
記住我



In 2021 worldwide, there were still 160 000 new HIV infections among children resulting in a cumulative number of 1.7 million children living with HIV [1]. Identifying children living with HIV remains a challenge. A recent large population-based study in seven countries in eastern and southern Africa estimated that 39% of HIV-infected children aged 0–14 years were undiagnosed [2]. These alarming figures result from the failure of Prevention of Mother-to-Child Transmission of HIV (PMTCT) programs to achieve their overall goal of a mother-to-child transmission of HIV (MTCT) rate of less than 5% in the breastfeeding population or less than 2% in the nonbreastfeeding population and less than 50 HIV infections per 100 000 live births [3]. To date, few countries in sub-Saharan Africa have achieved this goal [1]. This is partly because of the result of the failure to engage all women living with HIV (WLHIV) into care and partly due to new infections among pregnant and breastfeeding mothers after initial negative HIV tests [4,5].
The PMTCT program represents a cascade consisting of health interventions with selected process indicators to track countries’ progress toward elimination of MTCT of HIV: antenatal care (ANC) coverage, HIV testing of pregnant women and antiretroviral therapy (ART) coverage for pregnant women living with HIV [3]. Antenatal visits are the gateway to PTMCT for many women, and the WHO recommends at least four ANC visits during pregnancy [3]. The ANC attendance among pregnant WLHIV is suboptimal in Africa, with only 78.8% of them attending at least four antenatal visits in Gambia in 2013 [6]. A systematic review estimated that the proportion of women attending antenatal care who benefited from HIV counseling was 96% (range 30–100%) [7]. Prenatal HIV testing is highly heterogeneous in sub-Saharan Africa, ranging from 6.1 to 100% [7,8]. WHO estimated that about 80% of pregnant WLHIV were on ART in 2020 [9]. ART coverage among pregnant women has increased over time, and this has been accompanied by a decrease in HIV MTCT [10].
In the postpartum period, the proportion of children with an early infant diagnosis (EID) is still suboptimal in sub-Saharan Africa [11,12] with western and central Africa lagging behind eastern and southern Africa. Furthermore, 25 and 74% of children having their test result transmitted to the mother by 6–8 weeks of life, respectively [1]. In Zambia, only 64% of HIV-exposed children received a postnatal antiretroviral prophylaxis (PNP) [13]. Most PMTCT outcomes are reported to be suboptimal in adolescent girls and young women as compared with their older counterparts [14].
However, most of the data assessing the PMTCT performance are from modelling or small-scale studies.
There is a scarcity of ‘real-world’ and country-level data from the target population as recommended by WHO to complete the modelling data [15]. This makes it difficult to assess efficiently the overall performance of PMTCT programs at the population level.
Most available data are derived from PMTCT program indicators, which by definition do not account for mothers who do not attend PMTCT facilities. In addition, program data are often aggregated (attendance at key visits) rather than individual, making difficult to estimate the proportion of mothers who benefited from different program components.
Across the continent wide, the second immunization visit in the Expanded Program of Immunization (EPI-2) at 6–8 weeks after birth is almost universally attended by children aged 6–8 weeks, regardless of their mothers’ ANC attendance. In the PROMISE-EPI study, we screened all mother–infant dyads at EPI-2. This provided a unique opportunity to retrospectively assess the PMTCT interventions that they had received up to that visit. This population-level assessment strategy has proven effective in Bobo-Dioulasso, a medium-sized urban city of Burkina Faso [16]. The present study aimed to validate this strategy in Burkina Faso and Zambia, two sub-Saharan African countries with different HIV epidemic patterns and different ANC/PMTCT health service organization.
Methods Study designThis cross-sectional study was conducted in Burkina Faso and Zambia. In Burkina Faso, the data collection started in December 2020 and ended in September 2021. In Zambia, it started in December 2019 before the onset of the coronavirus disease 2019 (COVID-19) crisis and ended in July 2021. This analysis is part of the first step in the selection of mother–child dyads for a Phase III randomized controlled trial, the PROMISE-EPI trial (NCT03869944). This study aims to test a rescue preventive intervention among HIV-1-uninfected children exposed to HIV-1 by their HIV-1-infected breastfeeding mothers against a control routine Option B+ implementation. The protocol of the PROMSIE-EPI study has been published elsewhere [17].
SettingsBurkina Faso is a West African country with a HIV prevalence of 0.7% (0.5–0.8%) among adults aged 15–49 years in 2020 [18]. According to UNAIDS, 89% of pregnant women had access to ART, and only 10% of HIV-exposed children had access to early HIV diagnosis in 2020 [18]. During ANC visits at primary healthcare centers (PHC), pregnant women were offered HIV testing through an opt-out process. Those living with HIV are initiated on ART and followed up at the PHC under the supervision of the next level of the healthcare system.
Children born to HIV-infected mothers are initiated on PNP according to WHO recommendations: nevirapine only for 6 weeks for all HIV-exposed children with a dual PNP using zidovudine (AZT) and nevirapine (NVP) for 6 weeks or extended to 12 weeks if children are at high risk of acquisition [19].
EID sampling is scheduled at 6 weeks of age (the 42nd day visit) and the results are returned to caregivers as soon as they are available. PHC are also in charge of the application of the Expanded Program on Immunization (EPI). The EPI-2 visit is scheduled at 8 weeks of child age. This study was implemented in 32 PHC from the two main cities of the country, Ouagadougou and Bobo-Dioulasso.
