In this multicentric cohort followed at tertiary centers in Italy and UK for the last 20 years, 1 in 5 patients with PAH had features suggestive of concealed LHD. Although most often treated with single therapy, they had a survival similar to those without features of LHD. In these subjects, both the COMPERA and COMPERA 2.0 tools performed better in predicting prognosis at follow-up than at baseline. However, only COMPERA 2.0 reflected the effect of therapy by reclassifying a significant proportion of patients into the low and intermediate-low risk strata.
The age of the PAH population has progressively increased worldwide. Mean age of PAH patients in the Swiss PH registry rose from 53 ± 16 years between 2000 and 2004 to 60 ± 15 years between 2009 and 2012 [20]. Both the COMPERA registry and the Registry to Evaluate Early and Long-term PAH Disease Management (REVEAL), 2 large-scale ongoing observational studies in Europe and USA, now include sizable numbers of old individuals with PAH [21, 22].
This demographic shift explains why risk factors for LHD have become common among PAH patients. By convention, LHD is considered likely when at least 3 diseases are present among the following: arterial hypertension, DM, obesity, and CAD. AF is also often taken into account, as it is mostly associated with LHD. The frequency of patients with such a clinical profile has been shown to range from approximately 16% to 25% [6, 9, 23].
It should be highlighted that having conditions that predispose to LV diastolic dysfunction does not necessarily implicate elevated left heart filling pressures at rest. Pulmonary hemodynamics may be indicative of combined post- and pre-capillary PH, rather than of pre-capillary PH, even if the aforementioned risk factors for LHD do not cluster in one patient. Likewise, a classical PAH hemodynamic profile, with high PVR and low PAWP, may be observed in spite of concomitant comorbidities heralding LHD. This consideration is buttressed by the observation that a minority of the patients in our registry had coexistence of clinical and hemodynamic criteria for occult LHD (7 out of 57, 12.3% in the main analysis; and 12 out of 80, 15% in the secondary analysis). A similar finding was made in the post-hoc analysis of the GRIPHON trial, in which 55.6% met the clinical definition of PAH-LHD, 39.4% the hemodynamic one, and just 5% both [8]. In an Italian study of elderly PAH patients, there was even no overlap between clinical or hemodynamic criteria for PAH-LHD [9].
Being the classification of PAH-LHD quite discordant by means of clinical or hemodynamic parameters, the combination of either type of information, as adopted by the AMBITION steering committee, appears to be the most effective way not to miss subjects with PAH-LHD. To the best of our knowledge, this is the first report of the real-life frequency of PAH-LHD as per AMBITION criteria. The prevalence we found (20%) is higher than the one described in the GRIPHON trial (13%); however, enrollment in the latter was not allowed if PVR was < 5 WU or age was > 75 years, thus favoring the selection of individuals without PAH-LHD.
