
記住我





The original trial employed a three-group parallel (1:1:1), single-blind randomized clinical trial design to compare CT vs BA vs MM. We elected to not add a fourth arm to the trial comprising of an inert control condition as all three techniques have been examined in prior trials and their efficacy has been established relative to inert controls; thus, it would be unethical to assign participants to an inert control and the associated cost would be unjustifiable. This paper represents the main outcome paper related to establishing effect sizes for treatment outcome changes in the trial; however, the current analyses are considered as secondary analyses, given that the primary funded objective of the trial was to elucidate the micro- and macro-level mechanisms of action for the three treatments using ecological momentary assessment (see published protocol) [22]. All study variables were assessed remotely, and treatment was delivered in a group format via videoconferencing technology using the Zoom (https://zoom.us) platform. Study procedures were approved by the University of Washington (UW) Human Subjects Division (Identifier: STUDY00003841), and the study was pre-registered on clinicaltrials.gov (Identifier: NCT03687762) prior to commencing participant enrolment. Data collection took place between October 2018 and March 2022.
Sample recruitment and eligibility criteriaPotential participants were identified primarily via coding lists (i.e., sections of medical charts that identify medical conditions) of UW Medicine patients who had a low back pain diagnosis in their electronic medical record. The UW Medicine setting provides a large variety of services, ranging from primary and preventative care to the most highly specialized medical care for complex conditions. Patients who did not have any clear evidence for having any of the exclusion criteria per their electronic medical record were invited to learn about the study via email and postal mailings; staff also attempted to reach each of these individuals by phone. Other recruitment strategies included the use of the UW Rehabilitation Medicine departmental research participant pool, posted flyers in pain and rehabilitation clinics, clinician referrals, news releases with the UW Newsroom, and a variety of national recruitment strategies, including use of ResearchMatch.org, social media, and posting the study on research and/or pain-related websites. Potential participants were screened for eligibility by research staff over the phone.
Study inclusion criteria were (1) ≥ 18 years of age; (2) low back pain as a primary or secondary pain condition; (3) chronic pain lasting ≥ 3 months, with pain experienced on ≥ 50% of days in the past 6 months; (4) average chronic pain intensity ≥ 3 on an 11-point scale for the past week; (5) chronic pain interference for general activities ≥ 3 on a 11-point scale for the past week; (6) able to read, speak, and understand English to comprehend the worksheets, measures, and interventions implemented; (7) if currently taking analgesic or psychotropic medication, medications must have been stabilized for ≥ 4 weeks prior to this study; (8) availability of a telephone, webcam, and microphone through computer or smartphone; and (9) access to the internet.
Study exclusion criteria were (1) headache as the primary pain condition (because the temporal nature of headache varies widely from that of most other chronic pain conditions, and the outcome measures for headache treatments differ accordingly); (2) severe cognitive impairment defined as ≥ 2 errors on the 6-Item Cognitive Screener [23]; (3) current alcohol or substance dependence [24]; (4) active malignancy (e.g., cancer not in remission), terminal illness, or serious medical condition that may interfere with either study participation or with receiving potential treatment benefits (e.g., severe lupus); (5) inability to walk at least 50 yards, which would limit the ability of participants to benefit from the BA intervention; (6) significant pain from a recent surgery or injury in the past 3 months; (7) pain condition for which surgery has been recommended and is planned; (8) any planned surgery, procedure, or hospitalization that may conflict with or otherwise influence participation in the study; (9) currently or recently receiving other psychosocial treatments for any pain condition, defined as four or more sessions within the past 12 months (as this may influence these treatment results); (10) current or past participation in a research study with treatment components that may overlap those in the current study; (11) current or history of diagnosis of primary psychotic or major thought disorder within the past 5 years; (12) psychiatric hospitalization within the past 6 months; (13) psychiatric or behavioral condition in which symptoms were unstable or severe within the past 6 months; (14) any psychiatric or behavioral issue as noted in the medical record or disclosed/observed during self-report screening that would indicate participant may be inappropriate in a group setting; and (15) a presenting symptom at the time of screening that would interfere with participation, specifically active suicidal or homicidal ideation with intent to harm oneself or others, or active delusional or psychotic thinking.
