
記住我



The incidence of HIV among the older population is increasing because of widespread transmission and the use of highly effective antiretroviral therapy (ART). Consequently, a progressive shift in the age structure towards the older has been observed among those people with HIV (PWH) [1]. Approximately 8.1 million people aged 50 years or older are currently living with HIV worldwide, a number that is expected to increase [2]. Notably, China has experienced a pronounced escalation in the annual growth rate of HIV cases within its older population. The incidence of new HIV diagnoses for those aged 60 years and older has increased from 1.35 to 14.06 per 100 000 between 2007 and 2018, with a particularly marked increase in males aged 60–79 years and females aged 50–69 years [3]. Recent studies conducted by the Chinese Center for Disease Control and Prevention have also shown a substantial increase in the proportion of PWH aged 50 years and older in China, rising from 22% in 2011 to 44% in 2020 [4]. These findings highlight the increasing number of older PWH in China and emphasize the urgent need for further research focused on addressing the unique challenges and healthcare needs of this vulnerable population.
The aging process, coupled with the HIV infection and various health concerns such as liver and kidney deterioration, non-AIDS-related illnesses, geriatric syndromes, and heightened emotional and physical stress, can have a substantial impact on older PWH [5–7], resulting in more complex and challenging clinical management. The primary intervention for HIV is ART; however, no specific ART regimen has yet been established for older populations. The response of older PWH to ART remains a subject of controversy, despite numerous studies demonstrating potential benefits for this population. Some studies suggest that older participants have better virological outcomes compared with younger people, but their immune function recovery tends to be more slower [8–11]. Conversely, other studies have reported no significant age-related differences in immune recovery or viral suppression over time [12–15]. It is worth noting that studies on immunological and virological responses to ART have predominantly concentrated on younger participants, typically excluding older participants because of the potential complexities associated with age-related comorbidities. Furthermore, there is a lack of research on the long-term effects of immune reconstitution in older individuals after ART. Considering the significance of age-related differences in ART outcomes, it is essential to thoroughly investigate the response to ART in older populations.
The establishment of Yunnan antiviral therapy management information system has facilitated the analysis of ART effectiveness in specific populations over time. To gain a better understanding of ART outcomes in older participants, we systematically analyzed immune reconstitution characteristics, virological suppression, regimen changes and adverse drug reactions (ADRs) in older PWH, with the aim of enhancing and personalizing treatment strategies to meet the specific needs of older PWH.
Materials and methods Study designThe study cohort was drawn from the Yunnan Provincial AIDS Care Centre in Kunming, China, which had provided comprehensive follow-up care for over 7200 PWH. Participants diagnosed as HIV-positive and initiated ART between January 2010 and December 2019 were included. The inclusion criteria were as follows: be at least 18 years old, have received ART for a period exceeding 36 months, and had complete records for no less than three follow-up visits. Participants with incomplete demographic, baseline, or follow-up data were excluded.
Participants were monitored for a minimum of 3 years. Each participant underwent routine clinical assessments and laboratory tests, typically at intervals of 3–6 months after treatment commencement, and subsequently every 6–12 months. The follow-up time was calculated from the date of ART initiation to the most recent follow-up. Upon starting ART, clinicians prescribed a tailored medication schedule for each PWH, considering their overall health status and existing HIV management guidelines. A standard ART regimen typically combines two nucleoside reverse transcriptase inhibitors (NRTIs), with a nonnucleoside reverse transcriptase inhibitor (NNRTI), a protease inhibitor, or an integrase strand transfer inhibitor (INSTI).
Data collectionThe data were obtained from the National AIDS Integrated Prevention and Control Information System, including demographic details (age, gender, date of diagnosis, route of HIV infection, and marital status), immunological outcomes (CD4+, CD8+ T-cell counts, and CD4+/CD8+ ratio), virological outcomes (viral load), and treatment outcomes (regimen changes and ADRs).
Laboratory measurementsThe counts of CD4+ and CD8+ T-cell counts were assessed using Truecount Tubes (BD Biosciences, San Jose, CA, USA) and a FACSCalibur flow cytometer (BD Biosciences). The viral load was determined with the Viral Load Detector (Roche, Basel, Switzerland) and its associated reagent (COBAS TaqMan HIV-1 Test v2.0).
