
記住我
As of 2020, a total of 37.7 million people were living with HIV, including 10.2 million who were not receiving treatment and 1.5 million who were newly diagnosed with HIV infection. Globally, 680,000 people die annually of HIV-related causes.1 Significant improvements in the life expectancy of HIV-infected individuals have been achieved with the introduction of universal antiretroviral therapy (ART).2 At the same time, as patients age, comorbidities often act as prognostic factors or factors that cause a decline in quality of life, and appropriate management of these comorbidities is desirable.2 The expansion of ART coverage has decreased the incidence of AIDS and AIDS-related morbidity and mortality, as well as HIV transmission.3–6
According to the Millennium Development Goals report,7 the incidence of new HIV infections declined by 40% from 2000 to 2013 worldwide. One study reported a decrease in the incidence of AIDS-defining malignancies (ADMs), namely Kaposi sarcoma, non-Hodgkin lymphoma, and invasive cervical cancer.8 Since 1998, we have conducted an annual national surveillance of opportunistic complications among people infected with HIV in Japan. In a previous report,9 we showed that the number of AIDS-defining illnesses (ADIs) has decreased continuously since 2012. Globally, as of 2020, the number of newly diagnosed patients with cancer was 19,292,789; furthermore, 9,958,133 people died from cancer.10 In Japan, as of 2018, the number of newly diagnosed patients with cancer was 980,856, and 376,425 people died from cancer.11
By contrast to the decreasing trend of ADIs and ADMs, there is a growing body of evidence supporting an increase in the incidence of non–AIDS-defining cancers (NADCs). The reasons for the increase in NADCs have been discussed using a multifactorial approach because organ-specific factors affect the pathogenesis of each cancer, such as age-matched factors, smoking status, transmission routes, contaminated blood product use, coinfection with other viruses, cigarette smoking, alcohol consumption, and advanced age.12–15
METHODS Patient GroupThis study was conducted annually, using 2 main content surveys at the same time: (1) the annual national surveillance of opportunistic complications in patients infected with HIV and (2) the annual national surveillance of NADCs. The former survey analysis was reported by us previously,9 and similarly, in this study, HIV/AIDS referral hospitals in Japan were used for the survey. As of September 2021, these hospitals were located at 378 sites throughout Japan. Since 1999, we have posted an annual questionnaire on NADCs for patients diagnosed with NADCs among individuals infected with HIV-1 from January to December of the previous year.
Questionnaire DevelopmentThe questionnaire was divided into 2 parts. The first included questions regarding the presence of patients with NADCs in each hospital. The second part gathered information regarding patients with NADCs. This included questions on the type and onset of NADCs, clusters of differentiation 4-positive (CD4+) lymphocyte levels at the onset, diagnostic procedures used for NADCs, outcomes of cancer treatment, ART initiation at the onset, elapsed time from the initial HIV diagnosis until the onset of NADCs, and ART initiation time after the diagnosis of NADCs. A detailed survey of each disease was omitted because the aim of this study was to determine the trends in patients with NADCs in Japan. Outcomes, including survival status, were recorded at the time when each physician responded to the questionnaire. Questionnaires were posted to HIV/AIDS referral hospitals throughout Japan annually for 23 years. As this surveillance was an annual report, the outcome was a clinical judgment made by each physician a year after diagnosis.
The questionnaire responses were recorded in a database created using Microsoft Access 2010 (Microsoft Corporation, Redmond, WA) for further analysis. The questionnaire was developed in accordance with the ethical guidelines for medical research targeting human subjects16 and therefore did not include identifiers such as patient initials or record numbers by which patients could be linked or identified.
Mortality RateThe mortality rate was calculated as “the accumulated number of deaths reported in the survey per accumulated number of diagnosed cancer patients.”
Capture RateThe annual capture rate was calculated on the basis of the number of AIDS cases reported to the AIDS Surveillance Committee of the Ministry of Health, Labour, and Welfare (MHLW) in Japan. The capture rate (average of the last 2 years) was calculated as the number of AIDS cases reported through our questionnaires (total number in the past 2 years) divided by the number of AIDS cases reported through the MHLW surveillance (total number in the past 2 years).
Statistical AnalysisAll data were analyzed using IBM SPSS 23 (IBM Corp, Armonk, NY). We performed an aggregate analysis in this study, in which the number of cases by the responders to the questionnaire was calculated, and the percentage of each response was examined for each year.