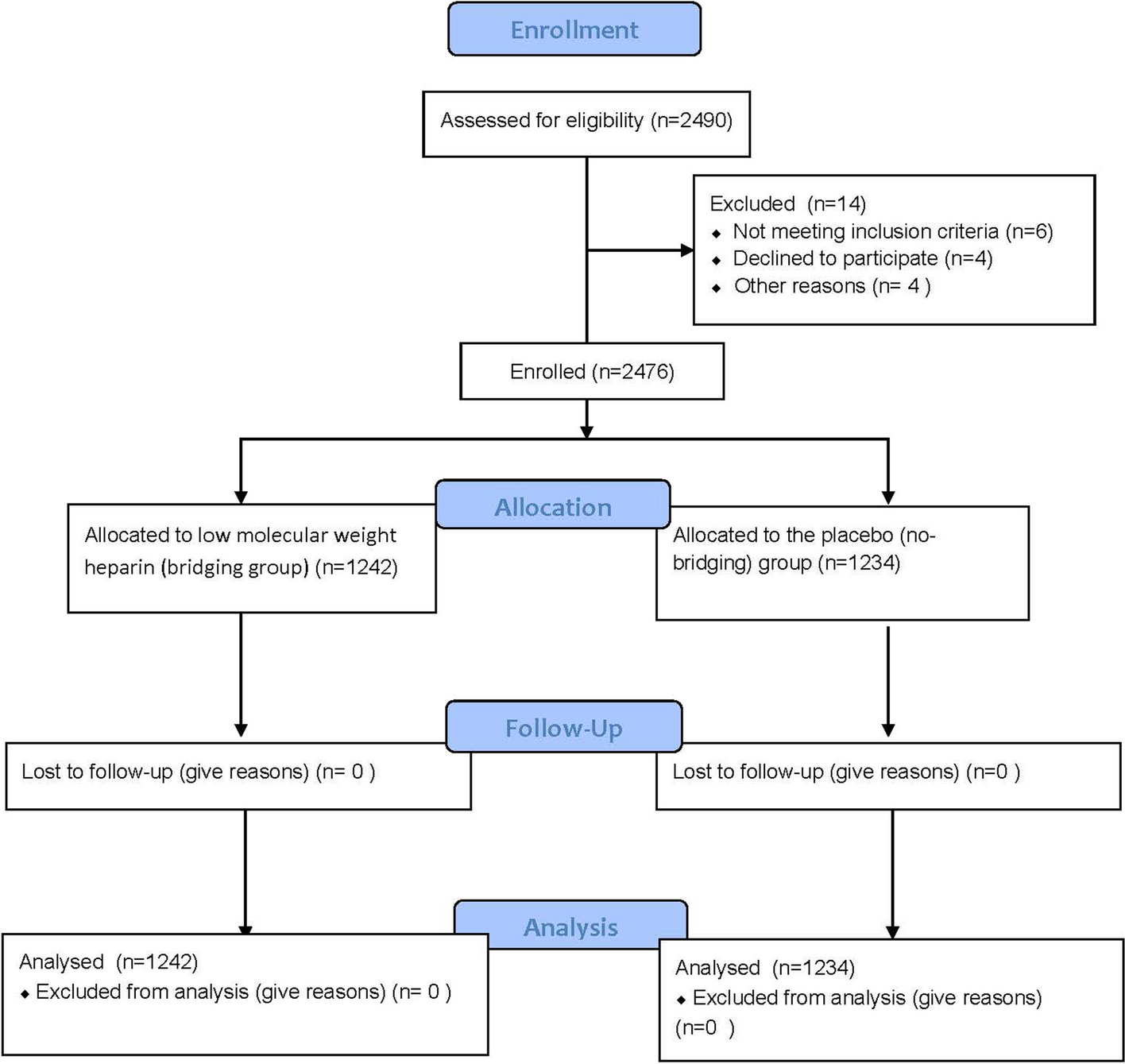
All participants who met eligibility criteria and provided informed consent were asked to complete the pre-treatment assessment, all baseline self-monitoring procedures, and a technology training session on the Health Insurance Portability and Accountability Act (HIPAA)-compliant (i.e., a platform with controlled authorized access and safeguards in place to protect the privacy and confidentiality of participants) Zoom videoconferencing platform used to deliver the treatment sessions (https://zoom.us). Of the 1081 participants screened for eligibility, 100 could not be contacted, 78 declined participation, 494 did not meet screening criteria, and 12 were not recruited as the recruitment period had concluded due to the target sample size having been reached. A total of N = 302 were randomized (n = 101 in BA; n = 99 in CT; n = 102 in MM). See Fig. 1 for a Consolidated Standards of Reporting Trials (CONSORT) flow diagram [25].
