
記住我



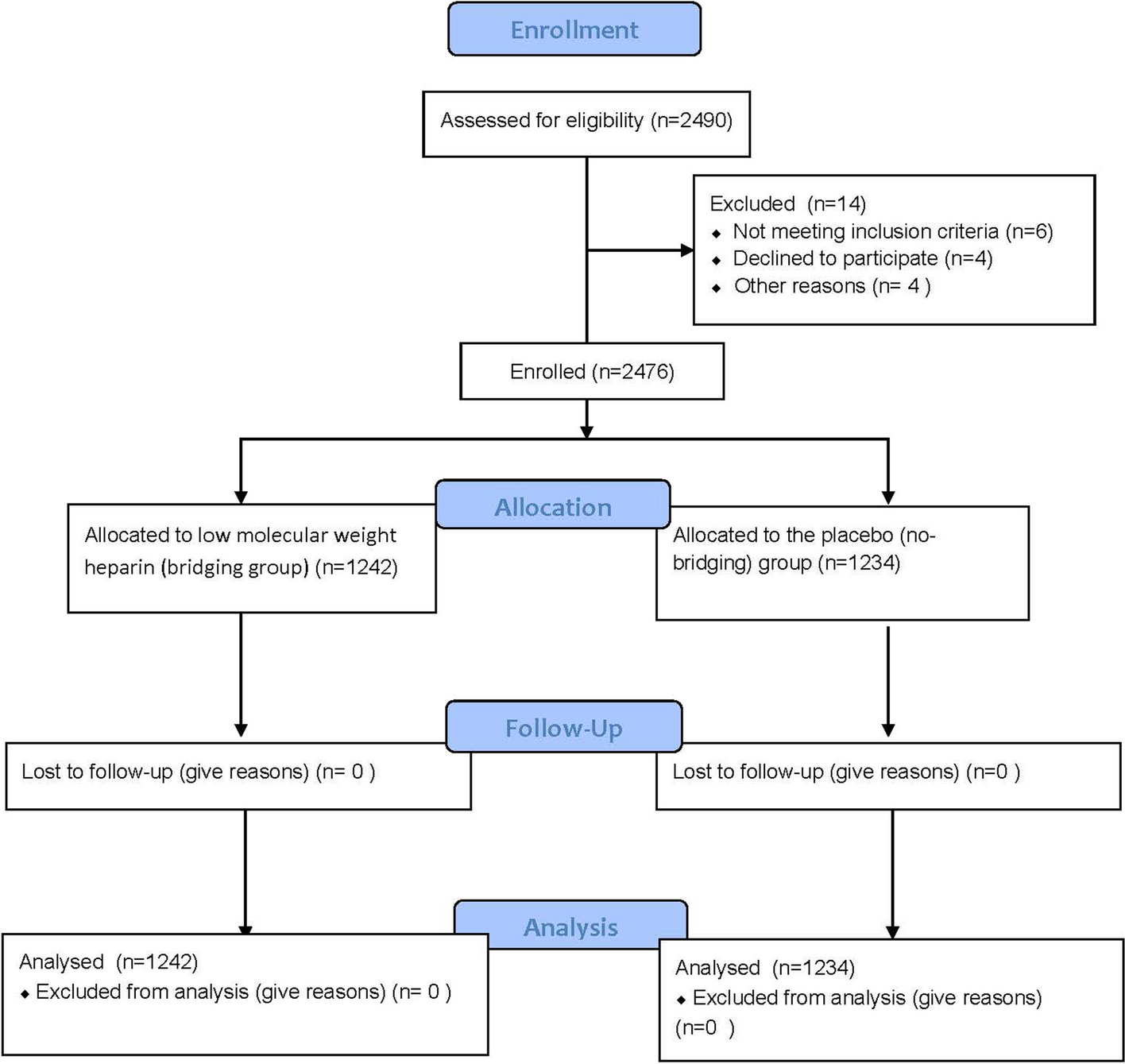

Between September 4, 2020, and January 7, 2022, a total of 64 patients were enrolled (Additional file 1: Fig. S2), and all these patients received study treatment (SAS, including subjects of safety run-in phase, n = 6; and expansion phase, n = 58). The median age of patients was 52.5 years (range, 28.0–70.0), 82.8% were male. At study entry, 17 (26.6%) patients were BCLC stage B and 47 (73.4%) were stage C. Child–Pugh score of 5 and 6 were noted in 58 (90.6%) and 6 (9.4%) patients, respectively. Thirty-seven (57.8%) patients exhibited extrahepatic spread, and 7 (10.9%) had macrovascular invasion. Hepatitis B served as the most common etiology of HCC (58/64, 90.6%). Twenty-six (40.6%) cases had a baseline alpha-fetoprotein level of ≥ 400 ng/mL. Most of the patients (73.4%) had experienced disease progression of previous locoregional therapy (Table 1).