EthicsThe study was approved annually by the Institutional Review Board of Nagasaki University Hospital (Approval Number: 18111929-2) and by the institutional review boards of each participating hospital. Informed consent was waived in this study because the information did not include any human samples or personal information.
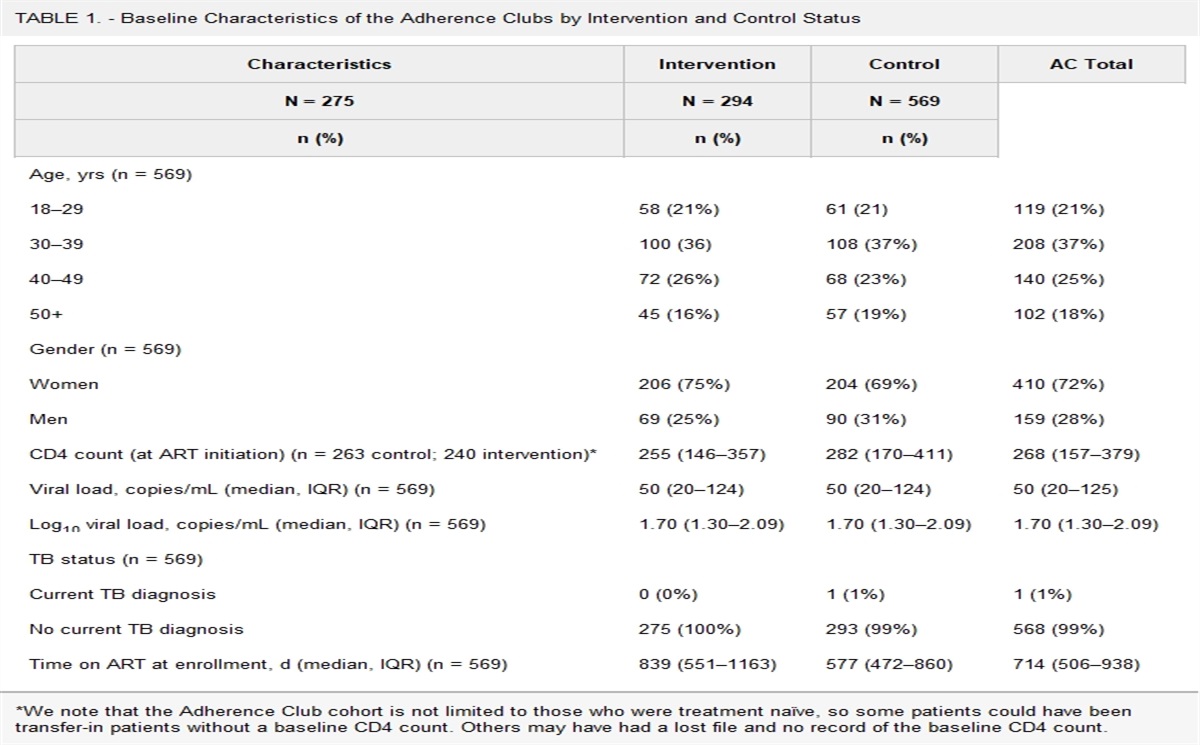
RESULTS Trends and Number of Cases of NADCsThe baseline data of the study are summarized in Table 1. The response and case-capture rates for the questionnaires in 2021 were 37.8% and 81.2%, respectively (see Table, Supplemental Digital Content 1, https://links.lww.com/QAI/C225). A total of 93% of the patients were male patients. Data of sex-specific tabulations of key data are shared in the Table, Supplemental Digital Content 2, https://links.lww.com/QAI/C226.
TABLE 1. - Baseline Study Data Research period 23 yrs (1999–2021) Number of facilities in 2021 378 Response rate in 2021 (%) 37.8 Case capture rate in 2021 (%) 81.2 Sex (%) Female (6.9)/Male (93.1)Questionnaires were posted to HIV/AIDS referral hospitals throughout Japan annually from 1995 to 2021. In 2021, questionnaires were sent to 378 hospitals, and a response rate of 37.8% (143 hospitals) was observed. In 2021, 60 cases of NADCs were reported from a total of 922 NADCs to date. In the annual occurrence of NADCs (Fig. 1A), the number of cases of NADCs increased significantly in 2000, with 8 cases compared with the previous year of 1999, which only had a few cases. After that, the number of NADCs increased every year, with approximately 40–50 cases annually after 2010, and then leveled off but reached a peak in 2017 before slightly decreasing again after 2018.