Hepatitis C virus (HCV) infection was detected by the HCV Antibody Diagnostic Kit (Wantai BioPharm, Beijing, China). Virus RNA extraction was conducted with a Stream SP96 automated nucleic acid extractor (Daan Gene, Guangdong, China), and RNA amplification was performed on an Applied Biosystems 7500 system (Applied Biosystems, Warrington, UK) with the HCV Nucleic Acid Detection Kit (Daan Gene). HCV infection was determined based on positive results for anti-HCV and HCV RNA. Hepatitis B virus (HBV) infection was defined as the positive of HBV surface antigen (HBsAg) using an ELISA kit (Wantai BioPharm). The experimental procedure was conducted following the manufacturer's instructions.
Outcomes of interestThe study participants were categorized into three groups based on their age at ART initiation: younger (18–34 years), middle-aged (35–49 years), and older (50 years and above). Immunological outcomes were assessed using CD4+ T-cell counts, CD4+/CD8+ ratio, and cumulative complete immune reconstitution (CIR) at different time intervals. CIR was defined using binary indicators (CD4+ T ≥ 500 cells/μl and CD4+/CD8+ ratio ≥0.8) [16], which have been validated as accurate measures of immune system function and status and can predict the likelihood of death after long-term ART [17]. Virological outcomes were assessed according to the Chinese Guidelines for Diagnosis and Treatment of Human Immunodeficiency Virus Infection/Acquired Immunodeficiency Syndrome (2021 edition), with a single viral load at least 200 copies/ml or a rebound to at least 200 copies/ml after initial suppression classified as ‘virological failure’ [18]. Furthermore, regimen changes and the emergence of ADRs were also examined. Regimen changes was defined as any alteration, switch, or discontinuation of at least one antiretroviral drug from the initial ART regimen [19].
Statistical methodsStatistical analyses were performed using SPSS V.21 (SPSS, Chicago, Illinois, USA) and data were visualized using GraphPad Prism V.9.4.1 (GraphPad Prism, San Diego, CA, USA). Missing data were omitted from the analyses. Values were presented median and interquartile range (IQR) for data that were not normally distributed, and number (%) for categorical variables. The incidence of regimen changes and ADRs was calculated by total person-years (PYs) and reported as the number per 100 PYs. For multigroup comparison, P values were derived from the Kruskal–Wallis test or the chi-squared test or Fisher's exact test. Multivariate survival analyses were performed using the Cox proportional hazards model. In Cox regression analysis, statistically significant variables in univariate Cox regression were further enrolled into multivariate Cox regression. For all comparisons, P less than 0.05 was considered statistically significant.
Ethical considerationsWritten informed consent was obtained from all study participants. The research was conducted in accordance with the Declaration of Helsinki and was approved by the Ethics Committee of the Yunnan Infectious Diseases Hospital (approval number: 2022004).
