
記住我


The HIV and substance use (SU) epidemics are deeply intertwined in the United States; it is well-established that people with HIV who engage in SU experience barriers to care, leading to lower retention, poor viral suppression, and other gaps along the HIV care continuum.1–4 SU contributes to HIV acquisition through injection drug use and particularly among cisgender women, through sexual routes due to challenges, such as impaired ability to negotiate with partners.3,5 The epicenter of the HIV epidemic is in the South, which faces the highest burden of HIV compared with other regions of the country.6 Similarly, higher rates of substance use disorder (SUD) and gaps in capacity for SUD treatment have been identified in the Southeast United States.7–9 Women comprise 20% of the 40,000 annual new diagnoses in the United States and are disproportionately affected in the South.10,11 Therefore, implementing strategies to improve gaps in the continuum and treatment access for both HIV and SU for women in the South is crucial to end the syndemic.
Evidence-based interventions for SUD12,13 have been shown to facilitate antiretroviral therapy (ART) initiation, uptake, and possibly viral suppression.14–16 However, the implementation gaps in these interventions among women living with HIV (WWH), particularly in the South, are unknown, due in part to underrepresentation of women in HIV research and limited sex disaggregated data. A SU care continuum, in conjunction with the HIV care continuum, would be useful to identify critical gaps in care from prevention to recovery and implement solutions to address such gaps.17,18 Unfortunately, data to populate such a tool are lacking for WWH.
We describe SU treatment utilization and HIV care outcomes over time among WWH and comparable women without HIV (WWOH) across the Southern United States. Through characterizing SU, SU treatment, and HIV outcomes over time in this understudied population, we seek to provide a foundation for an integrated SU and HIV care continuum to guide future care strategies.
METHODS Study PopulationThe Women's Interagency HIV Study (WIHS) is a large, prospective cohort study of WWH and demographically similar cisgender WWOH across 10 US sites.19 Four sites (Atlanta, Birmingham/Jackson, Chapel Hill, and Miami) in the South were added between October 2013 and March 2015 given the growing epidemic in this region. Additional details on eligibility criteria and recruitment methods have been published previously.19 To provide contemporary data on SU, we included women enrolled in the WIHS Southern sites from 2013 to 2015 and followed over time in this analysis. Participants who transferred from non-Southern sites were excluded. Participants had study visits every 6 months with standardized interviews, physical examinations, and biospecimen collection.19 All WIHS participants provided written informed consent for study participation. The WIHS protocol20 was approved by each site's Institutional Review Board.
MeasuresSU was defined as self-reported nonmedical use of drugs in the past year, including crack/cocaine, methamphetamines, and nonprescription opioids such as heroin; the use of tobacco, alcohol, or marijuana alone was not included in this definition, consistent with prior literature.21–23 SU frequency by drug type in the past 6 months was classified based on self-report (none, monthly, weekly, daily). SU treatment was defined as self-reported use of medications for opioid use disorder (obtained through prescription or self-treatment by the individual) or attendance at drug treatment programs in the past year. Drug treatment programs included inpatient and outpatient detoxification programs, halfway houses, buprenorphine/methadone maintenance programs, justice system-based programs, and Narcotics Anonymous. Polysubstance use was defined as use of more than 1 category of drugs (crack/cocaine, opioids, and methamphetamine). Depressive symptoms were defined as a Center for Epidemiologic Studies-Depression score ≥ 16.24 Retention in HIV care was defined as a self-reported attendance of an HIV care visit within the past 6 months, and viral suppression was defined as a study viral load <200 copies/mL.19
AnalysisDemographic, clinical, and sociobehavioral characteristics were summarized for women who reported SU in the past year at enrollment. Within this population, SU and SU treatment were determined at enrollment, 1, 2, and 3 years; overall and stratified by HIV serostatus; and compared using χ2, Fisher exact test, or Wilcoxon signed-rank test, where appropriate. Although standardized definitions for retention in SU care do not exist, year-long intervals were chosen as these periods of time were more appropriate for conceptualizing clinically relevant SU treatment engagement over time.25,26 Study visits closest to the specified year were included. Regarding HIV care outcomes, HIV care visits and viral loads in the past 6 months were determined at enrollment and subsequent time points, which were stratified by SU treatment status and compared using χ2 and Fisher exact tests, where appropriate. Missing viral load and interview data were infrequent (≤5% of the data) and were excluded from analysis.