 FIGURE 1.:
FIGURE 1.: Change over time in the number of cases of NADCs (1999–2021). A, Annual number of cases of NADCs. The numbers present a continuously increasing trend since 1999. B, Case counts number of cases of NADCs. NADCs, non–AIDS-defining cancers.
The case count numbers of NADCs is shown in Figure 1B, with lung cancer being the most frequent (131 cases in total). Liver cancer was the most frequent NADC until 2009, after which its incidence declined. By contrast, lung cancer became the most frequent NADC, with an increase in the number of cases to 11 in 2010, and remained the most frequently occurring disease cumulatively, although it showed a decreasing trend after that. The proportions of each NADC in descending order were as follows: lung cancer (14.0%), colon cancer (11.9%), stomach cancer (10.5%), liver cancer (8.0%), other hematologic tumors (6.0%), anal cancer (5.9%), head and neck cancer (5.2%), other urogenital tumors (4.9%), leukemia (3.9%), laryngeal tumors (3.7%), prostate cancer (3.6%), pancreatic cancer (3.4%), skin cancer (3.0%), breast cancer (3.0%), esophageal cancer (2.5%), renal cancer (1.8%), testicular cancer (1.5%), vulvar cancer (0.9%), brain cancer (0.5%), and multiple myeloma (0.4%).
In the single-year data for 2021, there were 12 cases of colorectal cancer, 7 cases of lung cancer, 2 cases of stomach cancer, 3 cases of anal tumors, 2 cases of laryngeal cancer, 4 cases of liver cancer, and 4 cases of head and neck cancer (Figs. 2A, B). In the graphs showing the annual incidence of the 8 major diseases (Figs. 2A, B), the rapid increase in the incidence of colorectal cancer since 2009 was particularly conspicuous. Liver cancer peaked at 6 cases in 2006, then decreased, and then increased again to 11 cases in 2017, after an almost stable rate of 1–4 cases/year for the past several years.
 FIGURE 2.:
FIGURE 2.: Change over time in the incidence of each cancer (1999–2021). A, The trends observed in the incidence of 4 major cancers (1999–2021). B, The trends observed in the incidence of other cancers.
Prognosis of MalignanciesRegarding mortality, categorized according to tumor type (Fig. 3A), pancreatic cancer, which originally had a poor prognosis, had the highest mortality rate, followed by leukemia and lung, liver, laryngeal, and esophageal cancer. In patient outcomes (Fig. 3B), complete/partial remission was observed in 62% of the patients.
 FIGURE 3.:
FIGURE 3.: Mortality and morbidity of NADCs. A, Mortality in each NADC (1995–2021). B, Outcomes of NADCs.
Transmission RoutesThe annual number of NADCs, classified according to the route of infection (Fig. 4A), showed an increasing trend over time, with more cases reported in male patients who have sex with male individuals (MSM) (n = 477 cases) than in others (n = 182 cases) (Fig. 4B). The incidence of lung, colorectal, gastric, anal, and head and neck cancers was particularly high among MSM. Lung cancer was the most common in both MSM and others. Although the number of iatrogenic infections (mainly in patients with hemophilia due to contaminated blood coagulation factor products) was relatively small (n = 65), which is not included in the Figure 4 data, it is noteworthy that liver cancer accounted for approximately 50% of cases, which may be attributed to hepatitis C virus caused by blood product contamination (data not shown).
 FIGURE 4.:
FIGURE 4.: Comparison between 2 transmission routes (1999–2021). A, Trends observed in malignancies according to the 2 transmission routes. B, Number of cases of malignancies for each of the 2 transmission routes.
Age DistributionThe most common age group of tumor onset (Fig. 5A) was in the 60s, and 2.1% of patients infected with HIV were in their 80s, an age group that generally has a small population of patients infected with HIV. Compared with the age of onset of opportunistic infections,9 which is close to the age of detection in patients infected with HIV, there was a clear shift toward an older age group. There was no significant difference in age distribution by route of infection, that is, among MSM and others (Fig. 5B). Regarding age distribution by tumor, testicular tumors tended to occur at younger ages; head and neck tumors, anal tumors, and leukemia were more common in the middle-aged group; and laryngeal, liver, colon, stomach, and lung cancers were more common in the older group (Fig. 5C).