In Zambia, the HIV prevalence among adults aged 15–49 years was 11.1% in 2020 [18]. Antenatal and postnatal consultations, EPI, HIV care and child health services are all provided in Maternal & Child Health (MCH) clinics until the child reaches 2 years of age. At the time of the study, differences with Burkina Faso in terms of PMTCT program included EID at birth using dried blood spots. The coverage of HIV-exposed children for EID was 64.8% in 2020 [1]. Perinatal infant prophylaxis was systematically initiated at birth with a triple combination of AZT/lamivudine (3TC)-NVP] for 12 weeks [20]. The study was conducted in 4 large MCH clinics (Chilenje, Matero, Bauleni and Chaisa) located in Lusaka. The main background characteristics of the two study settings are summarized in Table 1.
Table 1 - Key background characteristics of Burkina Faso and Zambia. Characteristics Burkina Faso Zambia Location Western Africa Eastern Africa HIV prevalence in the general population 0.7% [0.5–0.8] 11.1% [10.5–11.6] PMTCT-MCH integration Partial Full National recommendation on re-testing among pregnant and postpartum women 3 months 3 months Pregnant women coverage by ART 89% [69–100] 80% [70–89] Early infant diagnosis 10% [8.4–12.8] 64.8% [58.3–74.9] Final MTCT rate 12% [9.2–16.1] 13.% [11.1–16.1]MCH, Maternal & Child Health; PMTCT, Prevention of Mother-to-Child Transmission of HIV.
Postpartum women aged 15 years or older who attended the EPI-2 visit with their child between 4 and 16 weeks of age were included in this study.
Study proceduresAfter informed consent, all mothers attending the EPI-2 visit were offered to participate in the study. Data on PMTCT-related activities were first reviewed on the mother's health card. If answers were unclear or missing, mothers were interviewed by trained health center staff, using a standardized questionnaire for each item, ANC attendance, history of maternal HIV testing and HIV care whenever appropriate, infant antiretroviral prophylaxis, infant sampling for EID and EID result.