RESULTS Demographic CharacteristicsRegarding overall Southern site cohort characteristics, of 840 women (608 WWH, 232 WWOH), 51% (n = 432) reported SU in their lifetime (49% WWH, 57% WWOH) and 18% (n = 155) reported SU in the past year (16% WWH, 24% WWOH).
Among these 155 women reporting SU in the past year who were included in subsequent analysis, the median age was 47 years, 78% identified as non-Hispanic Black, 85% reported previous incarceration, 82% reported current cigarette use, and 46% endorsed >7 drinks/week (Table 1). Regarding mental health, 53% reported depressive symptoms and 40% attended a mental health visit in the past 6 months. Overall, 86% attended a health care provider visit, and among WWH, 88% attended an HIV care visit and 62% were virally suppressed in the past 6 months.
TABLE 1. - Demographic, Sociobehavioral, and Clinical Characteristics at Enrollment Among WIHS Participants Enrolled in Southern US Sites From 2013 to 2015 Who Reported SU in the Past Year Stratified by HIV Status (n = 155) OverallColumn percents may not total 100 due to rounding. Bold entries are variables with values (p < 0.05).
*P value from χ2 unless otherwise noted.
†Wilcoxon test.
‡Fisher exact test.
§Else refers to all races/ethnicities except non-Hispanic Black: non-Hispanic White n = 22, Hispanic n = 7, Native American/Alaskan n = 4, and other = 1.
║Health insurance includes public, private, and Ryan White benefits.
¶Collected at the first follow-up visit after enrollment.
#Heavy drinking defined as consuming more than 7 drinks per week.
**Defined as Center for Epidemiologic Studies-Depression score ≥ 16.
††Among women living with HIV only.
‡‡Polysubstance was defined as >1 drug from 3: crack/cocaine, opioids, and methamphetamine only.
§§Self-reported frequency of use in the past 6 months.
cART, combination antiretroviral therapy; NA, not applicable.
On SU, 89% reported crack/cocaine, 6% reported opioids, 1% reported methamphetamine, and 6% reported polysubstance use. Regarding SU frequency, 39% (n = 61) reported crack/cocaine monthly, 32% (n = 49) weekly, and 17% (n = 27) daily and <1% (n = 1) reported opioids monthly, 2% (n = 3) weekly, and 3% (n = 5) daily. Over time, 80% (n = 118), 56% (n = 79), and 53% (n = 73) of women still reported SU at 1, 2, and 3 years after enrollment. By HIV status, 79% (n = 74), 53% (n = 48), and 55% (n = 48) WWH reported SU at 1, 2, and 3 years, respectively, and 82% (n = 44), 62% (n = 31), and 50% (n = 25) WWOH reported SU at these time points.
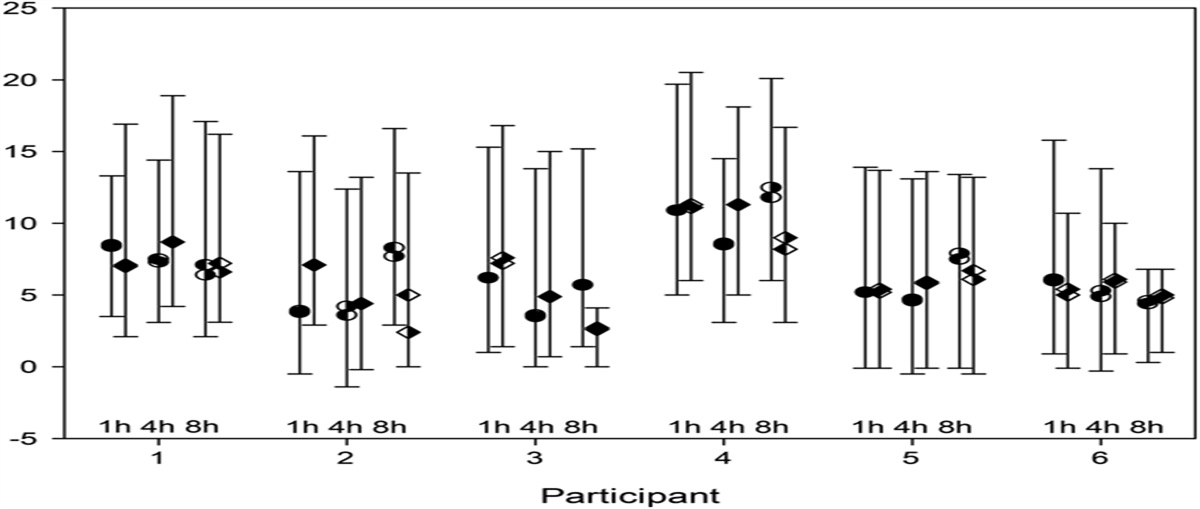
SU TreatmentOn treatment use, 25% (n = 38) at enrollment reported SU treatment in the past year (28% WWH, 18% WWOH, P = 0.17), including 26% (n = 36) and 40% (n = 4) of women who reported crack/cocaine and opioids, respectively. Of those engaged in polysubstance use, 40% (n = 4) reported treatment utilization. Overall, 30% (n = 45), 21% (n = 30), and 18% (n = 25) reported SU treatment at 1, 2, and 3 years; 38% (n = 57) reported SU treatment during at least 1 follow-up time point. While fewer WWOH reported SU treatment than WWH at enrollment, SU treatment engagement did not significantly differ by HIV serostatus at any time point (Fig. 1). Among WWH, 41% (n = 39) reported SU treatment during at least 1 follow-up time point vs. 33% (n = 18) WWOH (P = 0.38).