 FIGURE 5.:
FIGURE 5.: Age distribution in NADCs (1999–2021). A, Age distribution at the onset of malignancies. B, Age distribution in each infection route at the onset of malignancies. C, Age distribution in each malignancy at the onset of malignancies.
Distribution of CD4+ Lymphocytes and Time From DiagnosisThe distribution of CD4+ lymphocytes in peripheral blood at the time of cancer diagnosis showed a trend toward a higher number of patients with lower CD4+ lymphocyte counts (see Figure A, Supplemental Digital Content 3, https://links.lww.com/QAI/C227). The distribution of CD4+ lymphocytes in major malignancies is shown in Figure B, Supplemental Digital Content 3, https://links.lww.com/QAI/C227. Regardless of the tumor type, CD4+ lymphocytes were widely distributed, with no CD4 bias in any particular tumor. The onset of tumor development occurred more than 1 year after HIV diagnosis in 80% of all patients infected with HIV (see Figure C, Supplemental Digital Content 3, https://links.lww.com/QAI/C227). By contrast, in more than 80% of patients with opportunistic infections, tumor development occurred within 3 months (including simultaneous detection).9 Specifically, tumor development occurred after a period of time had elapsed since the diagnosis of HIV.
DISCUSSIONIn this study, we investigated the prevalence and long-term trends of NADCs among patients with HIV in Japan from 1999 to 2021. For patients infected with HIV in Japan, most treatments for complications, including malignancies, are provided at HIV/AIDS referral hospitals. Thus, the results of this survey provided a comprehensive picture of malignant tumors among such patients in Japan.
With the introduction of ART, the long-term prognosis of patients infected with HIV has improved,1 and the occurrence of malignant tumors has become a cause for concern.12,13 Furthermore, as conventional infection-linked cancers, NADCs have higher mortality rates than ADIs and have recently been the focus of attention because the disease burden has increased over time.17–21 Data on the incidence trends of NADCs have been reported from several countries22–27; however, there is a paucity of published data originating from Japan.28,29
This study highlighted several interesting characteristics of NADCs in Japan, categorized according to trends and number of cases, prognosis, transmission routes, age distribution, and CD4+ lymphocyte distribution. In our study, the number of NADCs among patients infected with HIV in Japan was found to have increased over time. To prevent the duplication of cases, the target year was specified in the questionnaire form to avoid confusion when surveying newly diagnosed cases for each year in the annual questionnaire. The theoretical possibility exists that duplicate enrollment is possible when patients are transferred between HIV/AIDS referral hospitals. However, in Japan, all the HIV/AIDS referral hospitals are high care medical institutions that are able to provide most of the specialized services; thus, transferring cases between these facilities is rare.
In Japan, the number of newly reported cases of HIV infection or AIDS has peaked, based on the Infectious Disease Surveillance System for HIV/AIDS diagnosis by the MHLW of Japan (see Table, Supplemental Digital Content 4, https://links.lww.com/QAI/C228). The increasing trend in NADC case counts may be related to an aging population of people living with HIV who acquired the infection in the 1990s/early 2000s, which explains why cases accumulated over time and why most individuals were aged in their 60s.
The distribution of cancer among patients infected with HIV clearly differed from the general tumor frequency in the Japanese population. Cancer incidence data among the general population in Japan were collected using the National Cancer Registry system, and data for the year 2018 are available on the website.30 When the Japanese epidemiological data were compared with the results of our study, anal (<1% vs. 5.9%, respectively), testicular (<1% vs. 1.5%, respectively), and laryngeal cancer (<1% vs. 3.7%, respectively) were found to be more common in our survey on patients infected with HIV. Cancer types that were infrequent in the general population were relatively common in our study, and diversity was observed. Moreover, 22 cancer types were identified in our survey. Excluding the major cancers (lung, colon, stomach, and liver), 18 other cancer types constituted 55.6% of all NADCs, which is similar to the proportion of 55.2% reported in the Japanese epidemiological data. Although it was difficult to determine whether there was a significant difference in the frequency of each cancer type because the overall number was not large, this trend of diversity is noteworthy, and the data may suggest that HIV infection itself is related to cancer immunity.
