
記住我
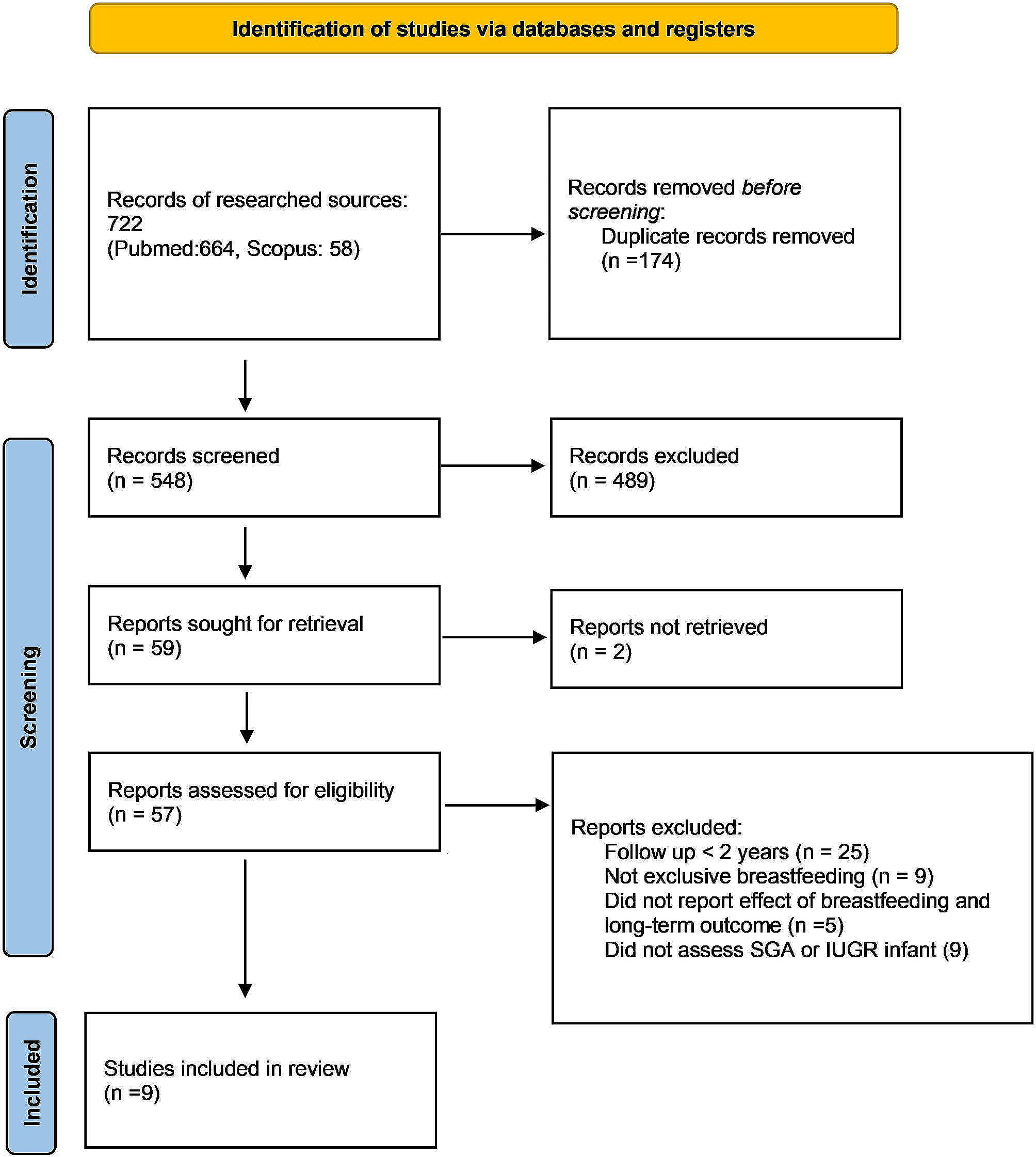

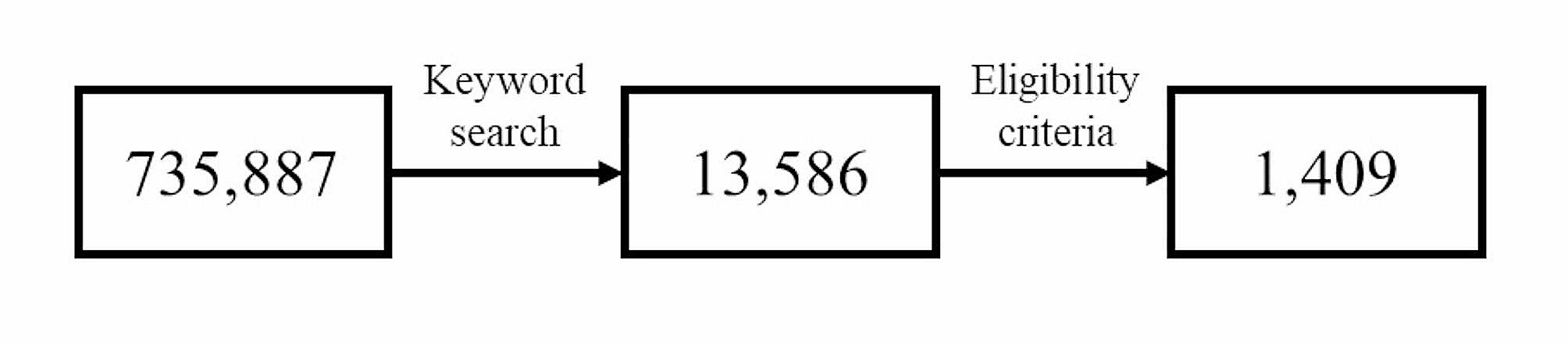


The present study used cross-sectional data from the 2020–2021 National Survey of Children’s Health (NSCH), which is funded and directed by the Health Resources and Services Administration’s Maternal and Child Health Bureau [16]. The NSCH is designed to generate national and state-level data on the physical and emotional health of children in the United States aged 0–17 years. The NSCH (2020–2021) had a total of 93,669 completed surveys with an overall weighted response rate of 42.4% for 2020 (N = 42,777) and 40.3% for 2021 (N = 50,892). Participants with missing values of study variables were excluded, leaving a final analysis sample of 85,314 children. The flow of participant screening and the frequency of missing values are illustrated in Fig. 1.
Fig. 1
Flow chart showing the patient selection process and analysis in the observational study
Sampling methods and proceduresIn this survey, randomly selected households were contacted by mail, web, or paper (offered in both English and Spanish). In each household with children aged < 18 years old, one child was randomly chosen for participation in the survey. The survey oversampled children with special health care needs and children aged 0–5 years. Additional information regarding sampling, administration, and methodology of the NSCH can be found on the Data Resource Center website [17].
Variables and data sourcesThe interest variable, congenital heart condition, was assessed based on the question, “Was this child born with the condition?” If the respondents answered “yes” to this question, the child was categorized as “yes” and “no” otherwise. In addition, respondents who answered “yes” were further asked whether the child currently has the condition, and, if so, the severity level was assessed with the