
記住我
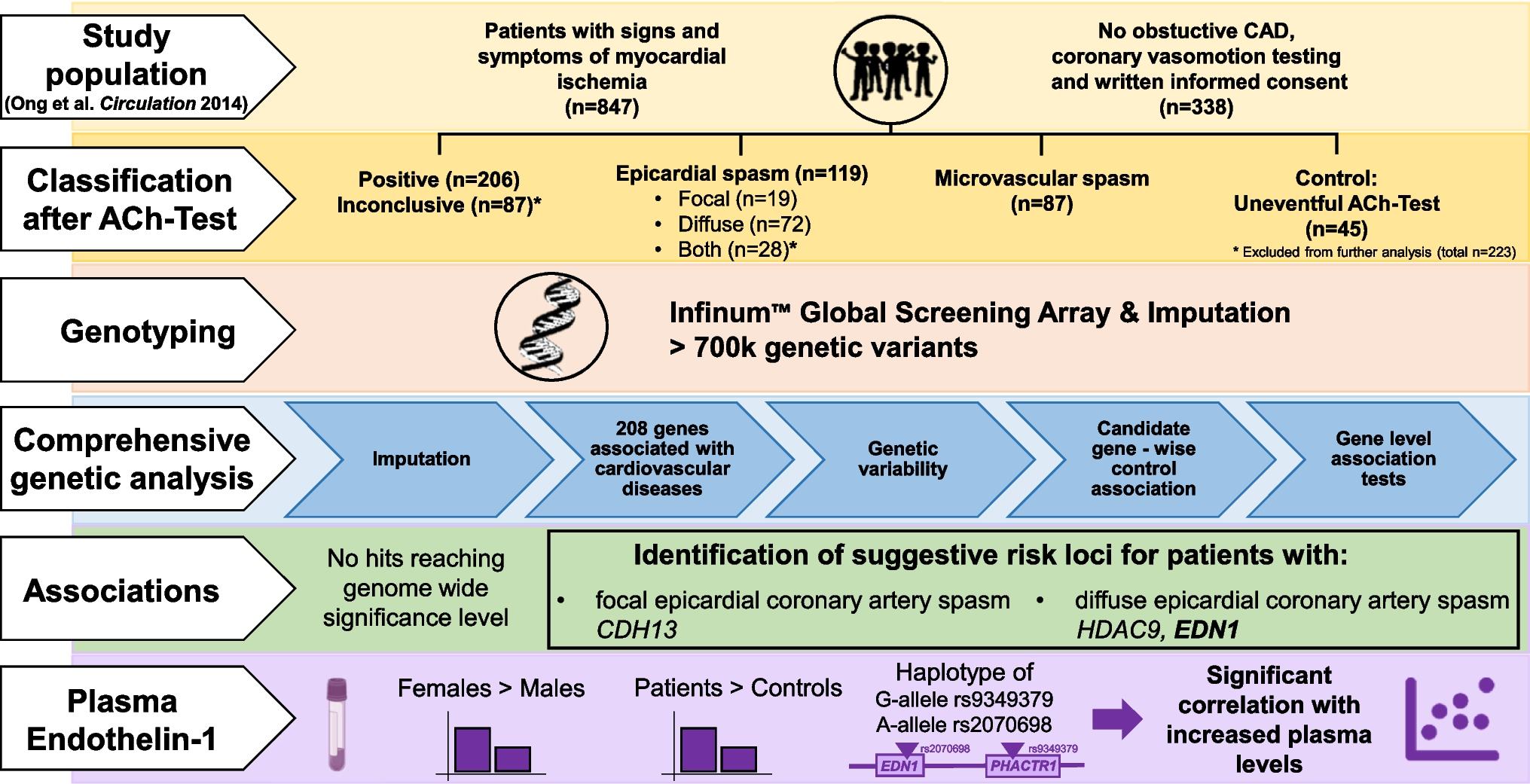
During the study period, a total of 1,051 LuTx patients were evaluated. After exclusion of pediatric patients (12), patients undergoing re-transplantation (27) or multi-organ transplantation (5) and patients with incomplete data or missing follow-up (4), 1,003 patients were included in the analysis (Fig. 1). In total, 98 LuTx patients with relevant CAD could be matched with 98 LuTx patients without CAD, achieving a standard difference of mean below 0.2 for all matching parameters (Supp. Figure 1). The median follow-up was 3.24 [1.30, 4.82] years. In the overall cohort, the median age was 54.7 years [45.8, 60.5] with 547 (54.5%) being male. Restrictive lung disease was the most frequent reason for LuTx (502, 50.0%), followed by obstructive lung disease (289, 28.8%), cystic fibrosis (139, 13.9%), and pulmonary vascular disease (40, 4.0%). The prevalence of CAD including mild CAD and coronary sclerosis was 23%. Relevant CAD was present in 104 (10.4%) patients, with the majority suffering from 1-vessel CAD (64, 6.4%), followed by 2-vessel (23, 2.3%) and 3-vessel disease (17, 1.7%). The most frequently affected coronary artery was the LAD (51, 5.1%), followed by RCA (28, 2.8%), LCX (24, 2.4%) and LM (2, 0.2%). 19 patients (1.9%) had suffered prior MI and revascularization had been performed in 60 patients (6.0%) via PCI while 4 patients (0.4%) had undergone CABG. Detailed baseline characteristics before and after matching can be found in Table 1 and 2, respectively.
Fig. 1