 FIGURE 1.:
FIGURE 1.: SU treatment among WWH and comparable WWOH who reported SU in the past year at enrollment in the Southern US WIHS sites at enrollment, 1, 2, and 3 years (2013–2018).
HIV Care OutcomesAmong WWH, 88% (n = 80), 87% (n = 79), 91% (n = 81), and 83% (n = 72) reported an HIV care visit in the past 6 months at enrollment, 1, 2, and 3 years, respectively. Retention in HIV care did not significantly differ by SU treatment engagement at any time point (P = 0.74, P > 0.99, P = 0.36, and P = 0.73, respectively). At enrollment, 62% (n = 59) were virally suppressed, 80% (n = 20) among those reporting SU treatment, and 56% (n = 39) among those not reporting treatment (P = 0.032). Over time, 71% (n = 65), 81% (n = 70), and 72% (n = 60) were virally suppressed at 1, 2, and 3 years without significant differences by SU treatment engagement (P = 0.56, P > 0.99, P = 0.37, respectively).
DISCUSSIONThis is the first description of SU, SU treatment, and corresponding HIV outcomes over time among women in the South. Our findings illustrate that while lifetime and past year SU were high in this observational cohort, only 1 in 4 women reported SU treatment engagement. Reflective of the HIV epidemic among women in the South, women reported primarily cocaine use, for which treatment is more variable and less standardized, unlike for opioid use disorder.23,27 National studies of WWH, WWOH, and reproductive age women report 9%–42% past year SU treatment.23,28 Adding to this literature, our analysis revealed low SU treatment over time for WWH and WWOH, demonstrating a critical gap in understanding treatment uptake and continuation. Furthermore, this gap was observed despite 86% of the study population reporting health care utilization in the past 6 months, suggesting that integrated solutions in various health care settings are needed to improve these potential access points for SU treatment. Given the high rate of prior justice system involvement in the study population, integrated care considering re-entry into the community should also be considered.
Although the care continuum framework has shaped HIV prevention and care, it has only recently emerged in the SU treatment literature.17,29–32 By characterizing SU, SU treatment, and HIV outcomes over time, our analysis illustrates data that can be used to populate a SU care continuum for individuals with HIV, variations of which have been proposed,17,18,33 to identify points for intervention and/or promotion of integrated HIV and SU care models. For example, we found that while SU treatment increased in the first year in this population, WWH and WWOH experienced substantial drop off in SU and SU treatment between 1 and 2 years while maintaining HIV outcomes. This may be a critical time point to add support for continued SU treatment engagement for those who may benefit in the context of HIV and other primary care services. Alternatively, given a drop off in both SU and SU treatment, it could represent the successful treatment of SUD in a subset of women by this time point. These 2 different implications reflect limited understanding of the optimal benchmarks for a SU care continuum, unlike in HIV care. For example, the optimal time for retention in SU treatment is not well-defined as evident by the range of timelines applied to analyze retention.25,34,35 Our analysis supports the need to better understand such drop offs through future qualitative work and larger epidemiologic studies for robust data on SU and treatment patterns to develop an evidence base which can address these gaps and inform appropriate benchmarks. Future studies must investigate how achievement of benchmarks in the SU and HIV care continuums overlap and differ to guide integrated care strategies in HIV, sexual health, and primary care settings.
