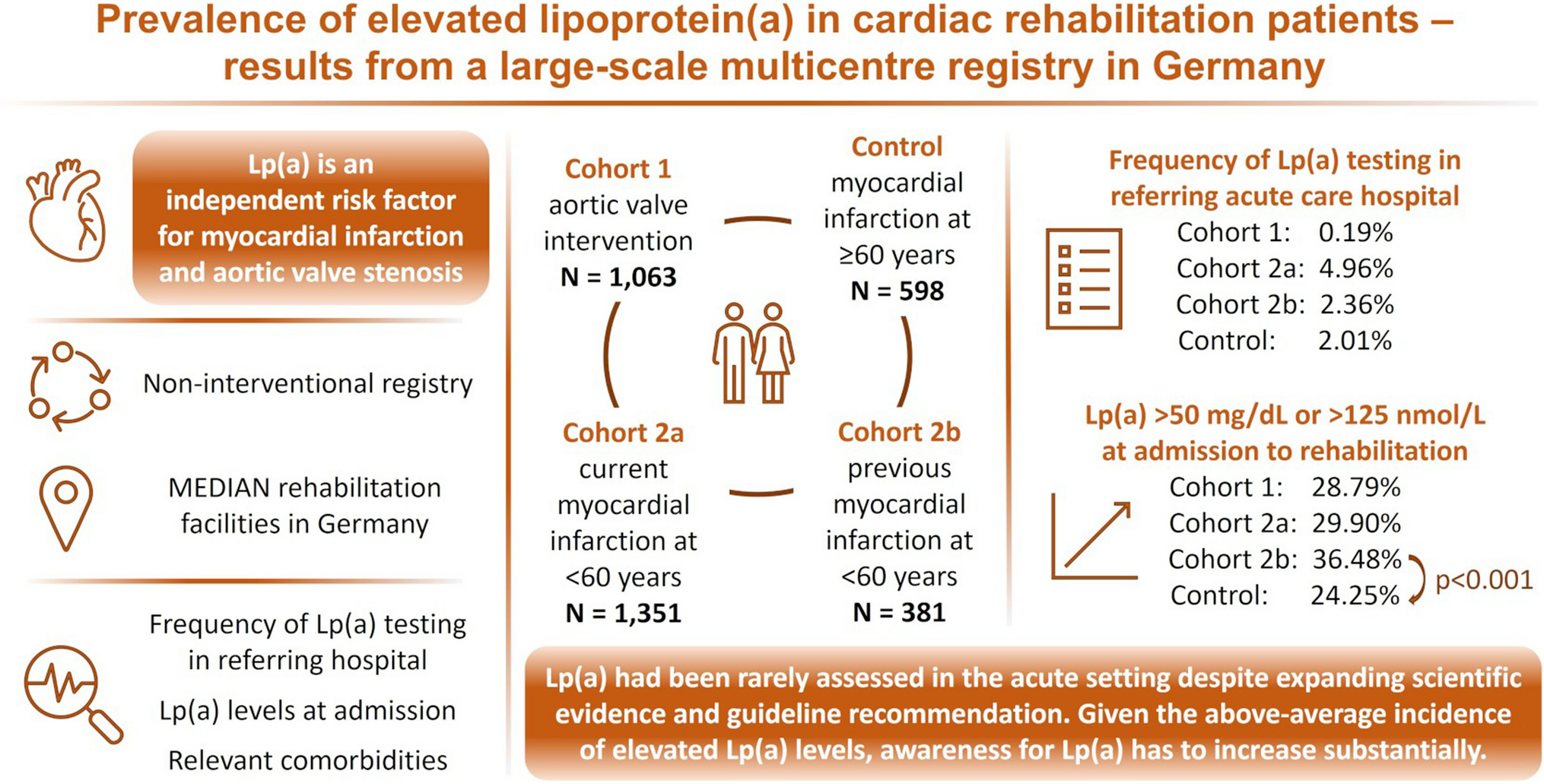
Data from the MEDIAN Lp(a) registry show pathologically elevated Lp(a) levels in one quarter to one third of patients with aortic valve intervention or myocardial infarction. Upon admission to rehabilitation, elevated levels of Lp(a) above 50 mg/dL or 125 nmol/L were detected in 28.79% of aortic valve intervention patients. In patients with premature myocardial infarction, 29.90 to 36.48% of patients had elevated Lp(a) levels, and in the control group of patients with myocardial infarction at a later age, the proportion was 24.25%.