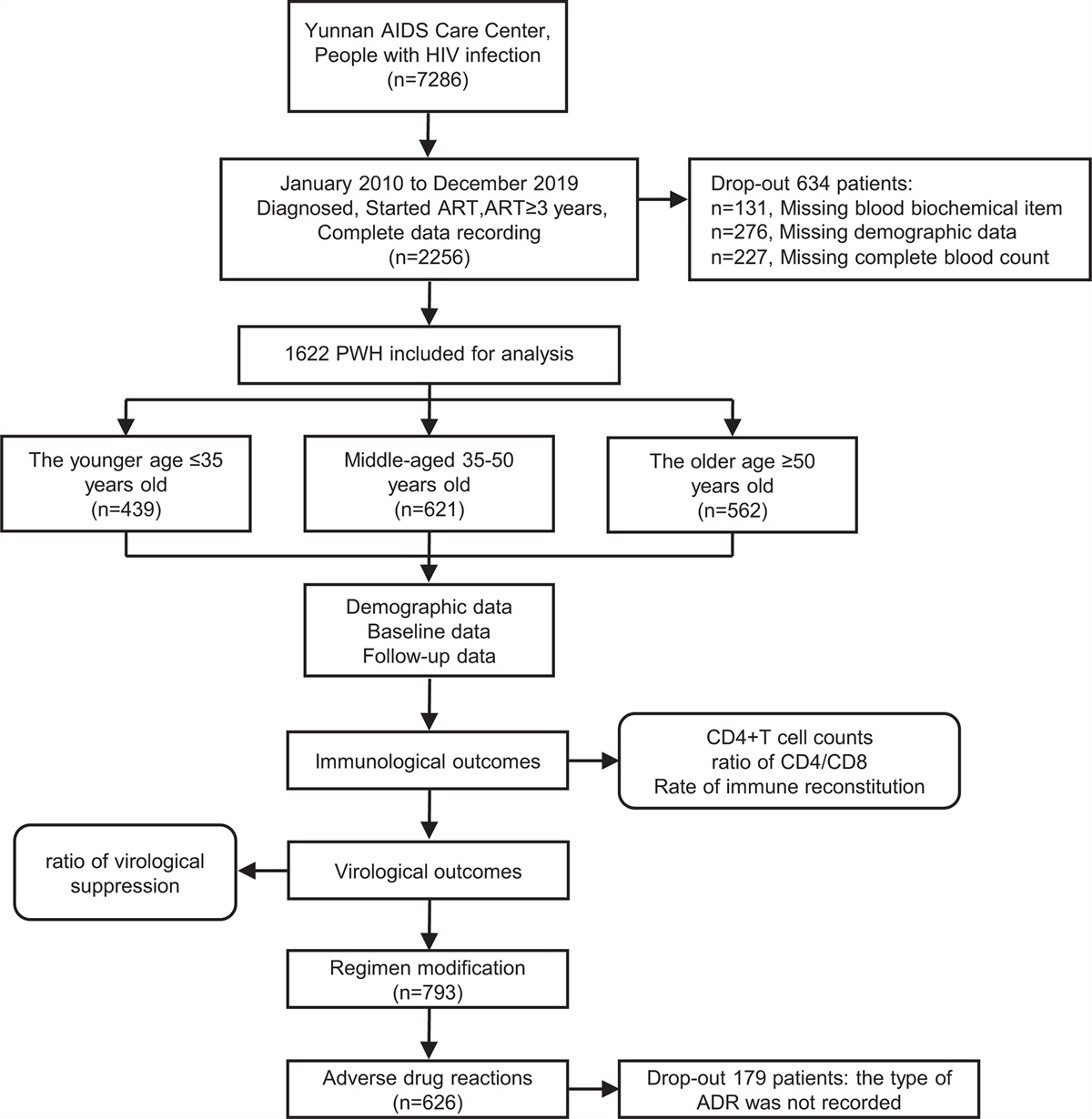
Results Cohort characteristics at enrollmentThe study included 439 younger, 621 middle-aged, and 562 older participants (Fig. 1 and Table 1). The median ages of ART initiation were 21.40 (IQR 20.00–23.00), 45.20 (IQR 43.00–48.00), and 58.50 (IQR 54.00–62.00) years in the younger, middle-aged, and older groups, respectively. The study population comprised 68.4% male individuals, with the younger group having the highest proportion of 81.3%, compared with 61.5% in the middle-aged and 65.8% in the older group. Sexual contact was the most common risk behavior for HIV infection. Younger individuals reported more homosexual contact (59.9%, n = 263), whereas heterosexual contact was more common among middle-aged (65.9%, n = 409) and older individuals (77.9%, n = 438). Intravenous drug use (IDU) (15.5%, n = 96) was the second most important risk factor for middle-aged participants, whereas a larger proportion of older participants (16.2%, n = 91) had unknown risk behaviors. The middle-aged participants had the longest follow-up duration with a median of 9.00 years (IQR 7.10–10.00) and the longest time to start ART after HIV diagnosis (0.90 months, IQR 0.40–3.30). Additionally, the rate of anti-HCV was significantly higher in the middle-aged group (12.6%, n = 78) compared with the younger (0.2%, n = 1) and older groups (2.8%, n = 2), but no significant difference was observed in the rate of HBV infection.