question, “If yes, is it mild, moderate, or severe?” The variables of the heart condition currently and severity of current heart condition were based on these two questions, respectively. Children with current heart conditions were classified as mild, moderate, or severe based on their responses.
Autism, the outcome variable of the study, was assessed based on the question, “Has a doctor or other health care provider ever told you that this child has autism or ASD? Include diagnoses of Asperger’s disorder or pervasive developmental disorder.” ADHD, another outcome variable, was assessed based on the question, “Has a doctor or other health care provider ever told you that this child has attention deficit disorder or attention deficit/hyperactivity disorder, that is, ADD or ADHD?” Intellectual disability, another outcome variable, was assessed based on the question, “Has a doctor, other health care provider, or educator ever told you that this child has an intellectual disability (formerly known as mental retardation)?” Speech or language disorder, another outcome variable, was assessed based on the question, “Has a doctor, other health care provider, or educator ever told you that this child has a speech or other language disorder?” The child was categorized as “yes” or “no” based on the responses to all the above-mentioned questions.
Based on the risk factors for NDDs, we examined the following covariates as potential confounding variables: maternal age, birth weight (in ounces), concussion or brain injury, preterm birth, cerebral palsy, Down syndrome, and other genetic or inherited conditions. Demographic variables including age (in years), race (classified as Hispanic; White, non-Hispanic; Black, non-Hispanic; Asian, non-Hispanic; American Indian or Alaska Native Non-Hispanic; Multi-Race Non-Hispanic), and gender were also included as covariates.