Table 1 Patient demographics and baseline characteristicsAs of December 16, 2022, the median follow-up duration was 15.7 months (range, 0.9–27.4). One patient was still receiving study treatment (last cycle of treatment). The median treatment duration of tislelizumab was 11.0 months (range, 0.7–11.9). The median treatment duration of lenvatinib was 11.1 months (range, 0.3–12.1). Overall, 63 (98.4%) patients discontinued study treatment. The primary reason for treatment discontinuation was completion of the planned 12-month study treatment (n = 33, 51.6%). In this study, 28 patients continued to receive study treatment after progression per RECIST v1.1, with a median post-progression treatment of 1.5 months (range, 0.1–10.6). During the post-progression treatment period, 6 patients had target lesions shrinkage compared with baseline and had no new lesions, and of which 1 underwent subsequent curative surgery. Data on subsequent anticancer medications during survival follow-up are summarized in Additional file 3: Table S1.
Safety run-in phaseNo DLTs were observed in the first 6 patients of the safety run-in phase. Therefore, the study combination was administered as per the planned dosage consistently throughout the entire study with lenvatinib 12 mg (body weight ≥ 60 kg) or 8 mg (body weight < 60 kg) orally taken once daily and intravenous tislelizumab 200 mg on day 1 for a 21-day treatment cycle.