Fig. 1
Study design and participant flow—CONSORT diagram
RandomizationAssignment to one of the three groups was accomplished using a covariate-adaptive randomization scheme developed by the study statistician (MAC), based on the procedure described by Pocock and Simon, with the objective of balancing the covariate in the marginal distributions [26]. The covariates were biological sex, baseline pain interference score (mild/moderate or severe, as assessed via the 11-item Roland–Morris Disability Scale [27]) with cutoff for severe being a score of ≥ 7, and whether or not low back pain was the primary or a secondary pain condition.
Concealment of treatment conditionA blinded research staff member (who was unaware of treatment allocation) communicated a numeric randomization code to an unblinded staff member, who conveyed randomization assignment and treatment schedule to participants. Participants were not informed of the study hypotheses, and all outcome assessments and data analyses were conducted by blinded research staff members who were unaware of treatment allocation. No interim data analyses were conducted.
Study interventionsThe interventions were provided simultaneously across thirteen cohorts of participants (i.e., 39 groups in all) via eight, 1.5-h Zoom-delivered group sessions delivered over 4 weeks (i.e., two sessions per week for a total of 12 h of therapy). The Zoom videoconference platform allowed participants to see and hear each other and allowed the therapist to screen-share and display visual information relevant to the respective treatment protocols (e.g., PowerPoint slides) during the sessions. The average number of participants enrolled in each group was 7.7 (standard deviation (SD) = 3.6, range = 2 to 14). The eight-session protocol length was selected as it is consistent with many prior trials and protocols (e.g., typical MBSR protocols are eight sessions long, and cognitive behavioral therapy (CBT) protocols often range from 8 to 12) [7,8,9,10]. Although in prior research, the eight sessions are typically held once per week, we elected to condense this to two sessions per week in this trial as participants were completing twice daily ecological momentary assessments (EMAs), and the participant burden of completing EMAs for 8 weeks during treatment as opposed to 4 weeks during treatment was considered excessive.
The interventions were based on standardized protocols and materials that were developed by the author team, with both the CT and MM manuals used and refined in prior trials [28,29,30]. The therapists were expected to follow the treatment manuals closely to ensure all content was delivered and to ensure the consistency and replicability of treatment (see fidelity monitoring procedures below). Participant workbooks specific to the respective treatment allocation were provided for participants to refer to during the group sessions, as well as additional readings and homework assignments to complete between sessions. Participants assigned to MM also received audio-recorded guided meditations to facilitate home practice.
The five therapists were post-doctoral psychology fellows or licensed psychologists with at least 2 years of clinical experience, including experience providing psychological treatments for chronic pain. They were trained and supervised to deliver all three treatments by study investigators who have considerable experience in the interventions. Therapist training, led by the investigators (MD, DE, and MJ), consisted of assigned readings [31,32,33,34] and a 6-h workshop, for each protocol (i.e., 18 h), as well as a 3-h motivational interviewing (MI) training for enhancing motivation to engage in treatment (i.e., via enhancing reflective listening practices—a MI treatment protocol was not delivered in this trial), and a 3-h training in group leadership techniques and conducting telehealth sessions, including strategies for enhancing group cohesion. Group supervision was provided (by MD, DE, and MJ) weekly during treatment delivery to support fidelity.
Cognitive therapy (CT)Participants assigned to CT were taught cognitive-restructuring techniques, including how to identify automatic thoughts and recognize the connection between thoughts and feelings, behaviors, and pain [31]. Specifically, participants assigned to the CT condition were taught to (1) identify automatic thoughts related to pain, including negative or unrealistic automatic thoughts; (2) evaluate automatic thoughts for accuracy; (3) identify sources and types of distorted/unhelpful thoughts; (4) recognize the connection between automatic thoughts and emotional/physical shifts; (5) challenge negative, distorted automatic thoughts via “weighing the evidence”; (6) develop new realistic alternative cognitive appraisals; and (7) practice applying new appraisals and beliefs.