Limitations of this analysis include that the study population may not be nationally representative, but as this is the largest cohort study of WWH and WWOH in the United States, our findings focus on the region that is the center of the US HIV epidemic. While we were not able to explore the role of pregnancy in this analysis, this is a critical area of service integration for reproductive age WWH and must be prioritized in future implementation and research. SU and treatment utilization were self-reported in questionnaires, which may yield desirability bias and potential misclassification. Although we were not able to assess the drivers of SU discontinuation and reasons for treatment disengagement, our study creates the foundation for qualitative work and multistate analyses to further quantify the cyclical nature of SU and treatment and define future benchmarks for successful treatment. This analysis also does not capture the formal diagnosis of SUD and was not able to characterize outcomes by degree of SU. However, by using SU in the past year as a proxy for SUD, this study offers novel data regarding SU, SU treatment, and HIV care patterns over time in a population for whom integrated services is essential to ending the syndemic.
Our results emphasize a crucial need to systematically explore opportunities to integrate SU treatment with other health care services and across diverse settings, such as community health clinics and the justice system, for this important and historically neglected population. Such work is critical for policy development and program implementation to bridge the gaps in SU and HIV care for women in the South. Such informed and integrated implementation focused on high-priority populations will bring us closer to ending the SU and HIV epidemics.
ACKNOWLEDGMENTSData in this manuscript were collected by the Women's Interagency HIV Study (WIHS), now the Multicenter AIDS Cohort Study/WIHS Combined Cohort Study (MWCCS). The authors gratefully acknowledge the contributions of the study participants and dedication of the staff at the MWCCS sites. The authors thank the WIHS site co-investigators for serving as site liaisons for data collaboration. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
REFERENCES 1. Chavis NS, Klein PW, Cohen SM, et al. The health resources and services administration (HRSA) ryan white HIV/AIDS program's response to the opioid epidemic. J Infect Dis. 2020;222(suppl 5):S477–S485. 2. Jarlais DCD, Arasteh K, McKnight C, et al. Providing ART to HIV seropositive persons who use drugs: progress in New York city, prospects for “ending the epidemic”. AIDS Behav. 2016;20:353–362. 3. Azim T, Bontell I, Strathdee SA. Women, drugs and HIV. Int J Drug Pol. 2015;26(suppl 1):S16–S21. 4. Cook JA, Burke-Miller JK, Steigman PJ, et al. Prevalence, comorbidity, and correlates of psychiatric and substance use disorders and associations with HIV risk behaviors in a multisite cohort of women living with HIV. AIDS Behav. 2018;22:3141–3154. 5. Darlington CK, Lipsky RK, Teitelman AM, et al. HIV risk perception, pre-exposure prophylaxis (PrEP) awareness, and PrEP initiation intention among women who use drugs. J Subst Use Addict Treat. 2023;152:209119. 6. Fauci AS, Redfield RR, Sigounas G, et al. Ending the HIV epidemic: a plan for the United States. JAMA. 2019;321:844–845. 7. Abraham AJ, Andrews CM, Yingling ME, et al. Geographic disparities in availability of opioid use disorder treatment for medicaid enrollees. Health Serv Res. 2018;53:389–404. 8. Hand DJ, Short VL, Abatemarco DJ. Substance use, treatment, and demographic characteristics of pregnant women entering treatment for opioid use disorder differ by United States census region. J Subst Abuse Treat. 2017;76:58–63. 9. Short VL, Hand DJ, MacAfee L, et al. Trends and disparities in receipt of pharmacotherapy among pregnant women in publically funded treatment programs for opioid use disorder in the United States. J Subst Abuse Treat. 2018;89:67–74. 10. CDC Issue Brief: HIV in the Southern United States. 2019. Available at: https://www.cdc.gov/hiv/pdf/policies/cdc-hiv-in-the-south-issue-brief.pdf. Accessed January 31, 2022. 