The emergence of CRKP presents a significant challenge to worldwide public health, posing a substantial obstacle to effective clinical infection management [4, 11,12,13]. This study sought to explore the drug resistance profile and epidemiological features of CRKP at the CMC, with the overarching goal of implementing effective measures to curb the spread of CRKP infections among pediatric patients. In this study, 32.5% of K. pneumoniae isolates demonstrated carbapenem resistance. According to the latest meta-analysis, the global prevalence of CRKP in patients with K. pneumoniae infections was 28.69% (95% CI: 26.53–30.86%) [14]. In a previous study conducted at CMC between January 2018 and April 2020, K. pneumoniae isolates showed resistance rates of 38% to imipenem and 20% to meropenem.
In our study, the prevalence of MBL-producing K. pneumoniae isolates was found to be 44%, aligning with previous findings [8]. Among CKCP and MBL-producing isolates, the prevalence of the blaNDM gene was 20% and 83%, respectively. Notably, the prevalence of the blaNDM gene surpassed previous reports, wherein only 42% of MBL-producing isolates tested positive for blaNDM [8].
The high prevalence of CRKP complicates the management of nosocomial infections, underscoring the urgency for a reassessment of current infection control protocols and antibiotic stewardship strategies. The predominant risk factors commonly associated with CRE infection include the utilization of indwelling medical devices, previous exposure to antibiotics, and admission to the ICUs [4]. The substantial number of CRKP isolates, particularly isolated from urine (37%) and blood (28%), suggests a potential association with the utilization of indwelling medical devices. Urinary catheters and central venous catheters, frequently utilized in healthcare settings to address diverse medical needs and ensure critical patient care, establish an optimal environment for bacterial colonization. Moreover, prior antibiotic exposure is identified as another key risk factor driving the emergence and spread of CRE infections [15]. All patients included in our study had a history of previous hospitalization and prior antibiotic use. Enhanced infection control measures, including stringent adherence to hand hygiene protocols, judicious use of indwelling medical devices, and implementation of antimicrobial stewardship programs to optimize antibiotic use, are essential for controlling the spread of CRE.
Twenty-six CRKP isolates (48%) were obtained from ICUs, aligning with findings from other studies that have consistently reported the highest incidence of CRKP infections among patients admitted to ICU wards [16, 17]. According to the latest meta-analysis, the prevalence of hospital-acquired CRKP infections is notably high in ICUs, with a pooled estimate of 62.31% [14]. ICUs, characterized by high patient acuity, prolonged hospital stays, and frequent invasive procedures, provide a conducive environment for the transmission of healthcare-associated pathogens like CRE [18]. Furthermore, the compromised immune status of ICU patients, coupled with the frequent use of broad-spectrum antibiotics and invasive medical interventions, further heightens their susceptibility to CRE infections.
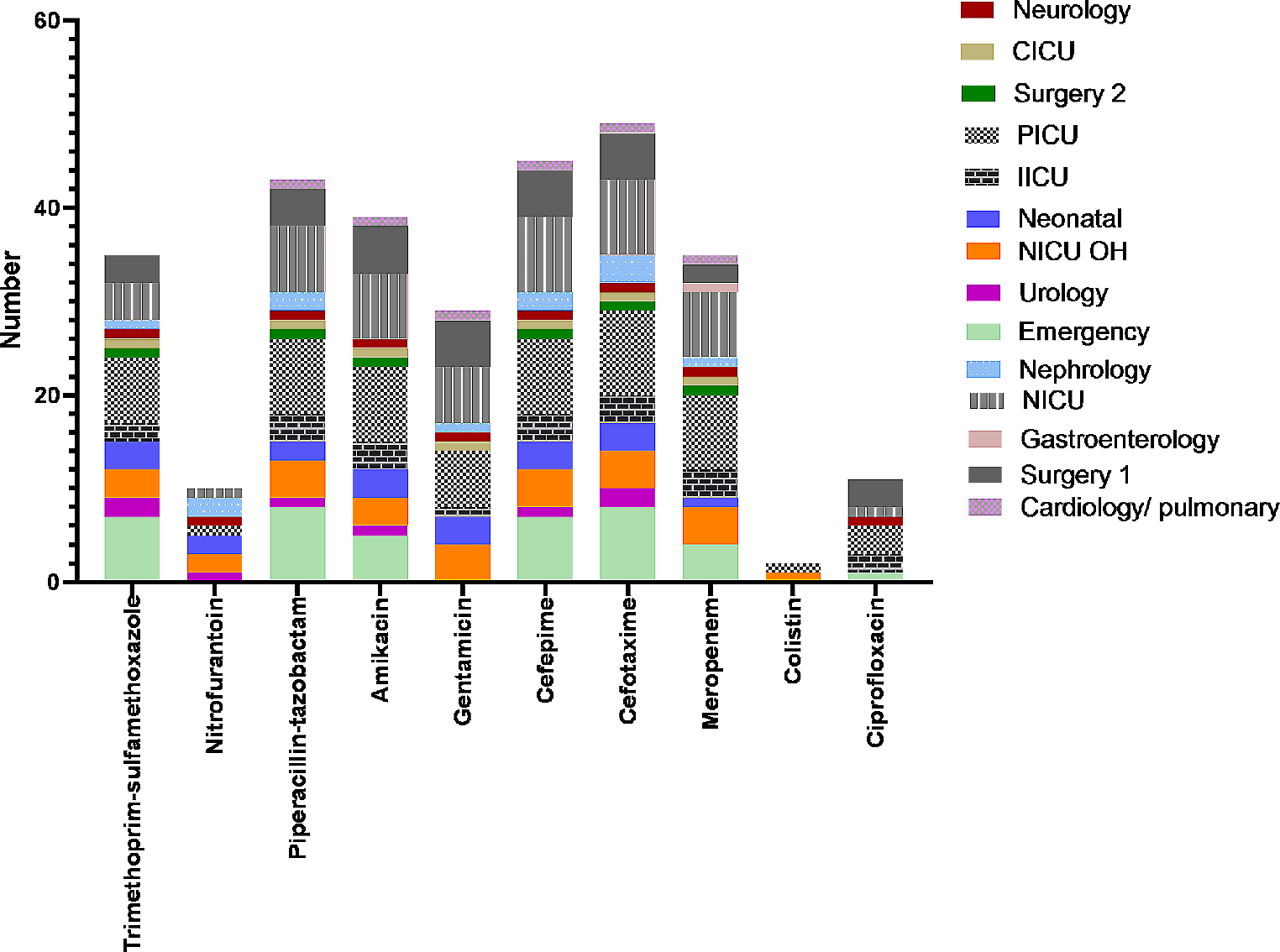
All CRKP isolates in our study were multidrug-resistant and showed high resistance to piperacillin-tazobactam and cephalosporins. The prevalence of resistance to colistin, and ciprofloxacin was low, which may be because of limited use of these antibiotics in children. This suggests that ciprofloxacin or colistin, in conjunction with other antibiotics such as meropenem and imipenem, may be useful for the treatment of complex CRKP infections.