According to the Copenhagen Heart Study, 20% of the general European population have Lp(a) levels above 50 mg/dL [10]. Also, in a cohort of 52,898 patients admitted to a clinic for cardiology in Germany, only 18.4% were reported to have Lp(a) levels above 50 mg/dL. This cardiologic cohort study was not limited to patients with major cardiac events [11].The prevalence of pathologically elevated Lp(a) observed in the MEDIAN registry therefore is higher than in the normal population and even higher than in a general cardiologic cohort. Furthermore, our results indicate that elevated Lp(a) levels are more frequent in aortic valve stenosis and myocardial infarctions, especially in patients with early events. This is consistent with the established risk correlations of Lp(a) elevations [3]. Therefore, more attention should be paid to the assessment of Lp(a) levels.
According to the ESC/EAS recommendations, Lp(a) should be determined at least once in a lifetime [7]. This is especially important as Lp(a) elevation is an independent risk factor, increasing the risk for major cardiovascular disease even in patients with low risk according to current scores, e.g. ESC/EAS SCORE. In the MEDIAN registry cohorts, the median cardiovascular risk scores in patients with aortic valve intervention and current or prior premature myocardial infarction were 4.0, 2.8, and 3.0, respectively. Thus, according to the risk scores, these patients did not have a high cardiovascular risk. The slightly higher cardiovascular risk score in cohort 1 can be solely explained by the higher age of these patients compared to cohorts 2a and 2b. Despite similar mean age in cohort 1 and the control cohort, the risk score in cohort 1 is lower compared to the control cohort, which emphasizes that the current risk scores do not adequately cover the actual cardiovascular risk.
Risk factors as diabetes mellitus and hypertension were less common in patients with premature myocardial infarction. However, with respect to diabetes, this only applies to cohort 2a. In cohort 2b, diabetes was more frequent than in cohort 2a, which may also be related to the higher age of the cohort. Cohort 2b included patients with a history of premature myocardial infarction, however, neither the time since the event had been documented nor the time since diagnosis of comorbidities. Therefore, it remains unclear whether diabetes mellitus was already prevalent at the time of the event in patients of cohort 2b. At the time of admission to the rehabilitation clinic, HbA1c levels were unremarkable on average. It can therefore be assumed that the blood glucose levels were well adjusted in all cohorts. Regarding patients in whom hypertension was documented, the current systolic and diastolic blood pressure on average indicated an adequate therapeutic management.
Dyslipidaemia was less frequent in cohort 1 of patients with aortic valve intervention and presumably plays a smaller role here than in other cohorts. All patients with documented dyslipidaemia received lipid-lowering therapy, but almost exclusively oral medication was mentioned. The LDL-C values measured upon admission to our institutions suggested insufficient LDL-C adjustment. The ESC/EAS-recommended LDL-C target level of 1.4 mmol/L for high-risk cardiac patients is rarely achieved [7]. It has to be pointed out that in our data, it remains unclear how long it has been since a lipid-lowering therapy has been initiated. Nevertheless, at least in the patients with history of myocardial infarction in cohort 2b, it could be assumed that dyslipidaemia had been diagnosed some time ago. If that is the case, lipid-lowering therapy had not been escalated adequately. According to modelling approaches and clinical investigation, available therapeutic options, including injectable escalation therapies, are sufficient to allow target achievement in almost all high-risk patients [12, 13]. Average triglyceride levels were within the normal range in all cohorts.
The ESC/EAS recommendation for a general Lp(a) test is controversial. Parhofer and Laufs argue against an extensive determination of Lp(a) levels as specific drug therapy for lowering Lp(a) is not yet available. However, they point out the importance of cascade screening [14]. Our registry data shows that more than one third of patients with premature myocardial infarction had a relevant family history of premature cardiovascular events compared to only one fifth of patients with aortic valve intervention and in the control cohort. This supports the importance of cascade screening [15]. However, an effective cascade screening would initially require the determination of Lp(a) in the index patients, i.e. those with a current cardiovascular event. The present MEDIAN Lp(a) registry data show that the assessment of Lp(a) is rarely implemented in clinical practice in Germany. Lp(a) had been determined in less than 5% of cases in the setting of acute hospital care, even in patients with premature myocardial infarctions. In patients with aortic valve stenosis, we were able to identify Lp(a) levels determined prior to rehabilitation referral in only 0.19% of cases.
