
記住我

Up to June 2022, 692 FMF patients, 59 MKD patients, and 49 TRAPS patients were included in the JIR Cohort in France based on clinical diagnoses. The proportion of patients who received canakinumab was 4.8% of FMF patients (n = 33), 47.5% of MKD patient (n = 28), and 14.3% of TRAPS patients (n = 7). Two FMF patients and two MKD patients were excluded from this analysis as they received canakinumab in a clinical trial setting. The first patients treated with canakinumab in the JIR cohort initiated it in 2009, 2010 and 2015 in FMF, MKD and TRAPS indications respectively. 35.5% of FMF patients, 73.1% of MKD patients and 42.9% of TRAPS patients initiated canakinumab prior to the reimbursement in these indications in France (November 2017). The median follow-up in this interim analysis was 3.1 years (range: 0.2–12.0) for FMF patients, 4.6 years (range: 0.0-11.7) for MKD patients and 2.7 years (range: 0.5–6.2) for TRAPS patients.
Characteristics of patients treated with canakinumab in real life practicePatients’ characteristics are presented in Table 1. The median age at canakinumab initiation was 14.4 years in FMF patients (16 children (i.e. <18 years old) and 15 adults), 9.7 years in MKD patients (18 children and 8 adults), and 18.9 years in TRAPS patients (3 children and 4 adults). The proportion of female patients was of 80.7%, 65.4%, and 42.9% in FMF, MKD, and TRAPS cohorts respectively.
The median age at symptom onset was 3.0 years in FMF patients, 0.5 year in MKD patients, and 3.0 years in TRAPS patients. The median diagnostic delay was 1.3 years, 2.8 years, and 11.4 years in FMF, MKD, and TRAPS cohorts respectively.
In the FMF cohort, most of the patients (93.6%) carried homozygous mutation in the exon 10 of MEFV (M694I, M694V, and M680I). In the MKD cohort, 80.8% were homozygous or composite heterozygous for class 4 and 5 variants in the MVK gene. In the TRAPS cohort, 71.4% were heterozygous for class 4 and 5 variants in the TNFRSF1A gene.
Three FMF patients (9.7%) and one TRAPS patient (14.3%) had been diagnosed with AA amyloidosis prior to canakinumab initiation.
Among FMF, MKD, and TRAPS cohorts respectively, 48.4%, 53.8%, and 28.6% of the patients were naïve of biotherapy. On the contrary, 48.4%, 38.5% and 71.4% of them had received anakinra prior to canakinumab.
In the FMF cohort, most of the patients (90.3%) were on colchicine treatment, and 83.9% of them continued it after starting canakinumab. The median dose of colchicine was 1.5 mg/day prior to canakinumab initiation and 1.0 mg/day after canakinumab initiation. Patients without colchicine prior to canakinumab initiation were all receiving anakinra.
The lack of effectiveness of colchicine was the main reported reason for canakinumab initiation in biotherapy-naïve FMF patients (55.5%, 5/9). Canakinumab was initiated due to the lack of effectiveness of anakinra in almost half of the FMF patients switching from anakinra to canakinumab (46.1%, 6/13). Two patients switched from anakinra to canakinumab due to AEs.
In the MKD cohort, the main reported reasons for canakinumab initiation was the first line maintenance (52.6%, 10/19) and the lack of effectiveness of previous treatment (31.6%, 6/19). The impossibility to maintain previous treatment (40.0%, 2/5) was the main rationale in TRAPS patients.
Table 1 Baseline characteristics of patients initiating canakinumab in FMF, MKD and TRAPSCanakinumab posology at the time of treatment initiationThe dose of canakinumab at initiation was missing for three FMF patients (1 adult and 2 children) and six MKD pediatric patients. Most of the patients in all three indications initiated canakinumab at the recommended dose of 2 mg/kg or 150 mg (85.7% of FMF, 65.0% of MKD, and 85.7% of TRAPS). All patients over 40 kg in FMF, MKD, and TRAPS indications started canakinumab with a dose of 150 mg per injection. More than half (58.3%) of the MKD patients and one-fifth (21.4%) of the FMF patients weighing less than 40 kg initiated canakinumab with a dose superior to 2.5 mg/kg (two with 2.5–3.5 mg/kg, 3 with 3.5–4.5 mg/kg and 5 with a dose of 150 mg).
The frequency of injections at initiation was broadly similar among FMF and MKD with less than half of the patients initiating canakinumab at the recommended dose interval of 4 weeks (45.2% and 34.6% respectively) and more than one-third initiating canakinumab every 8 weeks (35.5% and 38.5%). Two of the eight adult MKD patients initiated canakinumab with a dose interval inferior to 4 weeks. The proportion of patients initiated at the recommended dose interval of 4 weeks was slightly higher after November 2017 (65% of FMF and 42.9% of MKD). Among TRAPS patients, 57.1% (4 patients) initiated canakinumab every 4 weeks and 42.9% (3 patients) every 8 weeks. One FMF patient and one MKD patient were treated on demand.