HIV testing was then offered to participants except for those known to be living with HIV and those who had a negative test within the previous 3 months in Burkina Faso and within the previous month in Zambia. Data were entered offline at the site into an electronic case report form (eCRF), which was then uploaded daily to the central study database in Burkina Faso. In Zambia, data were entered online.
Subsequently, all eligible WLHIV were offered enrollment in the randomized controlled trial to assess the efficiency of an innovative strategy for the prevention of postnatal transmission.
After informed consent, WLHIV and their children were tested with a point-of-care (POC) device for HIV viral load using the GeneXpert HIV RNA and for HIV DNA using GeneXpert HIV Qual assay, respectively.
The tests were performed on-site at the maternal and child Health unit with same-day results returned to the mothers at the same EPI-2 visit in Zambia. In Burkina Faso, consenting women were referred by a peer navigator to the next level of the healthcare system, the referral Centre Médical avec Antenne Chirurgicale (CMA) for maternal and infant HIV testing. All children found to be living with HIV were enrolled in HIV care and treated with ART at the same facility or at a referral outpatient clinic (OPC), as needed.
Ethical considerationThe PROMISE-EPI study has been approved by the National Ethics Committee of Burkina Faso the ‘Comité d’éthique pour la recherché en santé ‘(CERS) (N° 2020-5-090), the National Ethics committee of Zambia (N° 2018-Oct-002) and the Regional Ethics Committee North (REK nord 2018/1953) in Norway.
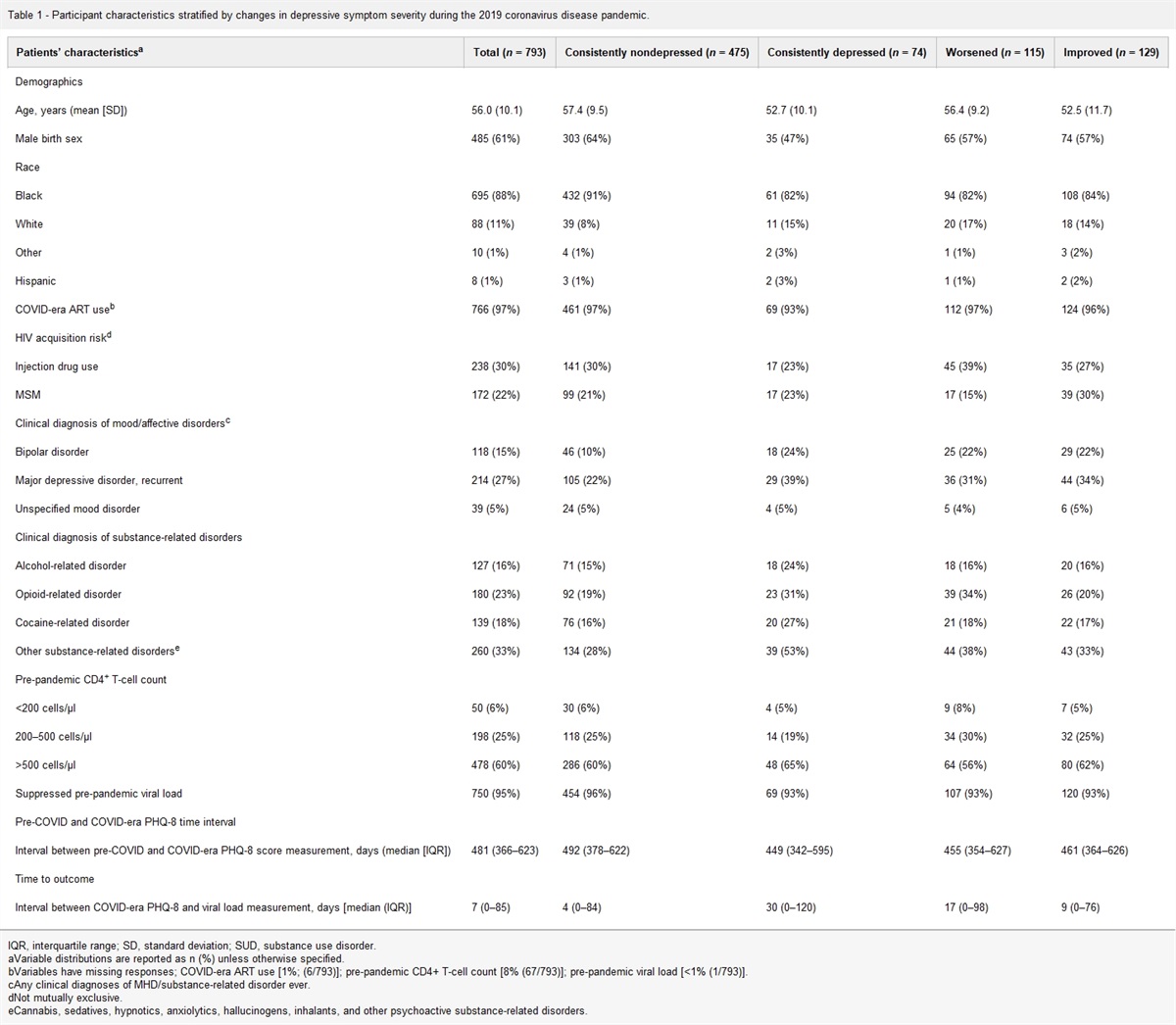
