IMT exhibits a relatively high incidence in children and young individuals, accounting for 50% of primary benign lung tumors in infancy. IMT typically presents as a parenchymal nodule and, less frequently, as a slow-growing endobronchial lesion [2, 3]. The age range affected by IMT spans 3 to 13 years, although the incidence is presumed to be higher.
The clinical presentation of IMT is primarily influenced by its location. Some cases remain asymptomatic and are only incidentally discovered during imaging studies [8]. Children with endobronchial IMT often experience symptoms of bronchial irritation, including cough and occasional hemoptysis, which may be accompanied by chest pain [4, 9]. In some instances, patients may present with symptoms related to the local effects of the mass, such as stridor or a history of wheezing [5]. They may also exhibit signs of chronic inflammation, such as low-grade fever, weight loss, anemia, thrombocytosis, polyclonal hypergammaglobulinemia, elevated sedimentation rate, and C-reactive protein [10, 11].
In our case, the patient's clinical history and intermittent fever initially suggested an infectious disease. However, the lack of response to broad-spectrum antibiotics and the persistence of atelectasis prompted us to investigate the possibility of a non-infectious lesion, with chest high-resolution computer tomography (HRCT) proving to be a crucial diagnostic tool.
Central and endobronchial tumors account for only 10% of IMT cases, leading to bronchial obstruction and atelectasis. Central IMTs are typically identified earlier, possibly due to the resulting symptoms of acute obstruction. Conversely, peripheral parenchymal tumors present with more misleading and nonspecific symptoms, leading to delayed diagnosis [12].
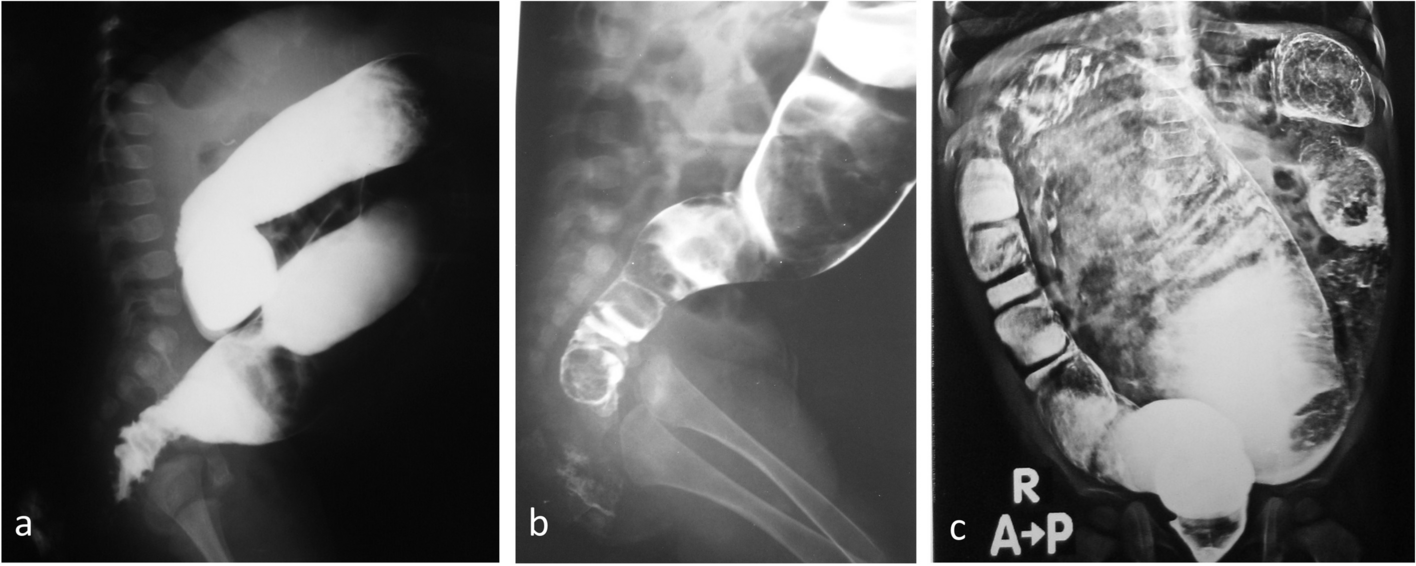
The differential diagnosis of IMT should include foreign body aspiration, infectious diseases (e.g., Aspergillus and Mycobacterium), necrotizing pneumonia, and spindle cell neoplasms [1]. Chest X-rays usually reveal a peripheral lesion or nodule of varying sizes (1.2 to 15 cm in diameter). On HRCT, IMTs often appear as solid single masses with homogeneous or heterogeneous enhancement, well-defined borders, a lobulated appearance, and occasional punctate calcifications, mimicking malignant tumors. Additionally, associated findings may include pneumothorax, pleural effusion, atelectasis, cavitations, and lymphadenopathies [13, 14].