Canakinumab persistence and reason of discontinuationTwo years after canakinumab initiation, the rate of patients still treated was 78.1% (95%CI: 57.2–89.6) in FMF patients, 73.7% (50.5–87.2) in MKD patients, and 85.7% (33.4–97.9) in TRAPS patients.
Overall, 19 patients (8 FMF, 10 MKD, and 1 TRAPS) discontinued canakinumab during the study period. Of those, 13 discontinued it within the first 2 years following initiation (6 FMF, 6 MKD, and 1 TRAPS). Four patients (3 FMF and 1 TRAPS) (6.2%) discontinued canakinumab after the first injection: two due to AEs (respiratory tract infections) and two due to other reasons (weight gain and post-renal transplantation infection risk with IL-1 inhibitors). The reasons for discontinuation in the remaining FMF patients were remission (as reported by clinicians) for four patients and lack of effectiveness for one patient. The main reason for discontinuation in MKD patients was lack of effectiveness (80.0%, 8/10).
Three of the eight FMF patients and eight of the 10 MKD patients restarted canakinumab during the study period. Of the three FMF patients who restarted canakinumab, one restarted it less than one year after the initial discontinuation. The median time to restart canakinumab in MKD patients was 2.7 years.
Evolution of posology during canakinumab treatmentWhile the dose of canakinumab per injection remained globally the same over the course of canakinumab treatment in all indications, we observed some adjustments of the dose intervals.
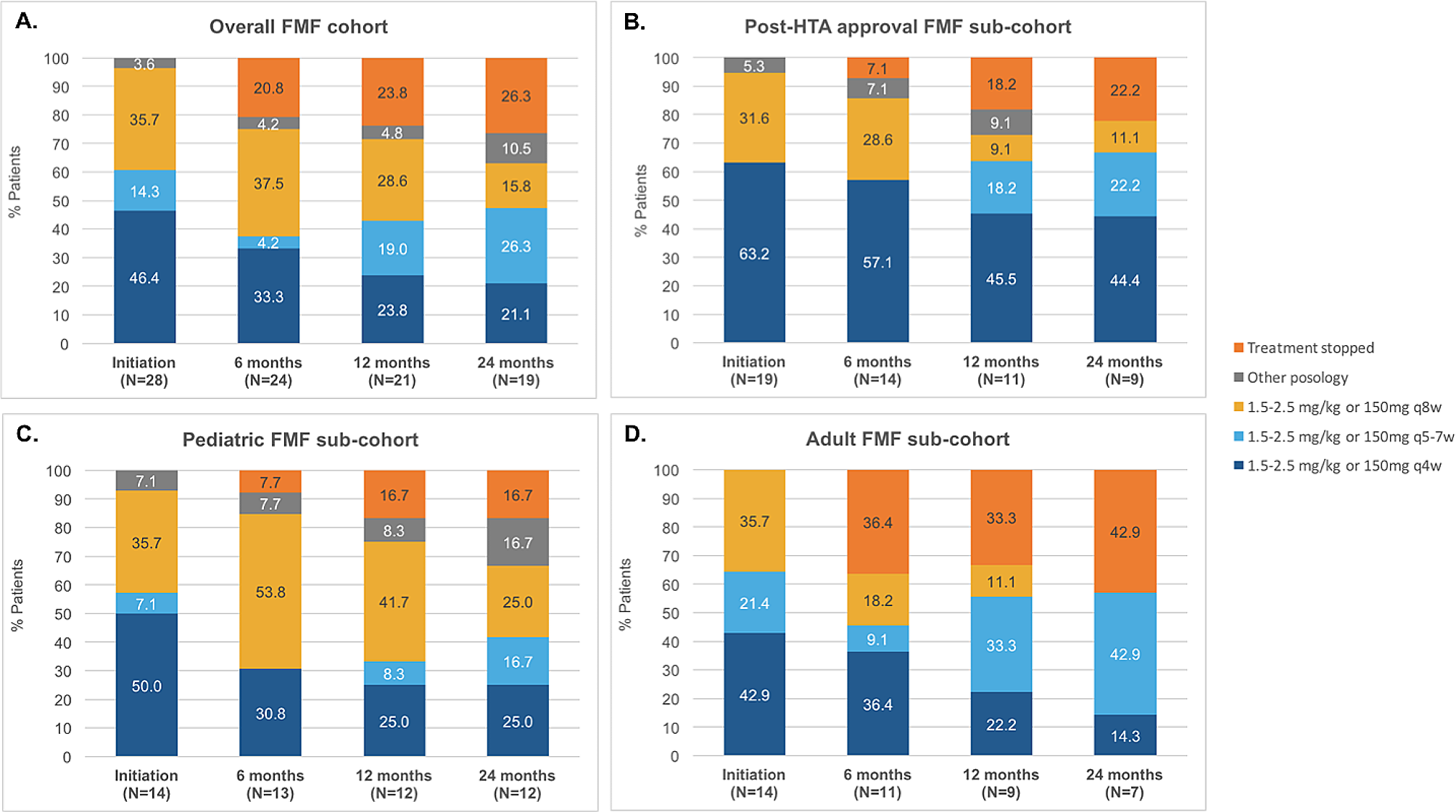
In the pediatric FMF sub-cohort, an increase of the dose intervals was observed at 6 months, 53.8% receiving canakinumab every 8 weeks at this point. It was followed by some adjustment of the dose interval with 25% of the patients having a reduction of the dose interval between 12 and 24 months. At 24 months, 25% were treated with 150 mg or 2 mg/kg every 4 weeks, 16.7% every 5–7 weeks, 25% every 8 weeks, 16.7% had another posology and 16.7% had already stopped canakinumab (including 1 patient due to remission). (Fig. 1)
In the adult FMF sub-cohort, no evolution of the dose intervals was observed in the first 6 months except for one patient who stopped due to remission. The same patient restarted treatment within the next 6 months. At 24 months, among the seven patients with sufficient follow-up, 14.3% received 150 mg or 2 mg/kg every 4 weeks, 42.9% every 5–7 weeks and 42.9% had already stopped canakinumab. (Fig. 1)
In the pediatric and adult MKD sub-cohorts, no specific trends were identified in dose intervals evolution, but a wide range of dose and interval combinations were observed. At 24 months, among the 10 pediatric patients still on treatment, we observed seven different dose and interval combinations, which varied from 300 mg or 4 mg/kg per injection less than 4 weeks apart (highest posology observed) to 150 mg or 2 mg/kg per injection more than 8 weeks apart (lowest posology observed). At 24 months, among the 5 adult patients still on treatment, 4 different doses and interval combinations were observed from 150 mg or 2 mg/kg per injection every 4 weeks (highest posology observed) to 150 mg or 2 mg/kg per injection more than 8 weeks apart (lowest posology observed). (Fig. 2)