The fact that the proportion of cancer cases in MSM was higher than that of others may also be a factor. However, different types of cancer in HIV-positive populations may reflect a phenomenon affecting cancer immunity. The well-known human oncoviruses are human papillomavirus (HPV), hepatitis B virus, hepatitis C virus, Epstein–Barr virus, human herpesvirus 8, human T-cell lymphotropic virus, and Merkel cell polyomavirus.31 Epstein–Barr virus has been implicated in the pathogenesis of Burkitt lymphoma, Hodgkin disease, non-Hodgkin lymphoma, nasopharyngeal carcinoma, lymphomas, and leiomyosarcomas32,33; HPV with anal, laryngeal, and recently lung cancer34–36; and hepatitis B virus and hepatitis C virus with liver cancer.37 No association with viral infection has been found in other types of cancer, such as colon cancer.
According to the Department of Health and Human Services guidelines,38 HPV vaccination is beneficial and is recommended for the age group of 13–26 years because they may have sexual contact; moreover, vaccination for those older than 27 years is deprecated because of low benefits. Although HPV vaccination for male patients has not gained momentum,39–42 vaccination of patients younger than 26 years is recommended, given the risk of HPV-related malignancies. Therefore, with the introduction of the HPV vaccine, analysis of future trends in the prevalence of anal or laryngeal cancer can help determine the vaccination effect.
An increase in the incidence of lung cancer has been noticeable over the past few years. In 2014, a report from the United States documented a notable increase in anal, liver, and prostate cancers.22 A 2014 report from France also documented that lung and anal cancer rates have decreased since the beginning of the ART era.23 A single-center study in Japan reported an increased risk of liver and colorectal cancers, while the risk of gastric cancer, which is common in Japan, also increased.29 As a projection of future frequencies, a study from the United States predicted a rise in prostate and lung cancers by 2030.43 Continuous monitoring of the frequency of occurrence of NADCs is important because various factors are related to the occurrence of malignant tumors, including lifestyle variations in various countries.
Smoking is a pivotal factor in the development of malignancies. The average smoking rate among the general Japanese population from the 2019 national survey by the MHLW was 27.1% for male patients and 7.6% for female patients.44 A Japanese single-center study in 2011 analyzed 149 HIV-positive patients and reported a smoking rate of 42.2%.45 Because the average smoking rate in Japan in 2011 was 32.4% for male patients and 9.7% for female patients, it can be said that the smoking rate among patients infected with HIV in Japan is higher than that in the general population. Although there are no clear data, it is possible that factors contributing to the incidence of lung and laryngeal cancers, such as smoking, are higher among individuals with infected HIV, especially MSM, and the promotion of smoking cessation among individuals infected with HIV will be an important issue in the future. Smoking is also a high-risk factor of malignant tumors other than lung cancer (genitourinary system and throat cancers), and future trends should be closely monitored.
Considering the factors that contribute to the development of malignancies in patients with HIV, it would be reasonable to compare them with malignancies in other immunosuppressed populations. There is growing evidence of increased cancer incidence in immunosuppressed patients.46,47 As for the association with CD4+ lymphocyte counts, our present findings did not suggest an association; however, previous reports have shown that lower CD4+ lymphocyte counts are associated with lower survival rates.48,49 In addition to the association between HIV and the development of cancer based on conventional epidemiological information, recent studies have reported an association between HIV-derived microRNAs and interactions with tumorigenesis.22,50 This microRNA evidence may prove a link to malignancies that have been identified from previous ADIs. It is also expected that associations with malignancies not previously recognized as infection-linked cancers will be proven. Future advances in microRNA functional analyses may reveal a direct association between the target genes and tumorigenesis, which is impaired by age, smoking history, and other known risk factors.
In future HIV care, in addition to controlling antiviral therapy and paying attention to metabolic complications, it is important to conduct regular screening for the early detection of malignant tumors.51–54 The results of this study emphasize the need for screening for malignant tumors by focusing on the risk of acquiring certain cancers according to age. However, our results and previous reports suggest that patients infected with HIV may have a wide variety of malignant tumors and that it is difficult to detect all of them by commonly used cancer screening.55 To cope with the rapid increase in the number of cancers due to the aging of patients infected with HIV, there is an urgent need to develop screening and preventive methods for malignant tumors.20
In the epidemiological context of HIV in Japan, intravenous (IV) drug users account for a very small proportion of all blood-borne infection routes (see Table, Supplemental Digital Content 5, https://links.lww.com/QAI/C229). In these data, not a single case of IV drug use corresponded to this category. However, owing to the overlap of infection routes (MSM + IV drug use), it is possible that the IV drug use infection route in Japan is underestimated.