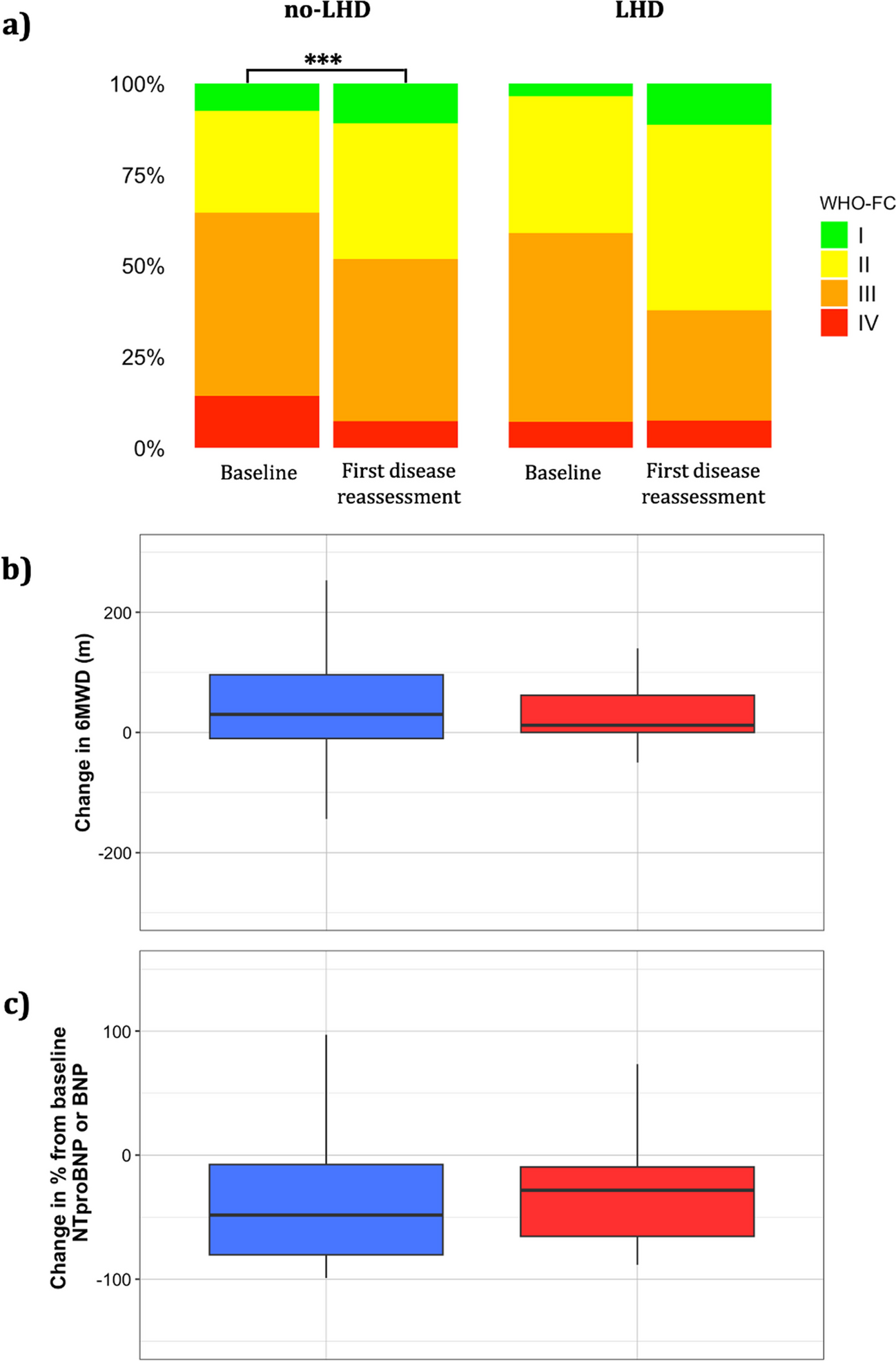
Compared with those without LHD, the patients with PAH-LHD in this study had signs of LV diastolic dysfunction, indicating that adopted definition reliably identifies PAH-LHD. They also had milder PH and RV impairment with lower concentrations of BNP and, although not to a significant extent, NT-proBNP. Nonetheless, functional status, as determined by WHO-FC class and 6MWD, was alike in the no-LHD and PAH-LHD groups. This finding is in contrast with previous investigations, which related higher symptom burden and worse functional capacity to CV comorbidities [22,23,24,25,26], possibly because the patients without a LHD phenotype in our cohort had more advanced PAH. Modulation of natriuretic peptide levels by neurohormonal inhibitors in subjects with PAH-LHD is also possible and may have influenced the differences as compared with those without a LHD phenotype.
The principles of PAH treatment have evolved in the long time period covered by this analysis, justifying the relatively low use of 2 oral drugs we found at both diagnosis and follow-up. With this shortcoming acknowledged, it is notable that dual therapy in patients with PAH-LHD was almost half as frequent as in patients without a LHD phenotype. This prescription pattern has already been noted by other authors and is supported by current guidelines, which recommend that treatment of PAH with comorbidities should be cautious and start with 1 drug [10, 24,25,26,27].