Statistical analysisQuantitative variables are presented as medians with their respective interquartile range (IQR). Qualitative variables are presented as frequencies and their proportions. Differences in proportions were assessed using Pearson's chi-squared test, or Fischer's exact test when conditions were not met. For the Pre-COVID-19 and COVID-19 lockdown analysis, the pre-COVID-19 lockdown period included all visits performed before 1 May 2020 and those performed after 1 May 2020 were considered as during/post COVID-19 period. The association between a detectable maternal viral load (>50 copies/ml) at EPI2 and various sociodemographic characteristics and PMTCT indicators was assessed using multivariate logistic regression. Crude odds ratios (OR) and adjusted odds ratios (aOR) with 95% confidence intervals (95% CI) were calculated.
Variable selection was based on the results of an initial univariate analysis and backward stepwise elimination, both with P less than 0.20 as the threshold. The threshold for statistical significance was set at P less than 0.05. All analyses were performed using Stata 16 (StataCorp LLC, College Station, Texas, USA).
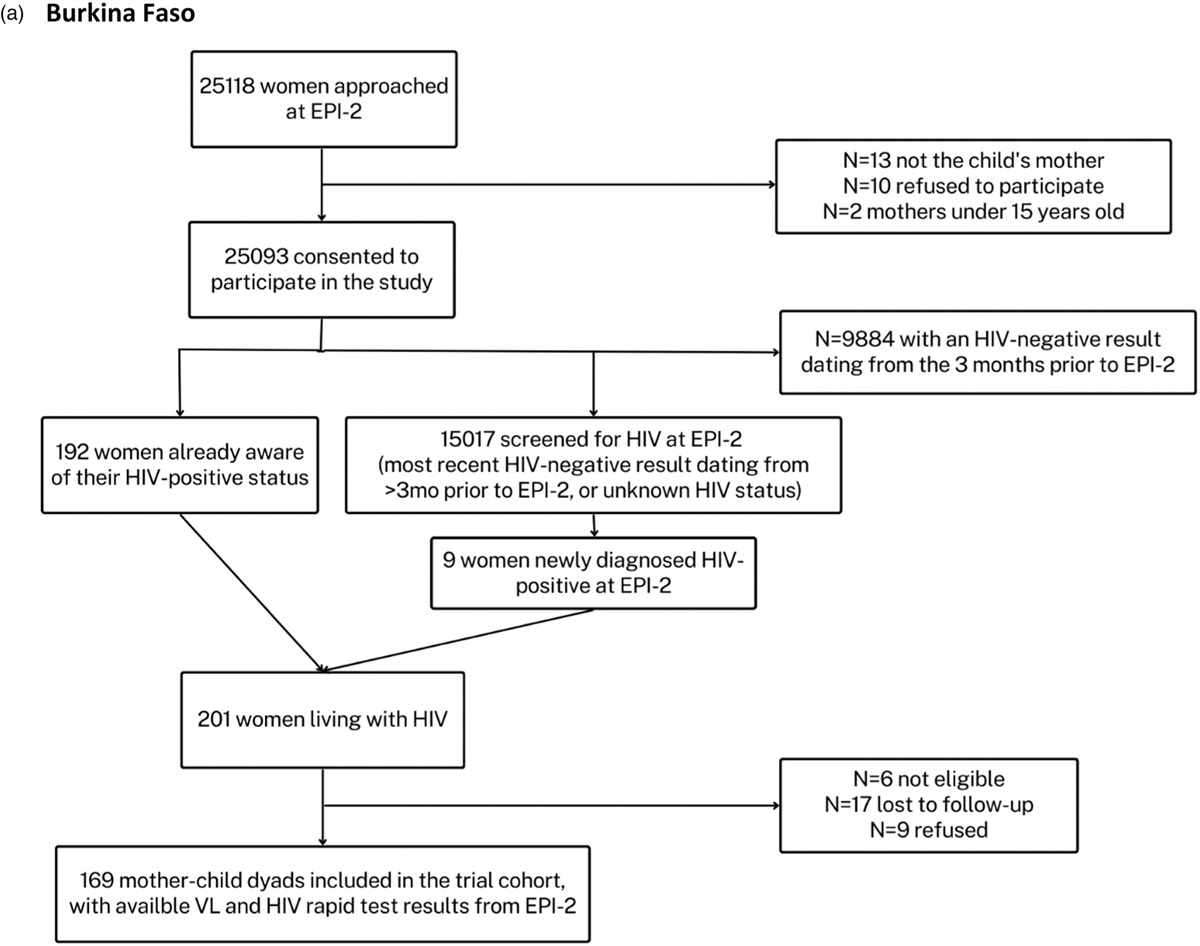
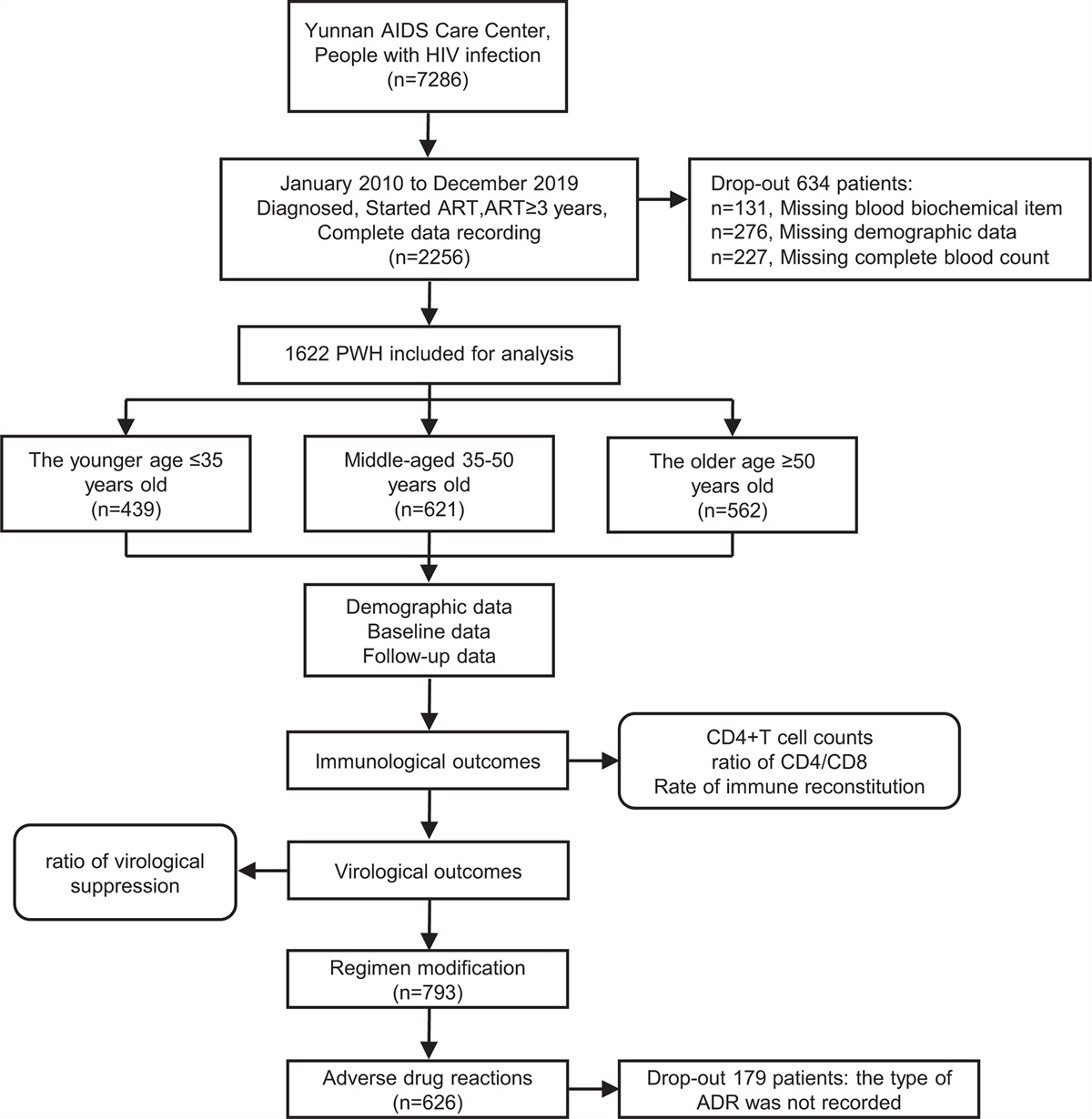
ResultsOverall, 25 118 women were approached for study participation at the EPI-2 visit in Burkina Faso and 25 093 consented to participate (Fig. 1 a). In Zambia, 9920 women were approached for study participation at the EPI-2 visit and 8961 consented to participate (Fig. 1 b).
 Fig. 1:
Fig. 1: Study flow chart.
 Fig. 1 (Continued):
Fig. 1 (Continued): Study flow chart.
Characteristics of the participantsThe median age of the participating mothers was 26 years (IQR: 22–31) in Burkina Faso and 27 years (IQR: 23–32) in Zambia. At enrolment, median child age was 9.1 weeks (IQR: 8.9–9.9) in Burkina Faso and 6 weeks (IQR: 6.0–6.3) in Zambia.
Overall, 99.8 and 99.9% of the women in Burkina Faso and Zambia, respectively, had attended at least one ANC visit. The median number of ANC visits during pregnancy was four visits (IQR: 3–5) in both countries (Table 2).