 Fig. 1:
Fig. 1: Patient flow diagram and study design.
Table 1 - Demographic and clinical baseline characteristics of study participants. Characteristics Younger (18–34 years) (n = 439) Middle-aged (35–49 years) (n =621) Older (≥50 years) (n = 562) P value Age at initial ART 21.40 (20.00–23.00) 45.20 (43.00–48.00) 58.50 (54.00–62.00) <0.001 Gender Male 357 (81.3) 382 (61.5) 370 (65.8) <0.001 Female 82 (18.7) 239 (38.5) 192 (34.2) Follow-up year 6.30 (4.60–8.00) 9.00 (7.10–10.00) 7.40 (5.30–9.30) <0.001 Diagnosis treatment interval 0.80 (0.30–2.20) 0.90 (0.40–3.30) 0.70 (0.30–1.60) 0.001 Marital status Married 44 (10.0) 465 (74.9) 450 (80.1) <0.001 Unmarried 376 (85.6) 53 (8.5) 22 (3.9) Divorced or widowed 3 (0.7) 95 (15.3) 81 (14.4) Unclear 16 (3.6) 8 (1.3) 9 (1.6) Infection route Heterosexual 119 (27.1) 409 (65.9) 438 (77.9) <0.001 Homosexual 263 (59.9) 31 (5.0) 15 (2.7) Blood transfusion 3 (0.7) 4 (0.6) 1 (0.2) Intravenous drug use 1 (0.2) 96 (15.5) 17 (3.0) Mother to child 14 (3.2) 0 (0.0) 0 (0.0) Other/unclear 39 (8.9) 81 (13.0) 91 (16.2) Baseline HBsAg Positive 19 (4.3) 35 (5.6) 21 (3.7) 0.157 Negative 329 (74.9) 431 (69.4) 421 (74.9) Unclear 91 (20.7) 155 (25.0) 120 (21.4) Baseline anti-HCV Positive 1 (0.2) 78 (12.6) 16 (2.8) <0.001 Negative 347 (79.0) 385 (62.0) 423 (75.3) Unclear 91 (20.7) 158 (25.4) 123 (21.9) Baseline CD4+ (cells/μl) 452 (292–632) 272 (162–418) 285 (179–427) <0.001 Baseline CD4+/CD8+ 0.45 (0.28–0.63) 0.31 (0.18–0.48) 0.30 (0.18–0.48) <0.001Figures are n (%) or median (IQR). Anti-HCV, antibodies against the hepatitis C virus; ART, antiretroviral therapy; HBsAg, hepatitis B surface antigen; IQR, interquartile range.
Changes in CD4+ T-cell counts and CD4+/CD8+ ratio during the follow-up were illustrated in Fig. 2. Younger participants had the highest baseline CD4+ T-cell counts, measured at 452 cells/μl (IQR 292–632), middle-aged and older participants had significantly lower counts of 272 (IQR 162–418) and 285 (IQR 179–427) cells/μl, respectively (P < 0.05). The CD4+ T-cell count remained consistently higher in younger participants compared with middle-aged and older participants (P< 0.01) after ART. Notably, younger participants had the highest CD4+ T-cell counts of 720 cells/μl (IQR 522–834) at 8 years post-ART. In comparison, the middle-aged and older groups reached their peak CD4+ T-cell counts at 575 cells/μl (IQR 438–749) and 498 cells/μl (IQR 357–700), respectively (Fig. 2a). To adjust for differences in baseline CD4+ T-cell counts, relative CD4+ T-cell counts were calculated, that is, the number of CD4+ T cells that increased after ART relative to baseline. Results showed that relative CD4+ T-cell counts increased rapidly during the first 4 years. The younger group had the highest relative CD4+ T-cell counts of 419 cells/μl (IQR 236–573), whereas the middle-aged and older groups reached 421 (IQR 293–572) and 323 (IQR 191–464) cells/μl, respectively (Fig. 2b).
 Fig. 2:
Fig. 2: Differences in virological and immunological dynamics among different age groups.