Behavioral activation (BA)Participants assigned to the BA condition were given information about the negative impacts of inactivity and behavioral avoidance on chronic pain and function [33]. Participants were taught: (1) how to be aware of the activities they avoid because of fear of increasing their pain; (2) how to set effective goals so that, step by step, they can start being more active and resume some activities they enjoyed in the past but are currently avoiding; and (3) behavioral pacing skills, to facilitate an increase in appropriate activity level that is consistent with their goals. They were also encouraged to identify activity goals that were pleasurable and/or meaningful and to develop plans for achieving these activity goals.
Mindfulness meditation (MM)Participants assigned to the MM condition were trained in a combination of Shamatha meditation, which involves training the mind for stability in maintaining focus on a specific object, and Vipassana, an open monitoring practice which involves acknowledging any sensory, emotional, or cognitive event that arises in the mind without evaluation, interpretation, or preference [32]. Participants were taught the following MM practices: (1) 3-min breathing space; (2) body scan meditation; (3) mindfulness of the breath and body practice; (4) mindfulness of the breath, body, sounds, and thoughts; and (5) mindfulness of the breath, body, sounds, and thoughts while also intentionally working with a difficulty through this practice. A guided inquiry of the participant’s experiences followed each in-session exercise and was also implemented in relation to discussing participants’ at-home practice.
Intervention fidelityTherapist adherence to the treatment protocols and quality of treatment delivered were assessed via ratings of a random selection of 25% of session audio recordings (two randomly selected sessions per group). Ratings of both prescribed and proscribed elements were obtained. The therapists were trained by one of the principal investigators (MD) to code the therapy sessions for fidelity ratings; therapists did not rate their own sessions. Therapist adherence to treatment manuals was measured on a 0 (“none, or hardly any adherence”) to 2 (“thorough adherence”) scale, and the average adherence score was 1.98 (SD = 0.07). No prescribed treatment elements were detected in the delivery of any of the conditions. The Therapist Quality Scale, which was developed and validated in this trial, was used to rate therapist quality on a 0 (“poor quality”) to 6 (“excellent quality”) scale [35]. Higher ratings are indicative of greater quality of treatment delivery. The average therapist quality score was 4.34 (SD = 0.55).
MeasuresReaders can refer to the published protocol paper for a full list of all study measures that were administered [22]. Study data were collected and managed using Research Electronic Data Capture (REDCap) tools hosted at the Institute of Translational Health Sciences [36, 37]. The measures that were used to provide data for the analyses presented here are described below.
Sample characteristicsA structured pain interview was used to assess reported pain characteristics [38]. The demographic information obtained included self-reported gender, self-identified race, and self-identified ethnicity, consistent with the U.S. National Institutes of Health inclusion policies. Other participant descriptive variables assessed were years of education, relationship status, employment status, disability seeking status, and income.
Primary outcome: pain interferenceWe selected five pain interference items from the Patient Reported Outcomes Measurement Information System (PROMIS) pain interference item bank to assess pain interference as the pre-specified primary outcome measure [39]. This item bank was developed using item response theory (IRT) which affords researchers the capacity to select those items from the item bank that best suit their needs. The process we used to select the five items to include in this study entailed first evaluating all of the items from the PROMIS pain interference item bank that assessed each of the key domains of pain interference described in the PROMIS interference item bank development article by Amtmann et al. [40], that is, the degree to which pain interferes with an individual’s physical, mental/emotional, and social activities. Then, using data collected in prior studies by our team and data for the original measure development sample [40], we tested three-, four-, and five-item measures with these items in order to identify the items to include, with the selection criteria being to include the fewest number of items needed (i.e., since the items were administered twice daily via EMA, which carries participant burden implications) to achieve an alpha that was > 0.80. Once the alpha for the items reached this cutoff, we stopped testing possible longer forms. Based on this process, the alpha for the five selected pain interference items, which tap a multifaceted assessment of pain interference, was excellent in the general population, 0.95 (N > 800) and good in the pain sample, 0.88 (N = 849). These five selected items ask participants to rate how much pain interferes with: (1) enjoyment of life; (2) ability to participate in leisure activities; (3) day-to-day activities; (4) social activities; and (5) household chores. Respondents rated each item on a 5-point Likert scale ranging from 1 (“Not at all”) to 5 (“Very much”), using a past 7-day recall frame. As is standard practice for PROMIS measures, the responses were computed into T-scores (i.e., mean of 50 and a standard deviation of 10 in the normative sample) [41]. The PROMIS pain interference item pool items were recommended for use by the National Institutes of Health (NIH) task force on research standards for CLBP and have substantial support for their discriminatory and prognostic importance, reliability, and construct validity [40, 42].