Table 2 - Characteristics of the participants. Variables Burkina Faso (N = 25 093) Zambia (N = 8961) Maternal age in years, median (IQR) 26 (22–31) 27 (23–32) Infant age in weeks, median (IQR) 9.1 (8.9–9.9) 6 (6–6.3) ANC visits attendancea, median (IQR) 4 (3–5) 4 (3–5) ANC visits attendance 1 361 (1.5%) 205 (2.3%) 2 1721 (6.9%) 685 (7.6%) 3 4902 (19.7%) 1951 (21.8%) 4 8810 (35.3%) 2457 (27.4%) ≥5 9090 (36.5%) 3662 (40.9%) ≥1 25 034 (99.8%) 8960 (99.9%) HIV testing ever done 24 296 (96.8%) 8960 (100%) HIV testing never proposedb 525 (67.7%) 1 (100%) HIV test done during last pregnancy+ 22 939 (99.2%) 7426 (99.1%) HIV test in the last 3 monthsc 9747 (42.5%) 3902 (52.5%)ANC, antenatal care; IQR, interquartile range.
aOne hundred and fifty-four missing values.
bAmong the women never tested for HIV: n = 777, including 776 in Burkina Faso and 1 in Zambia; + among women who declared having been tested for HIV prior to EPI-2 and whose last HIV test result was negative: n = 23 133 in Burkina Faso, and n = 1985 in Zambia.
cAmong women tested for HIV during this last pregnancy (n = 22 939 in Burkina Faso, and n = 7426 in Zambia).
In Burkina Faso, among women who reported having been tested for HIV at any time prior to EPI-2 and whose HIV test result was negative, 22 939 (99.1%) women had been tested for HIV during this last pregnancy. In Zambia, 7426 (99.2%) women had been tested for HIV during their most recent pregnancy. HIV testing had been done during the last 3 months in 42.5 and 52.5% of the women tested during their most recent pregnancy in Burkina Faso and Zambia, respectively. In Burkina Faso and in Zambia, 15 025 (99.1%) and 6898 (97.9%) women, respectively (including those whose last test was done more than 3 months ago and those with unclear information about the last test), were retested during EPI-2 (Table 2).
Prevention of Mother-to-Child Transmission of HIV interventions for women living with HIV and their children up to 6–8 weeks of ageIn Burkina Faso, 201 WLHIV were identified at enrollment in EPI-2, including 9 who were unaware of their HIV status. Among WLHIV who knew their HIV status, 95.8% were on ART at EPI-2, 75 and 62% had viral loads less than 1000 copies/ml and less than 50 copies/ml, respectively (Fig. 2). In Zambia, 1491 WLHIV were identified, including 26 who were unaware of their HIV status. Among WLHIV who were aware of their HIV status, 92.2% were on ART at EPI-2, 79.2 and 72.1% had viral loads less than 1000 copies/ml and less than 50 copies/ml, respectively (Fig. 2).
 Fig. 2:
Fig. 2: Cascade of care for women living with HIV at expanded program on immunization in Burkina Faso and Zambia.
Furthermore, prior to the current pregnancy, 95.8% (184/192) and 99.2% (1454/1465) of WLHIV who knew their HIV status were on ART in Burkina Faso and Zambia, respectively.
In Burkina Faso, among the 31 WLHIV with a viral load more than 1000 copies/ml at the EPI-2 visit, 8 (25.8%) never initiated ART, 15 (48.4%) started ART for the first time during this pregnancy, and 8 (25.8%) were on ART that was initiated before this pregnancy. In Zambia, among the same population (156 WLHIV with a viral load >1000 copies/ml at the EPI-2 visit), the respective proportions were 17 (10.9%), 70 (44.9%) and 69 (44.2%).
All WLHIV with a viral load greater than 1000 copies/ml received adherence support from the study team. They were also strongly encouraged to report the results to their usual HIV care provider for further management according to national guidelines. Infant PNP was administered from birth to 6–8 weeks to 60.9 and 89.7% of HIV-exposed children in Burkina Faso and Zambia, respectively.
In Burkina Faso, only 60 of 192 (31.3%) of HIV-exposed children were tested after delivery. Of these, 3 (5%, or 1.6% of all HIV-exposed children whose mothers knew their HIV-positive status) received a result by EPI-2 (i.e. 2 weeks later) and none were positive.
In Zambia, 64% of the 1465 HIV-exposed children were tested for HIV at birth shortly after birth. Of these, only 145 (15.5%, or 9.9% of all HIV-exposed children whose mothers knew their HIV positive status) received a result by EPI-2 and 1 was positive (Table 3).
Table 3 - Interventions and breastfeeding status of HIV-exposed children whose mothers were aware of their HIV-positive status at EPI-2. HIV-exposed children Burkina Faso (n = 192) Zambia (n = 1465) PNP-initiated 117 (60.9%) 1314 (89.7%) Six weeks PNP completed 93 (48.4%) 1304 (89.0%) Blood collected for EID in routine PMTCT 60 (31.3%) 938 (64.0%) EID result received by EPI-2 3 (1.6%) 145 (9.9%) HIV positive result 0 (0%) 1 (0.7%) Still breastfed at EPI-2a 199 (99.0%) 1410 (94.6%)EID, early infant diagnosis; PNP, postnatal antiretroviral prophylaxis; PMTCT, Prevention of Mother-to-Child Transmission of HIV.
aAmong all positive women (n = 201 in Burkina Faso, and n = 1491 in Zambia).