The baseline CD4+/CD8+ ratios in the younger, middle-aged, and older groups were 0.45 (IQR 0.28–0.63), 0.31 (IQR 0.18–0.48), and 0.30 (IQR 0.18–0.48), respectively. These ratios increased to 0.75 (IQR 0.54–1.01), 0.67 (IQR 0.51–0.95), and 0.58 (IQR 0.40–0.87) at the end of follow-up (Fig. 2c). During the follow-up period, both the middle-aged and older groups had lower CD4+/CD8+ ratios compared with the young group (P < 0.05). However, compared with the older group, the middle-aged group had a higher relative CD4+/CD8+ ratio at years 3 and 9 after ART and attained a higher CD4+/CD8+ ratio at the end of follow-up (P< 0.05) (Fig. 2d). Based on these findings, older participants appeared to experience a lower level of CD4+ T-cell recovery and relative CD4+ T-cell growth after ART compared with younger participants, suggesting that age may have a negative impact on these factors.
Older participants show a higher risk of poor immune reconstitutionA total of 119 participants (7.34%) demonstrated CIR before ART. There were no significant variations observed in the distribution of this population among the three age groups: younger (7.97%), middle-aged (7.73%), and older (6.41%) individuals (P = 0.572). The rate of CIR increased after ART. As shown in Fig. 2e, younger participants achieved a higher proportion of CIR compared with middle-aged and older participants (P < 0.001). At the end of the follow-up, 52.16% of young participants achieved CIR, compared with 39.29% of middle-aged and 32.21% of older participants (P < 0.001).
Cox regression analysis was conducted to examine the factors influencing CIR following ART. Age at ART initiation, marital status, infection route, initial ART regimen, regimen changes, baseline CD4+, CD8+ T-cell counts, and the CD4+/CD8+ ratio independently influenced CIR in the univariate Cox regression analyses (P < 0.05). In the multivariate Cox model, age over 50 at ART initiation, unmarried status, homosexual transmission, baseline regimen containing INSTIs, and baseline CD8+ T-cell counts at least 1000 cells/μl were identified as independent risk factors for incomplete immune reconstitution (Table S2, https://links.lww.com/QAD/D101).
Antiretroviral therapy successfully suppressed HIV replication in older participantsVirological suppression rates varied minimally across age groups, indicating no age-related differences. As illustrated in Fig. 2f, older participants had higher rates of virological suppression than younger participants in the second year of ART (P = 0.02). No differences in virological suppression were observed among the three age groups at any other time point. At the end of follow-up, all groups demonstrated high rates of virological suppression, with the young group achieving 100%, the middle-aged group achieving 95.12%, and the older group achieving 98.69% (P> 0.05).
Adverse drug reactions impacted regimen modification in middle-aged and older individualsThe summary statistics for regimen modification were presented in Table S1, https://links.lww.com/QAD/D100. A combination of efavirenz (EFV) + lamividine (3TC) + tenofovir disoproxil (TDF) remained the primary regimen for all participants, accounting for 617 cases (38.04%) at initial ART and 561 cases (34.59%) at the end of follow-up. Nearly half of the participants (49.08%) changed their initial regimen, which was significantly higher in middle-aged (52.82%, n = 328) and older participants (52.14%, n = 293) compared with young participants (39.86%, n = 175) (P < 0.001). The combinations of EFV + 3TC + zidovudine (AZT) and nevirapine (NVP) + 3TC + AZT were commonly replaced by protease inhibitors or INSTIs because of their increased potency. Specifically, regimens including protease inhibitors increased to 17.77% (n = 78), 19.32% (n = 120), and 19.22% (n = 108) in the young, middle-aged, and older groups, respectively.
The reasons behind regimen changes were investigated. According to Table 2, the main reason for modifying regimens was ADRs, with a rate of 7.38 per 100 PYs (95% CI 6.84–7.96). Compared with younger and middle-aged participants, older participants were more likely to change regimens because of ADRs [11.93 per 100 PYs, 95% CI 9.99–14.19]. Middle-aged participants showed a significantly higher proportion of regimen changes because of polypharmacy or comorbidity. Younger participants had a greater probability of experiencing regimen changes because of personal reasons (2.80 per 100 PYs, 95% Cl 1.89–4.11), including financial constraints, maternity-related events, or self-administration of medications. No significant differences in the rate of treatment failures or optimized protocols among the three age groups.