The observed Lp(a) determination rate is insufficient given the relevance of Lp(a) levels especially if other risk factors do not sufficiently explain the occurrence of events. Patients who have experienced a life-threatening event need clarification of the causes with appropriate intervention and counselling on how to prevent future events. Unfortunately, no specific drug therapy is currently available on the market for the reduction of Lp(a) levels, standard drugs for the treatment of dyslipidaemia do not show sufficient effect on Lp(a) levels, and the risk of re-events may not be adequately reduced by LDL-C reduction alone [3]. From the point of view of cardiological rehabilitation, elevated Lp(a) and a cardiovascular risk constellation therefore result in an enormous need for advice for those affected. It is essential for the treating physicians to support their patients through systematic and adequate patient information and training, and to provide them with offers of cascade screening, and participation in scientific studies. Furthermore, participation in specialized self-help groups (e.g. https://lipidhilfe-lpa.de, which was founded in Dresden in 2019) could promote patients understanding of the disease. This may significantly increase motivation for strict normalization of manageable risk factors. Therefore, we advocate a systematic determination of Lp(a) in risk constellations, with the setting of cardiac rehabilitation offering advantages here. The MEDIAN registry data demonstrated the feasibility of Lp(a) assessments in the routine of cardiological rehabilitation.
The current data demonstrate the urgent need to increase awareness for Lp(a) assessments. This could be achieved through inclusion of Lp(a) in the common cardiovascular risk scores. In the EAS Consensus Statement, the working group quantified the increase in risk due to Lp(a) as a function of baseline risk score. A lifetime risk for major cardiovascular events of only 5% based on the current risk scores nearly triples at an Lp(a) of 150 mg/dl to reach 13.6% [3]. Inclusion of Lp(a) values in the risk scores also requires test standardization. A lack of test standardization in the past certainly contributed to the reluctance to assess Lp(a) levels [16]. Today, most commercially available assays are based on the same methodology using nmol/L as standard unit (with conversion to mg/dL, if necessary). The available assays provide comparable clinical utility in terms of cardiovascular risk assessment [17].
The present data of the MEDIAN Lp(a) registry provide valuable and representative insights on the current state of Lp(a) determination in Germany. The registry included a large-scale patient population which is representative for rehabilitation after aortic valve stenosis and premature myocardial infarction. The annual incidence of aortic valve stenosis interventions in Germany was reported to be approximately 30,000 in 2019 [18]. The annual incidence of acute myocardial infarction in patients younger than 60 years of age was reported to be approximately 50,000 in 2009 [19]. Over 1 year, the registry included over 1000 patients after aortic valve stenosis-associated intervention and almost 1500 patients younger than 60 years of age receiving follow-up treatment after acute myocardial infarction. Therefore, the registry covers approximately 3% of annual incident cases with aortic valve stenosis interventions and premature myocardial infarction in Germany. Furthermore, the German healthcare structure is fully reflected in the participating MEDIAN facilities, which means that members from both statutory and private health insurances are referred. Referrers are clinics with different care mandates, i.e. from basic and standard care facilities to major regional and maximum care facilities.
Despite the favourable scale of the registry and the representative structural conditions at the participating sites, the present data bears some limitation. In this context, it is particularly important to mention that LDL-C levels are not known prior to referral for rehabilitation or at the time of the event. Furthermore, it was not known which lipid-lowering therapy the patients were receiving at the time of admission to the rehabilitation facility and how long they had been receiving lipid-lowering therapy. Therefore, the influence of LDL-C as a major risk factor for cardiovascular events cannot be comprehensively assessed in the cohorts. The same applies to further relevant comorbidities as diabetes mellitus or hypertension. Regarding previous Lp(a) assessments, it should be mentioned that apart from Lp(a) levels obtained from referral documents, no information on previous assessments was available and was not actively queried. It is therefore possible that Lp(a) had already been assessed prophylactically in some patients and that a determination in the acute setting may therefore have been obsolete.
Overall, the MEDIAN Lp(a) registry shows that Lp(a) assessment in the context of severe cardiac events is performed infrequently, and at the same time, it demonstrates the above-average incidence of pathological elevation of Lp(a) levels in patients with aortic valve stenosis or premature myocardial infarction. Given the established association of Lp(a) elevation and cardiac risk, significantly more attention needs to be paid to Lp(a) levels to better identify and manage patients at risk. The rehabilitation phase is an appropriate context for this.

留言 (0)