Flow diagram depicting patient selection. 1,051 patients receiving lung transplantation between 01/2000 and 08/2021 were screened, 48 patients met exclusion criteria and were removed from the analysis. A total of 1,003 patients was included and divided in patients with relevant coronary artery disease (n = 104) and patients without relevant coronary artery disease (n = 899). Using 1:1 propensity score matching 98 corresponding pairs of LuTx patients with and without relevant CAD were identified. CAD = coronary artery disease, PCI = Percutaneous coronary intervention, CABG = coronary artery bypass graft
Table 1 Baseline characteristics of unmatched LuTx patients without and with relevant CADTable 2 Baseline characteristics of matched patients without and with relevant CADDifferences in baseline characteristics between patients without and with relevant CADClinical and practical significant differences between unmatched patients with and without relevant CAD were observed concerning age at transplantation [y] (60.3 [56.7, 63.2] vs. 54.0 [44.5, 59.9], p < 0.001), sex [male] (74.0% vs. 52.3%, p < 0.001) and BMI [kg/m2] (24.1 [21.3, 27.4] vs. 22.2 [19.4, 25.6], p < 0.001) as well as the abundance of cardiovascular risk factors including hypertension (67.3% vs. 32.1%, p < 0.001) and history of tobacco use (67.3% vs. 40.9%, p < 0.001). Furthermore, patients with relevant CAD underwent transplants more often for restrictive lung disease (71.2% vs. 47.6%, p < 0.001), had lower CI [L/m2] (2.95 [2.50, 3.40] vs. 3.10 [2.68, 3.70], p = 0.012), more often reduced LVEF (11.6% vs. 5.4%, p = 0.027), a higher rate of carotid plaques (20.2% vs. 8.5%, p < 0.001) and a higher FEV1 [% of reference] (44.00 [23.00, 56.25] vs. 30.00 [20.55, 46.00], p < 0.001) (Tab. 1). In the matched cohort, patients with relevant CAD significantly more often had coronary sclerosis (100% vs. 27.6%, p < 0.001), suffered prior MI (17.3% vs. 0.0%, p < 0.001) and underwent prior PCI (56.1% vs. 0.0%, p < 0.001) (Table 2).