The retrospective design of this study had some limitations. First, a response rate of 37.8% from all HIV/AIDS referral hospitals may have led to a selection bias. However, most of the high-volume centers in each region of Japan responded to our survey every year, and the case capture rate of HIV/AIDS cases was 81.2%; therefore, we do not believe that there was a large selection bias. Second, the context of the questions was minimized for simplicity and ease of completion; therefore, the background information of patients was inadequate for performing additional analyses. Third, the calculation of the mortality rate in this study was not performed in accordance with the standard evaluation method; however, the percentage of annual deaths in the applicable year of the study period could be collected because of the limited information requested in the questionnaire. Fourth, although information on the time of diagnosis of malignancy was included in the questionnaire items, the time of ART initiation and the duration of ART were not included as information items. Therefore, it was not possible to analyze the relationship between ART and the risk of malignancy. Finally, there was the possibility of missing data for patients who received NADC treatment outside HIV/AIDS referral hospitals. In Japan, under the health care system, most patients with HIV/AIDS are managed at HIV/AIDS referral hospitals. Patients are rarely managed at hospitals other than the HIV/AIDS referral hospital. The HIV/AIDS referral hospitals provide both primary care and HIV management for people living with HIV, as outpatients and inpatients. Based on the above, it is assumed that most of the patients with NADCs in Japan are captured by this surveillance, based on the number of cases at HIV/AIDS referral hospitals in Japan.
In conclusion, our data, based on high-volume information obtained through annual national surveillance, clarified accurate 21-year trends in NADC status and occurrence in Japan. Our survey is a valuable resource because it collected serial data from across Japan. As changing lifestyles and social backgrounds are elements that influence the occurrence of malignancies to some extent, continuous surveillance is warranted to obtain future trends and disease outcomes.
ACKNOWLEDGMENTSThe cooperation of all personnel involved in the participating HIV/AIDS referral hospitals made it possible to continue the study every year. The authors express their deepest gratitude to them for their support in the survey, which they provided while encumbered with the increasing burden of duties. The authors would like to thank Editage (www.editage.com) for English language editing.
REFERENCES 1. UN AIDS. Global HIV & AIDS Statistics—Fact Sheet. Available at: https://www.unaids.org/en/resources/fact-sheet. Accessed February 21, 2024. 2. Marcus JL, Leyden WA, Alexeeff SE, et al. Comparison of overall and comorbidity-free life expectancy between insured adults with and without HIV infection, 2000-2016. JAMA Netw Open. 2020;3:e207954. 3. Samji H, Cescon A, Hogg RS, et al. Closing the gap: increases in life expectancy among treated HIV-positive individuals in the United States and Canada. PLoS ONE. 2013;8:e81355. 4. Grinsztejn B, Hosseinipour MC, Ribaudo HJ, et al. Effects of early versus delayed initiation of antiretroviral treatment on clinical outcomes of HIV-1 infection: results from the phase 3 HPTN 052 randomised controlled trial. Lancet Infect Dis. 2014;14:281–290. 5. Montaner JS, Lima VD, Harrigan PR, et al. Expansion of HAART coverage is associated with sustained decreases in HIV/AIDS morbidity, mortality and HIV transmission: the “HIV Treatment as Prevention” experience in a Canadian setting. PLoS ONE. 2014;9:e87872. 6. Cohen MS, Chen YQ, McCauley M, et al. Prevention of HIV-1 infection with early antiretroviral therapy. N Engl J Med. 2011;365:493–505. 7. Prendergast AJ, Essajee S, Penazzato M. HIV and the millennium development goals. Arch Dis Child. 2015;100(suppl 1):S48–S52. 