Secondary outcomesNine secondary outcomes were assessed. Pain intensity was measured using a single-item, numerical rating scale (NRS) which asked participants to rate their average pain over the past week, on an 11-point scale ranging from 0 (“No pain”) to 10 (“Pain as bad as you can imagine”) [43,44,45]. The NRS has been shown to be a reliable and valid assessment of pain intensity [43,44,45]. To assess physical function, depressive symptoms, anxiety, and sleep disturbance, we used four-item PROMIS scales [39, 42]. As with the PROMIS pain interference items described above, each of the items assessing these domains are rated on 5-point Likert scales, and a T-score can be calculated. The scores reflect the domain as labeled; that is, higher scores represent higher levels of physical function, depression, anxiety, and sleep disturbance, respectively. The PROMIS item banks have demonstrated high reliability and construct validity [39]. The 10-item Positive and Negative Affect Schedule short-form (PANAS-SF) was used to assess general positive and negative affect. Five-items assessed positive affect and five-items assessed negative affect [46], with respondents rating the extent to which they generally feel on a 5-point scale ranging from 1 (“Never”) to 5 (“Always”). For pain medication use, participants self-reported their medication intake in the past 7 days, and the average daily morphine milligram equivalent (MME) was calculated based on published conversion factors [47]. Finally, health care utilization was assessed by asking participants to self-report on the number of visits to a health care professional in the past month.
Adverse eventsAdverse events were self-reported by participants and documented in an electronic regulatory event within REDCap. Individual adverse events were followed until the event resolved or participation in the study ended, whichever occurred first. The majority of adverse events reported by participants were conveyed to researchers without prompt (e.g., disclosed during telephone interviews with staff). Adverse event monitoring formally occurred at the beginning of each treatment session with therapists asking whether anyone had any negative effects that they attributed to the treatment practice or homework; participants with such concerns would discuss the event(s) with their therapists. Any concerns relayed to the therapist that met the definition of an adverse event were documented in REDCap by either the therapist or an unblinded staff member.
Statistical analysesThe power analysis for the trial was based on the sample size needed to test the primary study hypotheses related to the mechanisms of these interventions, which will be reported in a planned future paper on the results of mediation models (see published protocol [22]). For the current analyses, an intention-to-treat approach was used. The primary study end-point was post-treatment (i.e., following the eight-session program, delivered over 4 weeks), and all numeric outcomes were defined as change scores computed from pre- to post-treatment (post-minus pre-treatment). The analyses also include examination of maintenance of effects, with two additional change scores computed from pre-treatment to 3-month and 6-month follow-ups. For each time point, the means of the changes in outcomes were compared among the three groups using an analysis of variance (ANOVA). The sample size varied from analysis to analysis due to missing values, ranging from 234 (at follow-up) to 298 (at the post-treatment primary end-point). The sample size for each outcome at each assessment time point is reported in the supplemental table. For each time point, we also calculated effect sizes (and 95% confidence intervals (CI)) for each intervention and between interventions for the primary outcome of pain interference, as well as for the secondary outcomes (pain intensity, physical function, depressive symptoms, anxiety symptoms, positive and negative affect, sleep disturbance). Pain medication use and pain-related healthcare utilization were categorized for each follow-up time point. Change in morphine milligram equivalent from pre-intervention to follow-up was classified as: “No prescription at pre- and follow-up,” “Increase in dose from pre- to follow-up,” “Decrease in dose from pre- to follow-up,” and “No change in dose from pre- to follow-up.” Medical services utilization was assessed by the number of health care visits in the past month and categorized as: “Decreased number from pre-treatment,” “Same number as pre-treatment,” and “Increased number from pre-treatment.” For each time point, we calculated the proportion in the category of decreased medication or decreased utilization for each intervention and between interventions. Confidence intervals of 95% were also calculated using Jeffrey’s method [48]. A comparison of distribution of the outcomes categories among the three interventions was conducted using the Pearson chi-square for homogeneity. ANOVAs were performed in SPSS v26. Effect sizes and 95% CIs were calculated in RStudio (macro effectsize), and proportions and Jeffrey’s 95% CI were calculated in RStudio (macro binom).
留言 (0)