Table 2 - Documented reasons for modification of treatment regimen among people with HIV during the follow-up. Reason for modification Total Younger Middle-aged Older Adverse drug reaction 7.38 (6.84–7.96) 7.73 (6.85–8.72) 6.09 (5.40–6.86) 11.93 (9.99–14.19) Personal reasons 0.77 (0.60–0.98) 2.80 (1.89–4.11) 0.46 (0.29–0.73) 0.56 (0.34–0.90) Polypharmacy or comorbidity 0.61 (0.46–0.81) 0.42 (0.13–1.14) 0.86 (0.61–1.2) 0.34 (0.18–0.63) Treatment failure 1.01 (0.82–1.26) 1.97 (1.23–3.12) 0.88 (0.63–1.22) 0.90 (0.62–1.31) Optimized protocols 0.46 (0.33–0.63) 1.25 (0.68–2.23) 0.37 (0.22–0.62) 0.34 (0.18–0.63)Events were expressed as per 100 person-years with 95% confidence intervals (CI).
As depicted in Table 3, a higher percentage of middle-aged (5.33 per 100 PYs, 95% Cl 4.73–6.01) and older participants (6.52 per 100 PYs, 95% Cl 5.77–7.36) experienced ADRs compared with younger participants (5.30 per 100 PYs, 95% Cl 4.41–6.34). Similarly, a considerably higher proportion of middle-aged and older participants experienced two or more different ADRs compared with younger participants (P < 0.01). Among the reported ADRs, the highest incidence of ADRs was bone marrow suppression (3.09 per 100 PYs, 95% Cl 2.60–3.66), followed by renal dysfunction (3.02 per 100 PYs, 95% Cl 2.54–3.58) and rash (2.26 per 100 PYs, 95% Cl 1.85–2.76). Older participants showed a higher rate of both bone marrow suppression and renal dysfunction compared with their younger counterparts, whereas younger individuals had a higher incidence of rash and digestive reactions (P < 0.01). No significant differences were found for the other types of ADRs among the three groups.
Table 3 - Treatment-emergent adverse drug reactions among people with HIV during follow-up. Total Younger Middle-aged Older ADR cases 5.74 (5.32–6.20) 5.30 (4.41–6.34) 5.33 (4.73–6.01) 6.52 (5.77–7.36) At least two kinds of ADR cases 1.74 (1.51–2.01) 0.87 (0.54–1.39) 1.73 (1.39–2.15) 2.25 (1.82–2.79) Kinds of ADRs Bone marrow suppressiona 3.09 (2.60–3.66) 3.98 (2.37–6.52) 2.57 (1.96–3.36) 3.50 (2.72–4.48) Renal dysfunctionb 3.02 (2.54–3.58) 1.99 (0.93–4.04) 3.00 (2.33–3.83) 3.28 (2.52–4.24) Rashesc 2.26 (1.85–2.76) 6.72 (4.56–9.74) 1.78 (1.28–2.46) 1.83 (1.28–2.60) Central nervous signsd 1.61 (1.27–2.05) 3.48 (1.99–5.91) 1.31 (0.89–1.92) 1.56 (1.06–2.27) Digestive reactione 1.43 (1.11–1.84) 3.98 (2.37–6.52) 1.03 (0.66–1.58) 1.33 (0.88–2.01) Abnormal liver functionf 1.06 (0.79–1.42) 3.23 (1.81–5.61) 0.98 (0.63–1.53) 0.67 (0.36–1.2) Osteoporosisg 0.92 (0.67–1.27) 0.50 (0.09–1.99) 0.80 (0.48–1.30) 1.17 (0.74–1.81) Abnormal lipid metabolismh 0.14 (0.06–0.32) 0.50 (0.09–1.99) 0.05 (0.00–0.30) 0.17 (0.04–0.53) Othersi 0.39 (0.24–0.64) 0.50 (0.09–1.99) 0.47 (0.24–0.89) 0.28 (0.10–0.69)ADR rates were expressed as ADR per 100 person-years with 95% confidence intervals (CI) based on an exact Poisson distribution. ADR, adverse drug reaction.