8. Bedimo RJ, McGinnis KA, Dunlap M, et al. Incidence of non-AIDS-defining malignancies in HIV-infected versus noninfected patients in the HAART era: impact of immunosuppression. J Acquir Immune Defic Syndr. 2009;52:203–208. 9. Tanaka T, Oshima K, Kawano K, et al. Nationwide surveillance of AIDS-defining illnesses among HIV patients in Japan from 1995 to 2017. PLoS ONE. 2021;16:e0256452. 11. International Agency for Research on Cancer, WHO. Global Cancer Observatory. Available at: https://gco.iarc.fr/. Accessed February 21, 2024. 12. Shiels MS, Engels EA. Evolving epidemiology of HIV-associated malignancies. Curr Opin HIV AIDS. 2017;12:6–11. 13. Yarchoan R, Uldrick TS. HIV-associated cancers and related diseases. N Engl J Med. 2018;378:1029–1041. 14. Spano JP, Poizot-Martin I, Costagliola D, et al. Non-AIDS-related malignancies: expert consensus review and practical applications from the multidisciplinary CANCERVIH Working Group. Ann Oncol. 2016;27:397–408. 15. Brugnaro P, Morelli E, Cattelan F, et al. Non-AIDS definings malignancies among human immunodeficiency virus-positive subjects: epidemiology and outcome after two decades of HAART era. World J Virol. 2015;4:209–218. 16. Ministry of Health, Labour and Welfare, Japan. Ethical Guidelines for Medical and Health Research Involving Human Subjects. Available at: https://www.mhlw.go.jp/file/06-Seisakujouhou-10600000-Daijinkanboukouseikagakuka/0000080278.pdf. Accessed February 21, 2024. 17. Castilho JL, Luz PM, Shepherd BE, et al. HIV and cancer: a comparative retrospective study of Brazilian and U.S. clinical cohorts. Infect Agent Cancer. 2015;10:4. 18. Engels EA, Yanik EL, Wheeler W, et al. Cancer-attributable mortality among people with treated human immunodeficiency virus infection in North America. Clin Infect Dis. 2017;65:636–643. 19. Horner MJ, Shiels MS, Pfeiffer RM, et al. Deaths attributable to cancer in the US human immunodeficiency virus population during 2001-2015. Clin Infect Dis. 2021;72:e224–e231. 20. Zucchetto A, Virdone S, Taborelli M, et al. Non-AIDS-defining cancer mortality: emerging patterns in the late HAART era. J Acquir Immune Defic Syndr. 2016;73:190–196. 21. Nishijima T, Inaba Y, Kawasaki Y, et al. Mortality and causes of death in people living with HIV in the era of combination antiretroviral therapy compared with the general population in Japan. AIDS. 2020;34:913–921. 22. Robbins HA, Shiels MS, Pfeiffer RM, et al. Epidemiologic contributions to recent cancer trends among HIV-infected people in the United States. AIDS. 2014;28:881–890. 23. Hleyhel M, Hleyhel M, Bouvier AM, et al. Risk of non-AIDS-defining cancers among HIV-1-infected individuals in France between 1997 and 2009: results from a French cohort. AIDS. 2014;28:2109–2118. 24. Chiu CG, Smith D, Salters KA, et al. Overview of cancer incidence and mortality among people living with HIV/AIDS in British Columbia, Canada: implications for HAART use and NADM development. BMC Cancer. 2017;17:270. 25. Chen M, Jen I, Chen YH, et al. Cancer incidence in a Nationwide HIV/AIDS patient cohort in Taiwan in 1998–2009. J Acquir Immune Defic Syndr. 2014;65:463–472. 26. Zhu W, Mao Y, Tang H, et al. Spectrum of malignancies among the population of adults living with HIV infection in China: a nationwide follow-up study, 2008–2011. PLoS ONE. 2019;14:e0219766. 27. Lee S, Lee SH, Lee JE, et al. Trends in malignancies among Korean patients infected with human immunodeficiency virus in the highly active antiretroviral therapy era. J Korean Med Sci. 2017;32:1445–1450. 28. Oka S, Ogata M, Takano M, et al. Non-AIDS-defining malignancies in Japanese hemophiliacs with HIV-1 infection. Glob Health Med. 2019;1:49–54. 29. Nagata N, Nishijima T, Niikura R, et al. Increased risk of non-AIDS-defining cancers in Asian HIV-infected patients: a long-term cohort study. BMC Cancer. 2018;18:1066. 30. National Cancer Centre Japan. Cancer Information. Available at: https://ganjoho.jp/reg_stat/statistics/stat/summary. Accessed February 21, 2024. 31. Schiller JT, Lowy DR. An introduction to virus infections and human cancer. Recent Results Cancer Res. 2021;217:1–11. 