MR analysisWe conducted a two-sample MR analysis using summary-level genome-wide association study statistics data. The datasets for genetic associations with congenital heart conditions were obtained from FinnGen, which included 3,42,499 individuals of European ancestry (3,459 cases and 3,39,040 controls). Instrumental variables were selected based on the following criteria: (i) associated at the level of genome-wide significance (p < 5 × 10− 6); (ii) linkage disequilibrium r2 < 0.001; (iii) < 5000 KB from the index variant. A total of 14 single-nucleotide polymorphisms (SNPs) were identified and listed in Supplementary Table 1.
The outcome data for NDDs were obtained from different sources, including the Integrative Psychiatric Research-Psychiatric Genomics Consortium (18,382 cases and 27,969 controls) for ASD [18], the Psychiatric Genomics Consortium (20,183 cases and 35,191 controls) for ADHD [19], the Social Science Genetic Association Consortium (12,441 individuals) for childhood intelligence [20], and FinnGen (2,288 cases and 25,4976 controls) for speech and linguistic disorders (Supplementary Table 2). European pedigree population data were restricted to reduce the bias caused by population level.
Statistical analysisObservational analyses were conducted based on NSCH 2020–2021 data. Continuous data were expressed as mean ± standard deviation or median (interquartile range) (for skew distributional data). The t-test or nonparametric rank-sum test, was performed to compare the differences between the groups with and without NDDs. Categorical data are described by frequency, and the differences between groups were compared using χ2 or Fisher exact test. To estimate the association between each factor and outcome, univariate and multivariable logistic regression analysis was used, with NDDs as the outcome variable and study and confounding variables (inclusion of NDDs other than outcomes) as explanatory variables. Multivariate adjusted odds ratios (ORs), 95% confidence intervals (Cis), and p-values were calculated. To reduce the impact of confounding variables and selection bias on results, PSM was also used to match case groups to control groups. Demographic variables (age, race, and gender), confounding variables (maternal age, birth weight, concussion or brain injury, preterm birth, cerebral palsy, Down syndrome, and other genetic or inherited conditions), and NDDs (other than outcomes) were used as covariates in the PSM model, using 1:1 nearest-neighbor matching techniques with a 0.01 caliper level. In the matched samples, NDDs were the outcome variable, and heart condition-related variables (congenital heart condition, current heart condition, and its severity) were the explanatory variables. A p-value of < 0.05 indicates a statistically significant difference.
In the MR analyses, we used inverse variance-weighted measures (IVW-MR), weighted median, and MR-Egger to estimate causal effects, and results are presented as ORs with 95% CIs per standard deviation increment in exposures. The F-statistic was employed to assess the strength of the instrument, and a value of at least 10 indicates weak instrument bias [21]. Additionally, we conducted several sensitivity analyses, including MR-Egger regression, MR Pleiotropy Residual Sum and Outlier (MR-PRESSO) method, to investigate the possibility of horizontal pleiotropy (p < 0.05) [22, 23]. The Cochran Q test in the IVW-MR method was performed to determine heterogeneity (p < 0.05) [24]. We further conducted a leave-one-out analysis and made a scatter plot to visually examine possible outliers. All analyses were performed using R (version 4.2.2) and the following packages: dplyr, MatchIt, cobalt, gmodels, ggplot2, knitr, kableExtra, tableone, survey, reshape2, and TwoSampleMR.
Research restrictionsWe recognize that there are some restrictions in this study. First of all, due to the relatively low incidence of severe CHD, the sample volume of some study variables may be small. Secondly, the data sources adopted by this research may have problems with insufficient information in some aspects, such as surgical methods for CHD. In the end, although MR analysis can reduce confusion, there are still some assumptions and limitations. These restrictions will be fully discussed in the conclusion and provide inspiration for future research.
Ethical statementThis study was approved by the Ethics Committee of Anhui children’s Hospital (approval no. EYLL-2022-020). This study involved secondary analysis using data from genome-wide association studies and the National Survey of Children’s Health (2020–2021). The participants had granted written informed consent before either study started. We confirm that all methods were performed in accordance with the ethical standards as laid down in the Declaration of Helsinki and its later amendments or comparable ethical standards.
留言 (0)