aBone marrow suppression was defined as a decrease in hemoglobin or hematocrit by more than 25% from baseline levels, hemoglobin levels of less than 70 g/l, and/or neutrophil counts less than 0.75 × 109/l.
bRenal dysfunction was defined as elevated serum creatinine, mild-to-moderate increase in urine albumin, and a reduction in creatinine clearance to less than 60 ml/min.
cRash was defined as participants experience symptoms such as itching, scaling, erythema, and blistering after ART.
dCentral nervous system reaction was defined as dizziness, headache, insomnia, dreaminess, mood disorders, poor concentration, depression, confusion, and even suicidal ideation, and in severe cases, delirium and cataplexy after ART.
eDigestive reaction were defined as nausea, vomiting, bloating, and diarrhea commonly occurring after ART.
fAbnormal liver function was characterized as serum transaminase levels exceeding 200 U/l or bilirubin levels surpassing 50 μmol/l.
gOsteoporosis was defined as T-score less than −2.5 indicates osteoporosis, and a T-score between −1 and −2.5 defines decreased bone mass.
hAbnormal lipid metabolism included fat deposition and lipoatrophy, often accompanied by hyperlipidemia. These abnormalities are characterized by fat atrophy in the limbs, buttocks, and face, alongside fat accumulation in the waist, back, and breasts. Fat atrophy is primarily observed in the face, limbs, and buttocks.
iOther ADRs include optic neuritis, mammary hyperplasia, hyperpigmentation, and gynecomastia.
We conducted a comprehensive analysis of immunological and virological outcomes in 1622 participants receiving ART in China over a follow-up period of 9 years. Our findings revealed that younger participants exhibited more robust immune recovery than middle-aged and older participants. Interestingly, despite different ages at ART initiation, both the middle-aged and older participants showed similar immunological responses to ART. This finding contradicted the observations made by Gras et al.[20], who reported that middle-aged participants had CD4+ T-cell counts ranging from 350 to 500 cells/μl at the beginning of ART but had higher median CD4+ T-cell counts than both younger and older participants after 8 years of ART. The reason could be attributed to the higher proportion of people who inject drugs and higher rates of HCV detection in the middle-aged group. Previous studies have suggested that people who inject drugs co-infected with HCV may exhibit poorer immunological responses and heightened susceptibility to treatment failure [21,22]. Furthermore, the middle-aged group had the lowest baseline CD4+ T-cell counts, factor known to contribute to suboptimal immune recovery.
Our findings regarding the impact of age on immune response to ART in younger and older participants align with earlier research [8,10,11,23]. In a multicenter cohort study, it was found that older participants had a median CD4+ T-cell count of 376 (IQR 279–474) cells/μl, while younger participants had a median CD4+ T-cell count of 424 (IQR 300–576) cells/μl (P = 0.0022; n = 3,024) [9]. Another study reported that a CIR (defined as an increase in CD4+ T-cell counts by 50–150 cells/μl during the first year of ART) was achieved in 92.5% of younger participants, compared with only 85.9% of older participants (P = 0.02), with a significant difference in the change of the CD4+/CD8+ ratio observed between the younger [0.27 (IQR 0.13–0.48)] and older groups [0.18 (IQR 0.09–0.39)] [11]. These findings suggest that older participants may exhibit a poor immune response to ART.
Several mechanisms may account for the diminished immune response observed in older individuals [24]. Firstly, the thymus tends to atrophy with increasing age, resulting in reduced naive CD4+ T-cell production, thymic output, and immunological repertoire [25,26]. This reduced thymic function may slow CD4+ T-cell recovery in older participants. Secondly, immunosenescence, the progressive decline and disruption of immune function with age, accelerated HIV progression. This has been observed in our previous studies using SIVmac239-infected macaques, where older macaques exhibited rapid development of HIV associated with preinfection immunosenescence characteristics, such as low naive CD4+ T cells and accumulated memory T cells [27,28]. Thirdly, CD4+ T cells in older individuals show elevated levels of immune activation [29], apoptosis, and depletion [30,31]. Additionally, disorders in secondary lymphoid tissues, dysregulated T-cell subsets, imbalanced cytokine levels, and chronic inflammation may further impede immune recovery in older participants [32]. The cumulative impacts of HIV infection and aging may contribute to overall dysfunction and inefficiency of the immune system [2,33].