32. Thompson MP, Kurzrock R. Epstein-Barr virus and cancer. Clin Cancer Res. 2004;10:803–821. 33. Chakravorty S, Afzali B, Kazemian M. EBV-associated diseases: current therapeutics and emerging technologies. Front Immunol. 2022;13:1059133. 34. Wang CJ, Palefsky JM. HPV-associated anal cancer in the HIV/AIDS patient. Cancer Treat Res. 2019;177:183–209. 35. Colón-López V, Shiels MS, Machin M, et al. Anal cancer risk among people with HIV infection in the United States. J Clin Oncol. 2018;36:68–75. 36. Tsyganov MM, Pevzner AM, Ibragimova MK, et al. Human papillomavirus and lung cancer: an overview and a meta-analysis. J Cancer Res Clin Oncol. 2019;145:1919–1937. 37. McGlynn KA, Petrick JL, El-Serag HB. Epidemiology of hepatocellular carcinoma. Hepatology. 2021;73(suppl 1):4–13. 38. Clinical Info HIV. Adult and Adolescent ARV—What's New in the Guidelines? Available at: https://clinicalinfo.hiv.gov/en/guidelines/hiv-clinical-guidelines-adult-and-adolescent-arv/whats-new. Accessed February 21, 2024. 39. Meites E, Wilkin TJ, Markowitz LE. Review of human papillomavirus (HPV) burden and HPV vaccination for gay, bisexual, and other men who have sex with men and transgender women in the United States. Hum Vaccin Immunother. 2022;18:2016007. 40. Budenz A, Klassen A, Leader A, et al. HPV vaccine, Twitter, and gay, bisexual and other men who have sex with men. Health Promot Int. 2020;35:290–300. 41. Stanley M. HPV vaccination in boys and men. Hum Vaccin Immunother. 2014;10:2109–2111. 42. Grandahl M, Nevéus T. Barriers towards HPV vaccinations for boys and young men: a narrative review. Viruses. 2021;13:1644. 43. Shiels MS, Islam JY, Rosenberg PS, et al. Projected cancer incidence rates and burden of incident cancer cases in HIV-infected adults in the United States through 2030. Ann Intern Med. 2018;168:866–873. 44. Ministry of Labour, Health and Welfare, Japan. National Health and Nutrition Survey. Available at: https://www.mhlw.go.jp/bunya/kenkou/kenkou_eiyou_chousa.html. Accessed February 21, 2024. 45. Hikasa S, Yasuda M, Hikasa S, et al. Smoking Prevalence and Effects of Smoking on Lipid Metabolism in Japanese HIV-Infected Patients (Program and Abstracts of the Annual Meeting of the Japan Society for Tobacco Control) [abstract in Japanese]. Available at: https://jglobal.jst.go.jp/detail?JGLOBAL_ID=201202223594028500&rel=1#%7B%22category%22%3A%220%22%2C%22keyword%22%3A%22201202223594028500%22%7D. Accessed February 21, 2024. 46. Kinlen L. Infections and immune factors in cancer: the role of epidemiology. Oncogene. 2004;23:6341–6348. 47. Grulich AE, van Leeuwen MT, Falster MO, et al. Incidence of cancers in people with HIV/AIDS compared with immunosuppressed transplant recipients: a meta-analysis. Lancet. 2007;370:59–67. 48. Gotti D, Raffetti E, Albini L, et al. Survival in HIV-infected patients after a cancer diagnosis in the cART Era: results of an Italian multicenter study. PLoS ONE. 2014;9:e94768. 49. Zhang S, van Sighem A, Kesselring A, et al. Risk of non-AIDS-defining events among HIV-infected patients not yet on antiretroviral therapy. HIV Med. 2015;16:265–272. 50. Zhao T, Chen W, Zhang X, et al. HIV-induced cancer—all paths leading to Rome. Microb Pathog. 2020;139:103804. 51. Corrigan KL, Wall KC, Bartlett JA, et al. Cancer disparities in people with HIV: a systematic review of screening for non-AIDS-defining malignancies. Cancer. 2019;125:843–853. 52. Thrift AP, Chiao EY. Are non-HIV malignancies increased in the HIV-infected population? Curr Infect Dis Rep. 2018;20:22. 53. Franzetti M, Ricci E, Bonfanti P. The pattern of non-AIDS-defining cancers in the HIV population: epidemiology, risk factors and prognosis. A review. Curr HIV Res. 2019;17:1–12. 54. Lurain K, Yarchoan R, Ramaswami R. The changing face of HIV-associated malignancies: advances, opportunities, and future directions. Am Soc Clin Oncol Educ Book. 2019;39:36–40. 55. Shiels MS, Althoff KN, Pfeiffer RM, et al. HIV infection, immunosuppression, and age at diagnosis of non-AIDS-defining cancers. Clin Infect Dis. 2017;64:468–475.
留言 (0)