After testing 1526 HIV-exposed children at EPI-2 as part of the study intervention, 20 were HIV-infected (5 in Burkina Faso and 15 in Zambia) and their status was not known by their mothers. The MTCT rates up to EPI-2 were 3.0% [1.0–6.8] (5/169) in Burkina Faso and 1.1% [0.6–1.8] (15/1357) in Zambia. At EPI-2, the median viral load of mothers of children living with HIV (CLHIV) was 133 500 copies/ml (IQR: 23 550–346 500). All of these mothers had viral loads greater than 50 copies/ml, 18 had viral loads above 1000 copies/ml but 2 of them (10%) had viral loads below 1000 copies/ml (93 and 176 copies/ml).
Factors associated with mother viral load above 50 copies/mlIn a multivariate analysis, attending fewer than four ANC visits [aOR = 1.5; 95% confidence interval (CI) (1.2–2.0)], not having disclosed HIV status to partner [aOR = 2.3; 95% CI (1.6–3.4)], being an adolescent mother (15–19 years) [aOR = 4.7; 95% CI (2.0–10.9)] or being aged between 20 and 24 years [aOR = 1.5; 95% CI (1.0–2.2)] were independently associated with an increased risk of having a viral load above 50 copies/ml at EPI-2, corresponding to the expected viral suppression level under ART. There was a dose–response effect in the link between age and the risk of having a viral load greater than 50 copies/ml (Table 4).
Table 4 - Factors associated with a viral load above 50 copies/ml among the women living with HIV at EPI-2. Variables OR 95% CI aOR 95% CI P value Antenatal care visits ≥ 4 Ref. <4 1.5 1.2–2.0 1.5 1.2–2.0 0.005 Disclosure of HIV status to partner Yes Ref. No 2.3 [1.6–3.4] 2.1 1.5–3.1 <0.001 Age ≥25 Ref. 20–24 1.6 1.2–2.3 1.5 1.0–2.2 0.049 15–19 3.9 1.9–8.0 4.7 2.0–10.9 <0.001The initial model included the following variables: antenatal care visits, mother's age, mother's employment status, use of dolutegravir-based regimen, duration of child's postnatal antiretroviral prophylaxis, country of study, time of mother's HIV diagnosis, mother's level of education and HIV status disclosure to partner. aOR, adjusted odds ratio; CI, confidence interval; OR, crude odds ratio.
Compared with the pre-COVID-19 era (i.e. before May 2021, the reception of EID result at the time of EPI-2 decreased significantly during the COVID-19 crisis, from 36.6 to 9.6% (P < 0.001) (Table 5).
Table 5 - Infant postnatal prophylaxis and early infant diagnosis before and during the coronavirus disease 2019 crisis in Zambia. Pre-COVID-19 perioda (N = 320) During the COVID-19 perioda (N = 1145) P value Infant PNP received since birthb 267 (95.7%) 1047 (98.7%) 0.001 Blood collected for EIDc 202 (63.1%) 736 (64.8%) 0.58 EID results receivedd 74 (36.6%) 71 (7.6%) <0.001COVID-19, coronavirus disease 2019; EID, early infant diagnosis; PNP, postnatal antiretroviral prophylaxis.
aThe pre-COVID-19 period includes the period before 1 May 2020. During the COVID-19, period includes the period starting from 1 May 2021 and onward.
bMissing data: n = 41 in Burkina Faso, n = 84 in Zambia.
cMissing data: n = 9 for the during the COVID 19 period.
dAmong n = 320 infants in the pre-COVID 19 period and n = 1145 during the COVID-19 period.
In these two countries with different healthcare organizations and resources, the performance of their PMTCT programs regarding HIV screening and ART coverage pregnant women met the UNAIDS goals [3]. However, the proportion of WLHIV with successful ART was much lower in Burkina Faso, and both countries had unacceptably low EID coverage rates. Perinatal PNP initiation and completion rates were high in Zambia but too low in Burkina Faso. As a result, Burkina Faso still face a high MTCT rate at EPI-2 visit, and the vast majority of infants diagnosed with HIV were not identified prior to our study, representing a serious missed opportunity for early ART initiation and improved HIV survival.
Our strategy based on the EPI-2 visit could be considered as a complementary approach to usual PMTCT monitoring and evaluation, as a PMTCT impact surveillance tool. In particular, it also complements the population-level evaluation of EID [21]. Although our findings are in full agreement with the proportions of pregnant women on ART in Burkina Faso [100% (100–100%)] and Zambia [97% (81–100)] estimated by UNAIDS [22], the actual EID coverage in our study was much lower confirming previous findings from Bobo-Dioulasso (Burkina Faso), where the EID coverage was as low as 1.8% at EPI-2 visit [16]. Although our evaluation took place, too early after sampling to report the coverage in terms of EID test results. The true MTCT rate at 6 weeks in Zambia (1.1%) is likely to result in a much lower final MTCT rate than the one reported by UNAIDS [7.6%, 95% CI: (6.4–9.5)] [22], given the high proportion of women on suppressive ART. Our findings suggest that these UNAIDS estimates, based on the SPECTRUM model, might be inaccurate and merit revision.
EID remained largely ineffective in both Burkina Faso and Zambia. The main issue is the long turnaround time, usually several months [23,24]. When the test result comes back at MCH or PHC centers, mothers of high-risk infants (those with viral load >1000 copies/ml) are also the ones most likely to stop coming to MCH or PHC.
Again, the current highly centralized approach, relying on very few central laboratories, has obviously been unsatisfactory for many years.