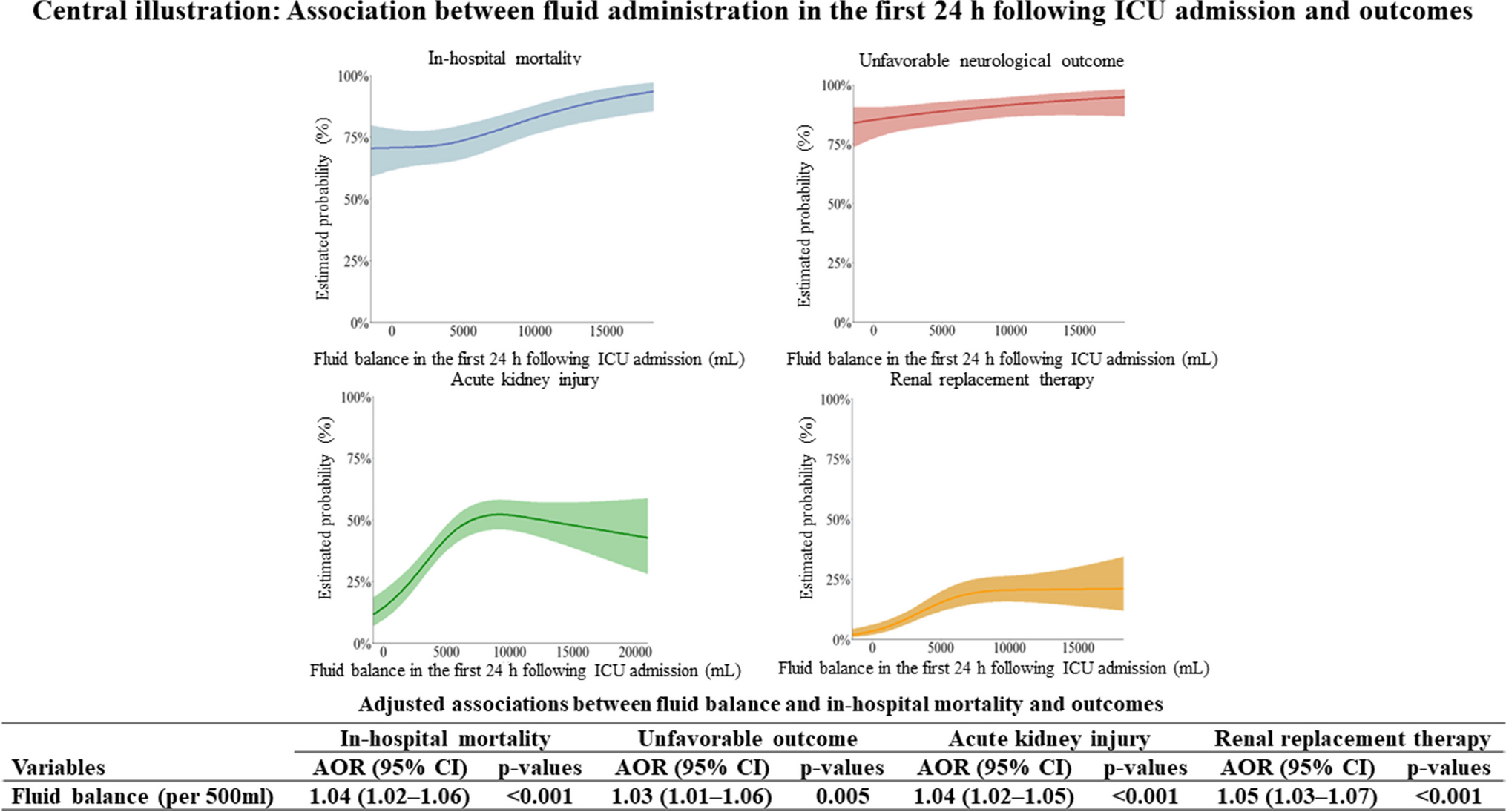
SurvivalSurvival was not significantly different between the two matched groups (HR = 0.90, 95% CI 0.61–1.32, p = 0.800) as shown in Fig. 2 (corresponding Kaplan–Meier analysis for the unmatched cohort (HR = 1.23, 95% CI 0.92–1.64, p = 0.167) is shown in Supp. Figure 2, and for no CAD vs. (I) 1- or 2-vessel disease, vs. (II) 3-vessel disease, vs. (III) prior MI, and vs. (IV) prior revascularization in Supp. Figure 3–6, respectively, accordingly without significant differences in survival). In addition, no significant difference in in-hospital mortality between LuTx patients with and without relevant CAD (8.2% vs. 8.2%, p > 0.999) could be detected (Table 3) (corresponding in-hospital analysis for the unmatched cohort is shown in Supp. Tab. 1–2).