EfficacyThere were 23 responders per RECIST v1.1 assessed by IRC in the first 60 patients of the EAS, which was more than the preset threshold of 18 responders based on the Simon’s two- stage design, indicating that statistical superiority of the study combination therapy over historical control lenvatinib monotherapy was achieved (p = 0.0003).
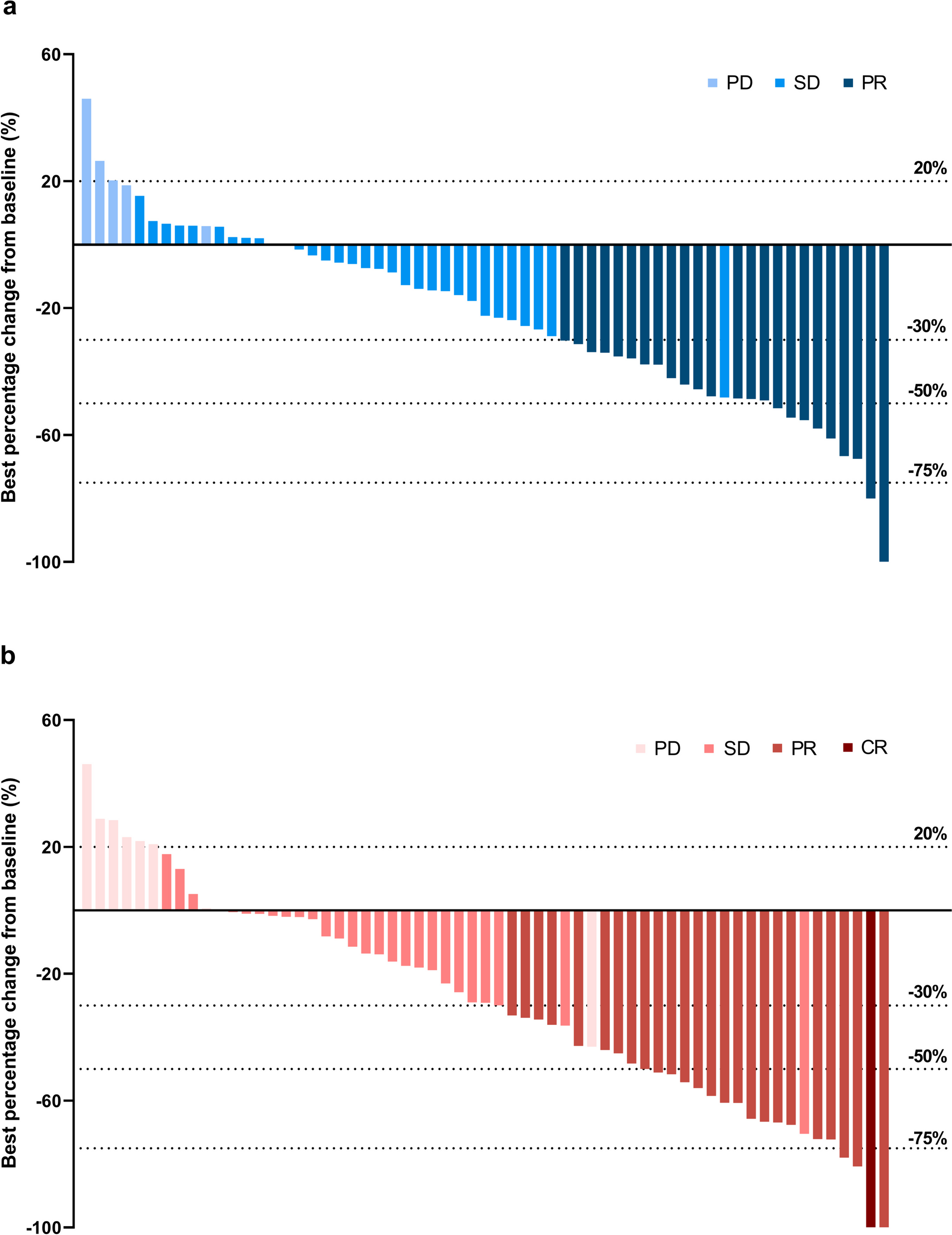
Of the total 62 patients in the EAS, confirmed ORR by IRC assessment for the primary endpoint was 38.7% (95% CI, 26.6–51.9) with 24 responders per RECIST v1.1. Confirmed ORR by IRC assessment was 46.8% (95% CI, 34.0–59.9) per mRECIST, and 38.7% (95% CI, 26.6–51.9) per iRECIST. The confirmed ORR assessed by investigators per RECIST v1.1, mRECIST and iRECIST were 41.9% (95% CI, 29.5–55.2), 46.8% (95% CI, 34.0–59.9), and 43.5% (95% CI, 31.0–56.7), respectively (Table 2). Reductions in tumor size of target lesions per RECIST v1.1 were reported in 72.6% (n = 45) of patients by IRC and 80.6% (n = 50) by investigator assessment (Fig. 1). The subgroup analysis of IRC assessed ORRs per RECIST v1.1 showed that the study treatment performed equally in patients with different prognostic features (Fig. 2).