Multiple outbreaks of CRKP infections carrying blaNDM genes have been reported in Iran [7, 19,20,21,22]. Research conducted in Turkey, Egypt, and Greece, examining the PFGE patterns of clinical CRKP isolates, has provided significant evidence supporting the transmission and prevalence of resistance within hospital wards, particularly in ICU settings [23,24,25]. In the investigation conducted by Tao et al. in China, the PFGE analysis of the 86 CRKP strains demonstrated their segregation into 15 separate clusters, primarily found within neonatal medicine, neonatal ward and ICU [26]. In the study conducted by Celikbilek et al. in Turkey, PFGE analysis revealed that over half of the CRKP isolates were grouped into clusters. However, cross-transmission was not limited to a specific wards or time period [25].
The current study also demonstrated that cross-transmission was not restricted to a single ward. For instance, despite the 13 CRKP isolates being clustered within the largest PFGE type, they were identified across various wards, including the CICU, emergency, urology, surgery, nephrology, cardiopulmonary, PICU, IICU, and neonatal department. Four CRKP isolates observed in cluster C harbored the blaNDM gene and were isolated from different ICU wards and emergency department. A significant association was observed between cluster C and the presence of the blaNDM gene. The lack of adequate infection control measures in our hospital raise concerns regarding the potential spread of CRKP through patient transfers, particularly from the emergency department to other wards. The detection of the blaNDM gene in other clusters implies the dissemination of this resistance gene across different wards within the hospital, thereby indicating the possibility of transmission to all wards. This clonal expansion has the potential to be transmitted to patients via personnel, equipment, or contaminated surfaces [25]. Therefore, it is highly recommended to enforce rigorous infection control protocols, encompassing effective isolation measures, thorough cleaning and disinfection protocols, and strict compliance with hand hygiene practices, to control the dissemination of CRKP within the hospital setting. Effective communication and collaboration among healthcare teams are vital to ensure that patients with CRKP colonization or infection are appropriately managed during transfers, thus minimizing the risk of further dissemination [5, 27].
While the blaNDM gene is a significant contributor to carbapenem resistance, there are other mechanisms, such as the production of carbapenemases like KPC and OXA enzymes, as well as non-enzymatic mechanisms involving alterations in porins and efflux pumps, that can also confer resistance to carbapenems. Understanding the full spectrum of resistance mechanisms is essential for developing comprehensive strategies to combat carbapenem-resistant infections effectively.
The study faced a limitation in its capacity to differentiate between colonization and infection with CRKP. An in-depth analysis of the definition of nosocomial infections could have provided a stronger foundation for the study and improved the interpretation of its findings. Conclusion.
In conclusion, our study revealed a concerning prevalence of carbapenem resistance among K. pneumoniae isolates. Specifically, the detection of the blaNDM gene in 20% of CRKP isolates, with a significant proportion (82%) observed in isolated CRKP from the ICUs and emergency departments, underscores the potential clonal expansion of these resistant strains within these critical hospital wards.




留言 (0)