11. HIV Among Women. Centers for Disease Control and Prevention (CDC); https://www.cdc.gov/hiv/pdf/group/gender/women/cdc-hiv-women.pdf (2021, Accessed June 1, 2023). 12. Hadland SE, Yule AM, Levy SJ, et al. Evidence-based treatment of young adults with substance use disorders. Pediatrics. 2021;147(suppl 2):S204–s214. 13. Stockings E, Hall WD, Lynskey M, et al. Prevention, early intervention, harm reduction, and treatment of substance use in young people. Lancet Psychiatry. 2016;3:280–296. 14. Warner LA, Wei W, McSpiritt E, et al. Ante- and postpartum substance abuse treatment and antiretroviral therapy among HIV-infected women on Medicaid. J Am Med Womens Assoc (1972). 2003;58:143–153. 15. Stein MD, Rich JD, Maksad J, et al. Adherence to antiretroviral therapy among HIV-infected methadone patients: effect of ongoing illicit drug use. Am J Drug Alcohol Abuse. 2000;26:195–205. 16. Gonzalez A, Barinas J, O'Cleirigh C. Substance use: impact on adherence and HIV medical treatment. Curr HIV/AIDS Rep. 2011;8:223–234. 17. Eaton EF. “Rapid start” treatment to end the (other) epidemic: walking the tightrope without a net. Clin Infect Dis. 2021;72:479–481. 18. Korthuis PT, Edelman EJ. Substance use and the HIV care continuum: important advances. Addict Sci Clin Pract. 2018;13:13. 19. Adimora AA, Ramirez C, Benning L, et al. Cohort profile: the women's interagency HIV study (WIHS). Int J Epidemiol. 2018;47:393–394i. 20. Bacon MC, von Wyl V, Alden C, et al. The Women's Interagency HIV Study: an observational cohort brings clinical sciences to the bench. Clin Diagn Lab Immunol. 2005;12:1013–1019. 21. Montgomery L, Bagot K, Brown JL, et al. The association between marijuana use and HIV continuum of care outcomes: a systematic review. Curr HIV/AIDS Rep. 2019;16:17–28. 22. Sinha S, McCaul ME, Hutton HE, et al. Marijuana use and HIV treatment outcomes among PWH receiving care at an urban HIV clinic. J Subst Abuse Treat. 2017;82:102–106. 23. Fujita AW, Ramakrishnan A, Mehta CC, et al. Substance use treatment utilization among women with and without human immunodeficiency virus. Open Forum Infect Dis. 2023;10:ofac684. 24. Radloff LS. The CES-D scale: a self-report depression scale for research in the general population. Appl Psychol Meas. 1977;1:385–401. 25. Fine DR, Lewis E, Weinstock K, et al. Office-based addiction treatment retention and mortality among people experiencing homelessness. JAMA Netw Open. 2021;4:e210477. 26. Radfar N, Radfar SR, Mohammadi F, et al. Retention rate in methadone maintenance treatment and factors associated among referred patients from the compulsory residential centers compared to voluntary patients. Front Psychiatry. 2023;14:1139307. 27. Penberthy JK, Ait-Daoud N, Vaughan M, et al. Review of treatment for cocaine dependence. Curr Drug Abuse Rev. 2010;3:49–62. 28. Martin CE, Scialli A, Terplan M. Unmet substance use disorder treatment need among reproductive age women. Drug Alcohol Depend. 2020;206:107679. 29. Socías ME, Volkow N, Wood E. Adopting the 'cascade of care' framework: an opportunity to close the implementation gap in addiction care? Addiction. 2016;111:2079–2081. 30. Stanojlović M, Davidson L. Targeting the barriers in the substance use disorder continuum of care with peer recovery support. Subst Abuse. 2021;15:1178221820976988. 31. Williams AR, Nunes EV, Bisaga A, et al. Developing an opioid use disorder treatment cascade: a review of quality measures. J Subst Abuse Treat. 2018;91:57–68. 32. Perlman DC, Jordan AE. Considerations for the development of a substance-related care and prevention continuum model. Front Public Health. 2017;5:180. 33. Eaton EF, Tamhane A, Turner W, et al. Safer in care: a pandemic-tested model of integrated HIV/OUD care. Drug Alcohol Depend. 2022;231:109241. 34. Bakouni H, McAnulty C, Tatar O, et al. Associations of methadone and buprenorphine-naloxone doses with unregulated opioid use, treatment retention, and adverse events in prescription-type opioid use disorders: exploratory analyses of the OPTIMA study. Am J Addict. 2023;32:469–478. 35. Tierney HR, Takimoto SW, Azari S, et al. Predictors of linkage to an opioid treatment program and methadone treatment retention following hospital discharge in a safety-net setting. Subst Use Misuse. 2023;58:1172–1176.
留言 (0)