Table 2 Tumor response by IRC and investigator review per RECIST v1.1, mRECIST and iRECIST (EAS, N = 62)Fig. 1
Best percentage change from baseline in sum of diameters of target lesions per RECIST v1.1 by a IRC review and b Investigator review (N = 62). IRC = Independent Review Committee, RECIST = Response Evaluation Criteria in Solid Tumors, PD = progressive disease, SD = stable disease, PR = partial response, CR = complete response
Fig. 2
Subgroup analysis of overall response rate per RECIST v1.1 by IRC review (N = 62). IRC = Independent Review Committee, RECIST = Response Evaluation Criteria in Solid Tumors, HBV = hepatitis B virus, ECOG PS = Eastern Cooperative Oncology Group Performance Score, BCLC = Barcelona Clinic Liver Cancer, TACE = transarterial chemoembolization, HAIC = hepatic arterial infusion chemotherapy, CI = confidence interval. Macrovascular Invasion or Extrahepatic Spread included 2 macrovascular invasion only patients, 32 extrahepatic spread only patients and 5 patients had both macrovascular invasion and extrahepatic spread
Median DoR per RECIST v1.1 was not reached by either IRC or investigator review, with the 6-month event-free rate of 88.9% (95% CI, 62.4–97.1) and 72.3% (95% CI, 50.4–85.7), respectively. Twelve-month event-free rate per RECIST v1.1 was not reached either by IRC or investigator review. DCR per RECIST v1.1 was 90.3% (95% CI, 80.1–96.4) by IRC and 85.5% (95% CI, 74.2–93.1) by investigator review (Table 2).
At the data cutoff, median PFS per RECIST v1.1 was 8.2 months (95% CI, 6.8–not estimable [NE]) by IRC and 9.6 months (95% CI, 5.3–NE) by investigator review. PFS rates at 12 months were 40.5% (95% CI, 26.2–54.2) and 43.7% (95% CI, 28.3–58.1), respectively (Fig. 3a-b). Median OS was not reached (Fig. 3c). The 6-month and 12-month OS rates were 95.2% (95% CI, 85.7–98.4) and 88.6% (95% CI, 77.7–94.4), respectively. PFS per mRECIST and iRECIST assessed by IRC or investigator review is shown in Additional file 1: Fig. S3.
Fig. 3
Kaplan–Meier plots for PFS per RECIST v1.1 and OS (N = 62). a PFS by IRC review; b PFS by investigator review; c OS. PFS = progression-free survival, OS = overall survival, IRC = independent review committee, CI = confidence interval, NE = not estimable
Safety and tolerabilityAll the 64 patients experienced at least one treatment-emergent adverse events (TEAEs), with 22 (34.4%) experiencing TEAEs of grade ≥ 3 (Additional file 3: Table S2). And 95.3% of patients reported ≥ 1 treatment-related adverse events (TRAEs); TRAEs reported in ≥ 20% of patients included proteinuria (46.9%), hypertension (35.9%), hypothyroidism (31.3%), aspartate aminotransferase increased (26.6%), platelet count decreased (23.4%), weight decreased (23.4%), and palmar-plantar erythrodysesthesia syndrome (20.3%) (Table 3). Grade ≥ 3 TRAEs occurred in 18 (28.1%) patients.
Table 3 Frequency of AEs (N = 64)Serious adverse events (SAEs) were reported in 11 (17.2%) patients; 7 (10.9%) experienced treatment-related SAEs. During the study, 3 (4.7%) deaths occurred. Two deaths were reported as unrelated to study treatments. One death was reported as treatment related. This patient received one dose of tislelizumab and 8 days of lenvatinib and died due to respiratory failure. Death was attributed to disease progression and study treatment. TRAEs leading to treatment discontinuation occurred in 3 (4.7%) patients. TRAEs led to treatment modification in 35 (54.7%) patients.
Immune-mediated adverse events (imAEs) occurred in 30 (46.9%) patients, and most were grade 1 or 2 in severity. Three (4.7%) patients with at least one imAEs received systemic corticosteroids. Grade 3 imAEs occurred in 3 (4.7%) patients (pancreatitis [n = 2, 3.1%]; enterocolitis [n = 1, 1.6%]) (Table 3). imAEs at grade 4 or higher were not observed. imAEs led to tislelizumab interruption in 7 (10.9%) patients and tislelizumab discontinuation in 1 (1.6%) patient.
留言 (0)