POC machines for maternal viral load testing could also be used for EID [25]. In addition to its cost-effectiveness, this strategy based on POC machines could also be cost-saving for EID [26]. The EID sample collection remained unchanged before and during the COVID-19. In fact, ANC attendance was not affected by the pandemic, and DBS cards remained available during this period. However, the COVID-19 sanitary crisis much hampered the capacity of the laboratories to perform the tests because of reagent shortages and therefore increased the turnaround time (TAT). Of note, even before the COVID-19 period, this TAT was very long as results were available 2 months later for only a third of the children sampled at birth. This indicator is much lower than UNAIDS estimates (64.8%) [1].
Our study showed an impressively high ART coverage among WLHIV, which stands as the main process indicator and target for WHO and PMTCT programs [3]: screening of all pregnant women for HIV and initiation of ART as soon as possible. In this respect, both Burkina Faso and Zambia are meeting the expectations. However, having meet this milestone, we must now focus more attention and efforts on improving ART success rates. Using a high threshold for ART efficacy of 1000 copies/ml, the suboptimal proportions of women with successful treatment (75% in Burkina Faso and 79.2% in Zambia) leave too many infants at risk of HIV acquisition, both intrapartum and during breastfeeding. Rapid transmission of HIV viral load results is a key step in improving these figures. Both alternative viral load techniques using POC machines, and a centralized approach to laboratory activities coupled with improved sample referral and electronic transmission of results, are potential solutions. In addition, during women's lifelong HIV care, viral load monitoring using cost-effective POC machines should be prioritized pregnancy and breastfeeding. Our results suggest that targeting young women and those who attended only one ANC visit during pregnancy, that is, those at much higher risk of ART failure, may be the first priority.
Indeed, in our study, adolescent and young mothers are at increased risk of not achieving an undetectable viral load, not attending multiple ANC visits, and missing HIV screening of their child (data not shown). Other studies have highlighted that these mothers are also at higher risk of poor ART adherence and poor retention in PMTCT programs [27,28].
Interventions aiming at improving adherence throughout the PMTCT cascade are needed to further reduce the risk of MTCT. These may include strengthening retention in care and adherence support [29,30]. Long-acting ART [31] if found well tolerated and effective in pregnant and postpartum women may also improve adherence. Targeting adolescent mothers, that is, those at much higher risk of ART failure, may be the first priority. Further studies are needed to document the facilitators and barriers to care for these young women, and how they could be prevented and addressed. Long-acting PNP [32] could also contribute to improve infants’ suboptimal PNP completion.
Our study demonstrates the feasibility of POC EID, with same-visit results at immunization visit, in two different countries with two different healthcare settings. It confirms the reliability of this entry point for EID A local, district-level organization, based on one or two POC machines in the largest centers, may be envisioned. Urgent action is needed to fill this under-recognized gap in PMTCT. Keeping in mind that later child HIV diagnosis, after 6 months or more of breastfeeding, also has poor coverage [33,34], few CLHIV benefit from a chance to be initiated on ART early, and many will remain undiagnosed [2] until they reach the end-stage of the disease.
Our study has limitations. It did not include rural areas where maternal characteristics are likely to be different in terms of education level, access to health facilities, or health literacy, which could lead to different PMTCT outcomes. Therefore, our findings, although based on more than 30 000 women, do not reflect the national situation in any of the countries.
In conclusion, our study validates the feasibility and reliability of evaluating PMTCT programs through the EP-2 visit in both low HIV prevalence (Burkina Faso) and high HIV prevalence (Zambia) settings. Although our findings confirmed very high maternal HIV testing and ART coverage, they highlighted sub-optimal perinatal PNP coverage, very low EID coverage and sub-optimal proportion of MLHIV on successful ART, particularly in Burkina Faso.
This PMTCT evaluation strategy within the EPI-2 visits with a short questionnaire could strengthen program monitoring by providing real-world (not modeled) data to help identify programmatic gaps that could be targeted for specific actions and resources on the road to pediatric HIV elimination.
AcknowledgementsWe want to thank all the study participants and the PROMISE-EPI Trial Group.
PROMISE-EPI Trial Group:
PCCEI/University of Montpellier (France): Philippe Van de Perre (principal investigator); Nicolas Nagot (methodologist); Jean-Pierre Moles (international laboratory coordinator); Anaïs Mennecier (international project manager); Beatriz Mosqueira (international project manager); Morgana d’Ottavi (central data-manager and biostatistician). University Teaching Hospital (Zambia): Chipepo Kankasa (principal investigator); Mwiya Mwiya (project coordinator); Catherine Chunda-Liyoka (assistant coordinator); Maria Melany Winfried Tonga (medical officer); David Rutagwera (laboratory coordinator); Beauty Matoka (monitor). Centre Muraz (Burkina Faso): Paulin Fao (principal investigator); Leticia Sakana (project manager Bobo-Dioulasso and monitor); Souleymane Tassembedo (project manager Ouagadougou and monitor); Dramane Kania (laboratory coordinator); Ajani Ousmane Taofiki (monitor Bobo-Dioulasso); Tegawende Dimanche Felix Sabo (Monitor Ouagadougou); Edgard Franck Kadeba (assistant laboratory coordinator Bobo-Dioulasso); Ibrahima Diallo (data manager Bobo-Dioulasso); Ousseni Bandaogo (assistant laboratory coordinator Ouagadougou); Nathalie de Rekeneire (scientific advisor). CMA de Do (Burkina Faso): Amélie Nikiema (Clinician) Moussa Sinare (laboratory assistant), Sabrina Eymard-Duvernay (central datamanager and biostatistician).
CMA de Dafra (Burkina Faso): Emmanuel Coulibaly (Clinician), Seydou Otore (laboratory assistant).