Fig. 2
Kaplan–Meier analysis of propensity score matched lung transplant patients with vs. without relevant coronary artery disease. CAD = coronary artery disease, HR = hazard ration, CI = confidence interval
Table 3 In-hospital mortality in matched patients without and with relevant CADCardiovascular events following LuTxCoronary angiography was required significantly more often in the matched CAD group (17.3% CAD vs. 5.1% non-CAD, p = 0.011). However, MI (7.1% CAD vs. 2.0% non-CAD, p = 0.170), PCI (5.1% vs. 1.0%, p = 0.212) and CABG (1% vs. 0%, p > 0.999) occurred numerically more frequently in the CAD group, but without reaching statistical significance. Stroke (2.0% vs. 6.1%, p = 0.279), atrial fibrillation (new onset) (15.3% vs. 23.5%, p = 0.206), dialysis (8.2% vs. 11.2%, p = 0.630) as well as cardiac arrest (6.1% vs. 11.2%, p = 0.310) were more frequent in the non-CAD group (Table 4, unmatched cohort is shown in Supp. Tab. 3–4) albeit without reaching statistical significance.
Table 4 Adverse events in matched patients without and with relevant CADCause of death following LuTxSepsis and infectious disease were the most common cause of death in LuTx patients (15.3% CAD vs. 16.3% non-CAD, p = 0.832), followed by chronic allograft dysfunction (11.2% vs. 6.1%, p = 0.118). Cardiovascular death occurred more often in the CAD group (7.1% vs. 2.0%, p = 0.078), albeit not reaching statistical significance. Further details on cause of death can be found in Table 5 (unmatched cohort is shown in Supp. Tab. 5–6).
Table 5 Cause of Death in matched patients without and with relevant CADRisk factors for in-hospital mortality in LuTx patientsThe logistic regressions models revealed the following set of independent risk factors for in-hospital mortality: age at transplantation [years] (Odds Ratio [OR] 1.04, 95% confidence interval [CI] [1.01, 1.07], p = 0.009), elevated bilirubin [mg/dl] (OR 1.90, 95%CI [1.19, 3.03], p = 0.007), decreased forced vital capacity [% of reference] (OR 0.97, 95%CI [0.95, 0.99], p = 0.004), double lung transplantation (OR 2.04, 95%CI [1.04, 4.01], p = 0.039) and necessity of reoperation (OR 2.99, 95%CI [1.84, 4.87], p < 0.001) were associated with higher in-hospital mortality. Time since first transplantation [years] (OR 0.93, 95%CI [0.89, 0.97], p = 0.001) was associated with lower in-hospital mortality. However, relevant CAD (OR 1.30, 95%CI [0.55, 3.09], p = 0.547) did not emerge as a risk factor for in-hospital mortality. The results are summarized in Table 6.
Table 6 Risk factors for (A) in-hospital mortality and (B) all-cause mortalityRisk factors for all-cause mortality in LuTx patientsThe following set of risk factors were independently related to all-cause mortality: Age at transplantation [years] (Hazard Ratio [HR] 1.02, 95%CI [1.01, 1.04], p < 0.001), elevated bilirubin [mg/dl] (HR 1.33, 95%CI [1.15, 1.54], p < 0.001), obstructive lung disease (HR 1.43, 95%CI [1.01, 2.02], p = 0.041), decreased forced vital capacity [% of reference] (HR 0.99, 95%CI [0.99, 1.00], p = 0.042) and necessity of reoperation (HR 3.51, 95%CI [2.97, 4.14], p < 0.001) were associated with higher all-cause mortality, while time since first transplantation [years] (HR 0.97, 95%CI [0.95, 0.99], p = 0.001) and double lung transplantation (HR 0.65, 95%CI [0.52, 0.80], p < 0.001) were associated with lower all-cause mortality. Similar to in-hospital mortality, relevant CAD (HR 0.96, 95%CI [0.71, 1.29], p = 0.788) was not associated with all-cause mortality. The results are summarized in Table 6.
留言 (0)