The continued use of ART has been demonstrated to effectively suppress HIV replication [34,35]. Our study observed that most participants achieved high viral suppression by the end of the follow-up, with no significant disparities among the various age groups. Previous research has indicated that older participants experience higher levels of viral suppression and attain it more rapidly than their younger counterparts [10,35,36]. This may be attributed to better adherence among older participants. Although we did not directly measure adherence in our study, the strict inclusion criteria of participants who had been on ART for more than 3 years and had several complete follow-up visits may have resulted in higher adherence across all age groups, thus influencing the virological outcomes.
In our study, a high percentage of participants (46.61%, n = 756) adjusted their regimen, which is higher than previously reported [37], potentially because of our extended follow-up period. The reasons for regimen changes varied, including ADRs, treatment failure, optimization of treatment protocols, polypharmacy or comorbidity, as well as personal reasons [38]. Similar to previous studies [19,37,38], ADRs were the main reason for regimen changes. Middle-aged and older participants had a higher frequency of regimen changes and ADRs. Age-related physiological declines, such as decreased metabolism and excretion of drugs, changes in drug distribution volume and blood drug concentration, and polypharmacy, may contribute to drug-related toxicity in older participants [39,40]. Changes in ART can lead to diminished clinical and immunological benefits, lower adherence rates, failure to achieve viral suppression, heightened drug resistance, and elevated mortality and morbidity related to HIV [41]. Therefore, when selecting ART regimens for older participants, multiple factors such as potential organ failure, drug–drug interactions, and complications, should be fully considered to reduce the incidence of ADRs.
Although ART has revolutionized HIV prevention and treatment, older participants present unique challenges in achieving satisfactory immune reconstitution and prognosis. Developing new therapies to promote immune reconstitution and restore immune status remains a priority. Among current treatment regimens, regimens containing INSTIs like dolutegravir (DTG), raltegravir (RAL), bictegravir (BIC), elvitegravir (EVG), and cabotegravir (CAB) may be considered more frequently for older participants. These regimens have demonstrated efficacy and safety in clinical trials, and easier administration. The well tolerated nature in clinical trials further supports their potential benefits for older individuals [42]. The investigation by Foca et al.[43] revealed no virological failures among individuals aged 65 years and above who received an INSTI regimen, indicating strong and lasting effectiveness. The study by Kawashima et al.[44] demonstrated the safe use of the BIC+FTC+TAF regimen in men over 50 years, with no reported renal or hepatic failure and no significant correlation found between age and pharmacokinetic parameters. Importantly, no instances of virological failure and no observed changes in various health markers further support the well tolerated use of the regimen in older participants. Furthermore, the study conducted by Maggiolo et al.[45] in 86 predominantly male and white participants, with a median age of 69, reported high virological suppression rates at 24 and 48 weeks of treatment, along with sustained levels of CD4+ T cells and an increase in treatment satisfaction. These findings collectively emphasize the efficacy, safety, and tolerability of INSTIs in the older patient population. Despite the limited guidance on the use of INSTIs in older participants and cautionary advice in product labeling, available data suggest that INSTIs may be considered for use in geriatric participants [41–46]. Furthermore, novel therapeutic modalities and treatment strategies, including the ‘shock and kill’ approach for the elimination of latent HIV reservoirs, immunotherapies (such as neutralizing antibodies, cytokine adjuvant therapy, and immune checkpoint inhibitors), stem cell transplantation, and gene editing [47], have shown promising results in achieving a functional cure for HIV. However, more research is needed to evaluate their effectiveness and safety specifically in older participants.
Ample studies have examined the immune recovery pattern in PWH after starting ART and the factors that influence it. It is widely accepted that the age at ART initiated, baseline CD4+ T-cell counts, and baseline CD4+/CD8+ ratio are strongly assoc
留言 (0)