However, there may be patients with PAH-LHD who benefit from combination therapy. In the GRIPHON trial, the reduction in the risk of a morbidity/mortality event attained with selexipag was consistent in participants fulfilling or not the AMBITION definition of PAH-LHD, and 80% were already on an endothelin receptor antagonist and/or a phosphodiesterase type 5 inhibitor at the time of randomization, with 30% on dual treatment [8]. In a recent, single-center study from the Netherlands, the rate of dual therapy and the subsequent hemodynamic and functional response were not different between PAH patients with vs without a high probability of heart failure with preserved ejection fraction according to the H2FPEF score [28].
In our cohort, the improvement in WHO-FC, 6MWD, and NT-proBNP/BNP levels was somehow smaller in patients with than without a LHD phenotype, but survival was comparable, suggesting that a less aggressive therapy in PAH-LHD might be appropriate.
Stratification of the risk of 1-year mortality is now mandatory in PAH management, since treatment intensity and subsequent escalation are based on predicted survival in the current therapeutic algorithm [10, 29]. While a comprehensive assessment incorporating clinical, functional, imaging, and hemodynamic variables is preferred at baseline, a simplified approach including a limited number of measurements is accepted for long-term follow-up [10, 30,31,32]. Most proposed tools for streamlined evaluation of risk in PAH distinguish 3 profiles with increasingly worse prognosis: low, intermediate, and high [11, 14, 33]. The majority of patients are classified at intermediate risk despite having various severity of disease; thereby, the treatment generically advised for the broad intermediate-risk category may not always be suitable. This flaw is overcome by the COMPERA 2.0 model, which further divides the intermediate-risk class in intermediate-low and intermediate-high. Furthermore, the COMPERA 2.0 4-strata model is more sensitive to modifications of risk from baseline to follow-up than other models [12].
CV comorbidities have already been shown to negatively influence the performance of PAH risk scores at baseline [24, 25, 27]. In our study COMPERA and COMPERA 2.0 failed to stratify the risk of all-cause mortality in patients with PAH-LHD at baseline, but showed good discrimination capacity at follow-up. Importantly, treatment of PAH-LHD resulted in a significantly greater proportion of subjects with intermediate-low or low risk at first disease reassessment. This is clinically meaningful, since the intermediate-low and low risk classes were associated with better survival in multivariable analysis. It is also noteworthy that a LHD phenotype did not portend an increased risk of death after multiple adjustment.
Overall, these data validate the use of COMPERA 2.0 for follow-up risk re-estimation in the difficult setting of PAH-LHD. Interestingly, in the aforementioned Dutch investigation, the percentage of PAH patients in the COMPERA 2.0 intermediate-low and low risk categories increased from baseline to follow-up regardless of the H2FPEF score [28].
The present work has limitations. Risk stratification in PAH was implemented in the last years of the study period, as were some medications. Nonetheless, risk assessment at follow-up by COMPERA 2.0 was effective, confirming the usability of this tool even in patients not managed according to the standards of care for PAH. Furthermore, the results of a sensitivity analysis focusing on patients enrolled from 2013 onwards were in the same direction as those of the main analysis. Second, our cohort was selected based on the previous hemodynamic definition of PAH, instead of that given by the most recent guidelines. We decided to do so to facilitate the interpretation of the results of this analysis in the light of other ones, as the cut-offs of mPAP ≥ 25 mmHg, PAWP ≤ 15 mmHg, and PVR > 3 WU have been used in all other studies conducted so far to validate risk scores in PAH. Third, an exaggerated response to rapid infusion of saline may be another tool to unmask LHD in patients with PAWP ≤ 15 mmHg, but it was not evaluated in the patient sample we analysed. Fourth, the inclusion of patients with RHC at follow-up may have led to an underestimation of the frequency of PAH-LHD.

留言 (0)