CMA de Pissy (Burkina Faso): Diallo-Barry Fatimata (Clinician), Cyrille Ouedraogo (laboratory assistant).
CMU Gounghin 6 (Burkina Faso): Abdallah Ouedraogo (Clinician), Fati Ouedraogo (Laboratory assistant). Université de Ouagadougou: Nicolas Meda (methodologist)
University of Bergen (Norway): Thorkild Tylleskar (child health expert); Ingunn Engebretsen (child nutrition expert). ANRS I MIE (France): Claire Rekacewicz (head of international research and collaboration department); Isabelle Fournier (senior project manager); Laura Fernandez (project manager). University of Toronto (Canada): Renaud Boulanger (ethical advisor).
The Scientific Advisory Board: Nigel Rollins (WHO, Switzerland), Roger L. Shapiro (School of Public Health, Harvard University, USA), Makoura Traore-Barro (CHUSS, Burkina Faso), Adama Dembele (CHUSS, Burkina Faso), Issiaka Sombie (OOAS, Burkina Faso), Kozwa Zyambo (Ministry of Health, Zambia) and the Data Safety Monitoring Board: Melissa Neuman (London School of Hygiene and Tropical Medicine, UK), Valeriane Leroy (Toulouse III University, France), Albert Faye (APHP, France), Thomas Bourlet (CHU St Etienne, France), Ameena Goga (SA-MRC, South Africa) and Connie Osborne (Kwame Nkrumah University, Zambia).
Ethics approval: Granted by the National Ethics Committee of Burkina Faso the ‘Comité d’éthique pour la recherché en santé ‘(CERS) (N° 2020–5-090), the National Ethics committee of Zambia (N° 2018-Oct-002) and the Regional Ethics Committee North (REK nord 2018/1953) in Norway.
Consent to participate: all participants provided written informed consent.
Consent for publication: no consent from the sponsor or any required bodies was needed.
Availability of data: deidentified data will be made available upon request to the corresponding author.
Code availability: the code is available upon request to the corresponding author.
Authors’ contributions: P.V.D.P., N.N., T.T., F.P., L.D.S., D.K., J.P.M. designed the study. S.T., L.D.S., A.M., M.D. and A.O.T. were responsible for data collection and oversaw the study implementation. M.D. and S.T. conducted the statistical analyses, under the supervision of N.N., P.V.D.P. and J.P.M. S.T. drafted the manuscript. All authors critically reviewed the manuscript and approved the manuscript for submission.
Funding: European and Developing Countries Clinical Trial Partnership (EDCTP).
Conflicts of interestThere are no conflicts of interest.
References 1. UNAIDS. UNAIDS data 2021 [Internet] [cited 3 November 2022]. Available at: https://www.unaids.org/en/resources/documents/2021/2021_unaids_data. [Accessed 3 November 2022] 2. Teasdale CA, Zimba R, Abrams EJ, Sachathep K, Ndagije F, Nuwagaba-Biribonwoha H, et al. Estimates of the prevalence of undiagnosed HIV among children living with HIV in Eswatini, Lesotho, Malawi, Namibia, Tanzania, Zambia, and Zimbabwe from 2015 to 2017: an analysis of data from the cross-sectional Population-based HIV Impact Assessment surveys. Lancet HIV 2022; 9:e91–e101. 3. World Health Organization. Global guidance on criteria and processes for validation: elimination of mother-to-child transmission of HIV and syphilis [Internet]. World Health Organization; 2014 [cited 16 January 2023]. 22 pp. Available at: https://apps.who.int/iris/handle/10665/112858. [Accessed 16 January 2023] 4. Graybill LA, Kasaro M, Freeborn K, Walker JS, Poole C, Powers KA, et al. Incident HIV among pregnant and breast-feeding women in sub-Saharan Africa: a systematic review and meta-analysis. AIDS 2020; 34:761–776. 5. Thomson KA, Hughes J, Baeten JM, John-Stewart G, Celum C, Cohen CR, et al. Partners in Prevention HSV/HIV Transmission Study and Partners PrEP Study Teams. Increased risk of HIV acquisition among women throughout pregnancy and during the postpartum period: a prospective per-coital-act analysis among women with HIV-infected partners. J Infect Dis 2018; 218:16–25. 6. Yaya S, Oladimeji O, Oladimeji KE, Bishwajit G. Prenatal care and uptake of HIV testing among pregnant women in Gambia: a cross-sectional study. BMC Public Health 2020; 20:485. 7. Car LT, Brusamento S, Elmoniry H, van Velthoven MH, Pape UJ, Welch V, et al. The uptake of integrated perinatal prevention of mother-to-child HIV transmission programs in low- and middle-income countries: a systematic review. PLoS One 2013; 8:e56550. 8. Awopegba OE, Kalu A, Ahinkorah BO, Seidu AA, Ajayi AI. Prenatal care coverage and correlates of HIV testing in sub-Saharan Africa: insight from demographic and health surveys of 16 countries. PLoS One 2020; 15:e0242001. 9. UNAIDS. Full report — In Danger: UNAIDS Global AIDS Update 2022 [Internet]. 2022 [cited 13 February 2023]. Available at: https://www.unaids.org/en/resources/documents/2022/in-danger-global-aids-update. [Accessed 13 February 2023] 10. Astawesegn FH, Stulz V, Conroy E, Mannan H. Trends and effects of antiretroviral therapy coverage during pregnancy on mother-to-child transmission of HIV in sub-Saharan Africa. Evidence from panel data analysis. BMC Infect Dis 2022; 22:134. 11. Anaba UC, Sam-A
留言 (0)