > 8.5 mm, n = 79: 34% unknown-cause, p = 0.009).
One main finding of our study was that MAD was diagnosed significantly more often in unknown-cause OHCA patients, while these patients generally showed distinctly less comorbidities, especially in terms of age, BMI, blood pressure, hypercholesterolemia, and CAD prevalence. According to a cohort study by Essayagh et al. in 595 MVP patients, the presence of disjunction was an independent risk factor for the occurrence of arrhythmic events in the long-course [22]. This finding is in line with a study by Dejgaard et al., which found severe arrhythmic events in 12% of MAD patients and postulated MAD to be an arrhythmogenic risk factor itself, independent of concomitant prolapse [3]. What is more, a large CMR-register study by Zugwitz et al. in 2022 numbered a mean MAD-extent of 3.4 mm in healthy subjects with MAD [23], which is clearly lower than in our cohort (7.1 ± 3.6 mm), indicating that there might be an association between extent and clinical relevance. Accordingly, multivariate logistic regression analysis in the present study revealed MAD to be an independent marker of OHCA of unknown cause after adjustment for age, hypertension, and hypercholesterolemia. The latter three all represent classical risk factors of ischemic heart disease, which mirrors the high prevalence of myocardial infarction in the definable group. There are hardly any other data available about the role of MAD in OHCA. However, a study by Lee et al. investigating the association of MVP and severe arrhythmias indicated that systolic curling motion in MAD was a strong and independent predictor of these events [15]. In the present study, systolic curling motion was more common in unknown-cause OHCA patients; however, this difference was not significant, which is probably due to the small number of MAD in definable-cause OHCA patients.
Features of unknown-cause OHCA
Besides MAD, female sex has proven to be a strong prognostic marker for unknown-cause OHCA (and besides the only other significant marker for unknown-cause OHCA in the univariate analyses), with 74% of these patients being female. Referring to the above-mentioned register study, almost 65% of all OHCA patients were male, which is in line with our study (58%). However, the percentage of women with unknown-cause OHCA in that register study was 40%. This is most likely due to the high rate of cardiac events in the definable-cause group (83%), which is accordingly more common in men [16]. Then, although patients in the unknown-cause group in general had structurally normal hearts, some of them still showed an EF below 40%. A sensible explanation for this phenomenon can be found in a study by Gonzalez et al., describing a marked decrease of LV-EF up to 25% due to CA, hinting that perhaps these patients with lower EF at CMR had a normal ventricular function pre-CPR [24]. Additionally, it can be assumed that the partly quite short interval between CPR and CMR also plays a non-neglectable role here, as the LV function underlies a high variability during the first few days after cardiac recovery, which was shown by Kalra et al. in OHCA patients via echocardiography [25]. Another finding, which is probably a result of the high frequency of cardiac triggers for CA in the present study, is that LGE was significantly less common in unknown-cause OHCA and in MAD patients. LGE was found to be a strong predictor for definable-cause OHCA. The percentage of patients with LGE in the definable-cause group (72%) is in line with a study by Neilan et al., detecting LGE in 71% of a patient cohort of 137 CA survivors [26]. Contrary, the proportion of patients showing LGE in the unknown-cause group was less than a tenth. This could be due to the young age of patients in this group as well as the low risk profile.
Epidemiologic features of MAD
In the present study, MAD was evident in 28% of patients in at least one segment of the posterior mitral leaflet. This is approximately in line with three studies reporting the prevalence of MAD via transthoracic echocardiography in MVP patients (MAD in 22%) [27], via 3D-TEE in a mixed-patients cohort (27%) [15] and via CMR in myxomatous mitral valve disease (35%) [7]. However, according to a recently published study by Toh et al., investigating the prevalence of MAD in a population of 98 patients without structural heart disease via CT, the true prevalence of MAD could be up to 96% [6]. This marked difference to our present study could be at least partly due to the underlying examination method, as CT shows a higher spatial resolution than CMR, which also manifests itself in a larger median MAD-extent in our study (5.7 mm vs. 3.0 mm in Toh et al.).