In the TRAPS cohort, at 12 months, two patients had canakinumab every 5–7 weeks, two every 8 weeks, one had another posology and one already stopped canakinumab.
Fig. 1
Evolution of canakinumab posology in FMF patients: overall (A), in patients who initiated canakinumab after health authority approval (B), in adult patients (C) and in pediatric patients (D). (FMF: Familial Mediterranean Fever, HTA: Heath technology assessment; q4w: every 4 weeks; q5-7w: every 5 to 7 weeks; q8w: every 8 weeks)
Fig. 2
Evolution of canakinumab posology in MKD patients: overall (A), in patients who initiated canakinumab after health authority approval (B), in adult patients (C) and in pediatric patients (D). (HTA: Heath technology assessment; MKD: Mevalonate Kinase Deficiency; q4w: every 4 weeks; q5-7w: every 5 to 7 weeks; q8w: every 8 weeks)
Evolution of colchicine dosing during canakinumab treatment in crFMF patientsOf the 26 of 31 FMF patients (83.9%) with concomitant colchicine at canakinumab initiation, six patients (23.1%) had a decrease in colchicine dose within the first two years of canakinumab initiation. None of the patients discontinued the colchicine during canakinumab treatment.
Evolution of disease activity with canakinumab treatmentWe had limited information on disease activity and inflammation biomarkers. Six months after canakinumab initiation, of the 12 patients with an AIDAI score (eight FMF and four MKD), 91.7% had a score inferior to nine (i.e. controlled disease). Among the 12 FMF patients and 12 MKD patients with a reported CRP at 6 months, 83.3% and 66.7% respectively had a CRP < 5 mg/l in an attack-free period. Among the 7 FMF and 4 MKD patients with a reported SAA at 6 months, 85.7% and 75.0% respectively had an SAA < 10 mg/l.
SafetySeven FMF patients reported nine AEs (one had three AEs), six MKD patients reported eight AEs (two had two AEs) and one TRAPS patient reported an adverse event. (Table 2). Four FMF patients, one MKD patient, and one TRAPS patient presented a severe AE. Of those, three were suspected to be related to canakinumab (all were infections, one requiring hospitalization or prolongation of hospitalization). Overall, of the 18 AEs reported, nine were infections and four were skin and subcutaneous tissue disorders. Two AEs in FMF, one in MKD, and one in TRAPS led to treatment discontinuation. Three AEs led to a dose reduction. None of the patients died during the study period.
Table 2 Reported adverse events during canakinumab treatment in FMF, MKD and TRAPS patients
留言 (0)