Bronchoscopy is indicated when there is suspicion of an endoluminal lesion. It serves as both a diagnostic and therapeutic tool, allowing for the removal of tumoral obstructions and the collection of biopsy samples [15,16,17,18].
The anatomopathological differential diagnosis is broad and relies on the clinical presentation, morphological alterations, and the immune phenotype of spindle cells. Histological assessment is crucial to rule out malignant mesenchymal tumors such as sarcomas and gastrointestinal stromal tumors [8, 19, 20].
Molecular rearrangements on chromosome 2p23 have been detected in several IMT cases (34–56% of both pulmonary and extrapulmonary IMTs). This locus harbors the human ALK gene, which codes for a tyrosine kinase receptor known as ALK. ALK rearrangements can be identified through immunohistochemical analysis using the monoclonal ALK-1 antibody and appear to be highly specific for these lesions. However, they may not be a sensitive marker in children [12, 21]. ALK-positivity does not seem to correlate with recurrence [6, 22, 23]. Other genetic abnormalities have also been implicated, such as aneuploidy, RET gene rearrangement, EML4-ALK inversion, and fusions of other kinase genes. Cytologic atypia and positive ALK status are more frequent in aggressive tumors, whereas metastatic tumors tend to be harmful for ALK. Additionally, positive immunohistochemical staining has been reported for vimentin, alpha-smooth muscle actin (alpha-SMA), ALK, and other markers such as desmin, cytokeratin (AE 1–3), CD34, protein S-100, and HHV8 [12, 24].
The primary treatment for IMT involves complete, yet conservative, surgical excision. This approach is essential to prevent recurrence. Adequate histologic assessment should precede surgery, typically achieved through needle biopsy during bronchoscopy, to avoid unnecessary procedures. The choice of surgical approach (e.g., wedge resection by bronchotomy with lobectomy or pneumonectomy) depends on factors such as the tumor's size and location, its relationship with surrounding structures, and the surgeon's experience with the available equipment. In cases where complete removal is not feasible due to invasion of vital structures, partial resection may be necessary [2, 4, 17, 20, 25].
Chemotherapy may be considered an alternative option for patients with microscopic or macroscopic residual disease, although its efficacy remains controversial. Complete surgical excision is the recommended treatment, which gives long-term survival benefits. Whenever a mass is resectable, lobectomy and pneumonectomy are better options than wedge resection or endobronchial resection for preventing local recurrence and metastasis. also, this can be controverted in the pediatric area given the growing period in childhood and the associated morbidity. A total lobectomy or pneumonectomy vs. local resection is an essential decision in a pediatric patient; when technically feasible, a sleeve resection of the involved bronchus is also recommended [21].
Recurrence is a rare phenomenon, occurring in only 14% of cases. Recent evidence suggests a 5 to 10-year disease-free survival rate of 89% following complete resection. The prognosis is good in up to 95% of the cases. The risk of recurrence justifies a long-term clinical follow-up. Indeed, bronchoscopy should be performed only in cases of severe respiratory symptoms [23,24,25,26].
Treatment received and available clinical and imaging follow-ups were noted to look for the presence or absence of local recurrence, transformation to sarcoma, and metastasis to assess malignant potential. Patients with multiple lesions at presentation were presumed to be multifocal in origin. Subsequent presentation with a new focal lesion at a different site was considered metastatic.



留言 (0)