The ratio of 75% women in MAD patients is in line with a study by Perazzolo Marra et al., describing MAD as a constant feature of arrhythmogenic MVP [4]. According to a large investigation of MVP prevalence in the course of the Framingham Study, MVP in general was shown to be a feature mainly affecting young women [28]. As MAD is very often still accompanied by MVP, this would be in agreement with our data. However, data about sex distribution in MAD are currently rather inconsistent [2] and studies still lacking. Another common feature of MVP is thickening of the mitral leaflets [4], which was shown to be best described via CT or echocardiography [29]; in our cohort, mitral leaflet thickening ≥ 5 mm (i.e. suggesting Barlow’s disease [30]) was not detected (long-axis cine images, end-diastole), with a median thickness of 1 mm and a maximum of 3 mm.
MAD and arrhythmias
Interestingly, the difference in initial ECG findings at CPR between patients with and without MAD was of borderline significance, with all 24 MAD patients showing VF at first medical contact. Overall, 84% of patients in the present study initially presented with a shockable rhythm, which is in line with a study by Majewski et al. investigating 871 OHCA patients that survived the first 30 days after CPR [31]. In the first post-CPR-ECG, the main difference between definable-cause and unknown-cause lies in the presence of repolarization disorders, being primarily due to the high ratio of myocardial infarctions showing ST elevation in the first group, with the remaining entities being rather unspecific repolarization abnormalities. There are no data available about arrhythmias requiring CPR in MAD; however, as this study’s MAD patients were distinctly younger than patients without MAD and showed less risk factors (i.e. diabetes, hypertension, hypercholesterolemia, CAD), these findings hint that the disjunction itself bears arrhythmogenic potential, especially in favour of ventricular arrhythmias [3]. Further, although being more and more regarded as arrhythmogenic entity itself, it is not yet clear why the presence of MAD seemingly predisposes for the development of severe arrhythmic events. Some studies postulate fibrosis of the myocardial wall or the papillary muscles as a reaction to myocardial stretch generated by a hypermobile mitral valve apparatus and a contingently prolapsing leaflet as the primary pathophysiology of MAD arrhythmic syndrome [32, 33], which can pithily be summarized as ‘hypermobility-stretch-fibrosis-sequence’. Another hypothesis involving damage or tissue change of the cardiac conduction system has not yet been sufficiently investigated [3, 34], but would explain the increased risk of arrhythmic events in MAD patients even without the presence of MVP [3] or, as shown in our study, LGE. The fact that only 9% of unknown-cause patients in our study showed replacement fibrosis is probably due to a compound of these and maybe still unknown pathophysiological mechanisms that result in arrhythmias even before being measurable. Then, if the currently more prevalent idea of a sequence consisting of a hypermobile mitral valve apparatus causing persistent myocardial stretch, which itself leads to myocardial fibrosis, proves right or at least partially truthful, future considerations regarding treatment could involve interventional or surgical remedying of the primarily underlying hypermobility before the development of clinically relevant fibrosis [35].
Study limitations
We acknowledge that this study bears some limitations, with the most important being its retrospective nature, which results in partly incomplete patient history records and further course after discharge. For example, genetic testing or endomyocardial biopsy was only performed in eight of the unknown-cause OHCA patients, as in clinical routine most genetic/congenital causes for CA can often be excluded either via ECG (long/short QT syndrome, Brugada syndrome, early repolarization syndrome) or via CMR (primarily arrhythmogenic right ventricular cardiomyopathy) [36]; nevertheless, a wider use of genetic testing would have raised the validity of our study. Furthermore, the selected patient population is subject to a certain selection bias, as the percentage of patients with unknown-cause OHCA was overproportionally high, due to the availability of CMR imaging being a central inclusion criterion and the less common referral to CMR in definite-cause OHCA. Another issue associated with our retrospective approach was that not all patients had CMR after OHCA—however, when excluding those with CMR prior to CA, MAD would still be more common in unknown-cause OHCA (57% vs. 15%, p < 0.001). Then, a probably very helpful tool and valuable addition to our analysis concerning tissue characterization in MAD could be parametric myocardial mapping. However, these sequences were not obtained in many patients due to these patients having been scanned before mapping sequences were commercially available. Lastly, CMR protocols were not entirely uniform due to the fact that CMR was primarily performed as a part of clinical routine rather than a scientific study; however, all patients were adequately evaluable in terms of MAD and cardiac function.

留言 (0)