
記住我


The safety and efficacy of HIV pre-exposure prophylaxis (PrEP), in which people who are not living with HIV take antiretroviral medications to avert HIV infection, has been robustly demonstrated.1 Since the advent of PrEP, new PrEP agents and modes of administration for PrEP have expanded the options for HIV pre-exposure prophylaxis.2–4 Extensive PrEP scale-up, alongside universal antiretroviral treatment for people living with HIV, could drastically reduce, or even eliminate, HIV transmission.5
Despite the enormous potential of PrEP as an HIV prevention tool, PrEP use has lagged in key populations in the United States and remains far short of global benchmarks. PrEP is indicated for approximately 1.2 million people in the United States according to the Centers for Disease Control and Prevention.6 In 2022, only 36.0% of all those for whom PrEP was recommended prescribed it. That year, among Black/African American and Hispanic/Latino people for whom PrEP was indicated, 12.8% and 24.4%, respectively, were taking PrEP. Globally, PrEP use fell far short of UNAIDS’ targets of 3 million people taking PrEP by 2020, with fewer than 500,000 having initiated PrEP by that deadline.7
Telehealth or telemedicine, the use of electronic communication to manage patient health,8 is a promising approach to increasing PrEP access, and the adoption of PrEP telehealth was accelerated by the COVID-19 pandemic because it motivated providers to find low-contact means of delivering PrEP care.9,10 In addition to having evident advantages in the setting of an air-borne pandemic, PrEP telehealth interventions may simplify interactions with the health care system, reduce societal obstacles such as lack of transportation to appointments, and lessen the impact of stigma by allowing participants to access PrEP more privately.11
In the United States, numerous commercial and nonprofit providers of PrEP telehealth care have emerged in recent years, with multiple nationwide companies providing telehealth care.12 Preliminary evidence from research on these early efforts suggests that PrEP telehealth is well received, often preferred to traditional models, and has been effective in delivering PrEP care to its clients.13–29 There have been relatively few reports in the literature on PrEP telehealth outside the United States, but efforts have been described in Brazil, Vietnam, Thailand, Germany, and Kenya.27,30,31
Despite growing attention to telehealth approaches as an avenue for dispensing PrEP, research to date on PrEP telehealth delivery has mostly been confined to reports on implementation or the acceptability of these interventions to patients. A trial of an online dyadic counseling intervention for HIV prevention did not find any significant gains in PrEP use among those randomized to the intervention arm.32 In this study, we report on findings related to effectiveness from a randomized controlled trial of PrEPTECH (ClinicalTrials.gov NCT04902820), a telehealth intervention that aims to tackle the challenges of accessing PrEP that young people encounter in traditional models of care.33
METHODS Study PopulationParticipants residing in 4 regions within the United States—the nine-county San Francisco Bay Area, CA; Los Angeles County, CA; Miami-Dade County, FL; and Broward County, FL—were recruited between February and September 2022. To be included, participants had to report having sex with men and either identify as a cisgender male and be in the age group of 15–17 years (in California only; minors in Broward or Miami-Dade Counties were ineligible due to ambiguous parental notification requirements in Florida34); identify as a cisgender male and be in the age group of 18–27 years; or identify as a transgender female and be in the age group of 18–27 years. In addition, participants had to qualify for PrEP by virtue of self-reporting being diagnosed with a sexually transmitted infection (STI) in the past 6 months or self-reporting condomless anal intercourse in the past 90 days. Participants were ineligible if they had taken PrEP in the past 30 days or had been diagnosed with HIV infection, hepatitis B infection, and chronic kidney, liver, or bone disease.
Study Procedures Recruitment, Screening, and EnrollmentParticipants were recruited through advertising campaigns on social media and LGBTQ+ dating applications and in-person and virtual outreach by community-based organizations. Each prospective participant initially created an account on the PrEPTECH website, authenticating their phone number and email addresses in the process, was screened for eligibility, and confirmed their identity by providing a photograph of themselves holding a visible photograph ID or sharing an active public social media profile on which their name was displayed. Approved participants who provided their informed consent and took the baseline survey were randomized, informed of their assignment, and directed to online PrEP resources (if randomized to control) or their next steps in accessing PrEP through PrEPTECH (if randomized to the intervention). Incentives were paid for each of the 3 surveys completed. The study was approved by the ETR Institutional Review Board.
Intervention ConditionFollowing randomization, participants in the PrEPTECH arm received online education about PrEP and were then directed to order a free home testing kit that allowed for rectal swab and dried blood spot testing for serum creatinine, hepatitis B, HIV, syphilis, and rectal chlamydia and gonorrhea. When laboratory test results became available, participants were prompted to complete a medical intake questionnaire on the PrEPTECH platform. If the study clinician [J.D.K.] deemed PrEP was indicated and safe for that participant on review of laboratory test results and intake responses, he issued a prescription for Truvada [emtricitabine/tenofovir disoproxil fumarate], written for a 6-month supply to provide maximally patient-centered, convenient care, lowering burdens of renewal and shipping, and a free initial supply was mailed by an online pharmacy. Thirty days after the prescription was sent, participants were invited to report side effects or challenges encountered in taking PrEP through a medical questionnaire. Ninety days post enrollment, participants could complete a second home specimen collection and testing kit with the same tests as before excluding creatinine and hepatitis B and a third medical intake questionnaire for review by the study clinician. Participants could also create custom text and email-based adherence reminders on the intervention website.
The free initial supply of PrEP included 30 doses for adult men who have sex with men (MSM). Transgender women (TW) enrolled in the study received a 6-month supply of free Truvada in 2 shipments because this subgroup had not been included in the pilot study of PrEPTECH, so providing greater support with PrEP uptake for them was desired. To help participants continue to receive PrEP beyond their initial supply, an interactive portal on the PrEPTECH page outlined their options for obtaining continued medication, depending on their insurance status and other characteristics, with detailed guidance. Preferences gathered through this interface were shared with the study team, allowing team members to offer appropriate assistance, including applying for benefits through Ready, Set, PrEP, a US federal government patient access program, if requested.
Control ConditionControl participants were provided with an online list of resources on PrEP, including links to webpages with sound information on PrEP, information on how to locate a PrEP provider in their community or through telehealth, and specific contact information for community-based organizations that were study partners and equipped to provide PrEP or patient navigation.
Follow-Up and Assessment of PrEP UptakeInvitations to take follow-up surveys on the PrEPTECH website were sent through SMS and email 90 and 180 days after their baseline survey was completed, with automatic reminders following 1, 3, 5, 7, 9, and 12 days after the initial invitation with further follow-up by a study follow-up specialist as needed.
Outcome MeasuresThe predetermined primary outcome for this study was PrEP initiation at 3 months post enrollment, assessed using participant self-report of having taken at least 1 dose of PrEP medication between study enrollment and the three-month survey administration. Other outcomes assessed in this study, also identified in advance, included PrEP initiation by 6 months post enrollment, recent PrEP use at 6 months post enrollment (meaning any use within 90 days of the third survey administration), PrEP prescription receipt, PrEP adherence, and PrEP unprotected intercourse. PrEP initiation at 6 months post enrollment was assessed using self-report of having taken at least 1 dose of PrEP medication at any point during the intervention period. Recent PrEP use at 6 months post enrollment was operationalized as the self-report of past 90-day PrEP use on the final survey.
PrEP adherence was assessed by self-report of the number of doses of PrEP taken in the past 30 days (excluding participants taking event-based or injectable PrEP because adherence would need to be conceptualized differently for those approaches to PrEP administration) and through a 4-level categorical variable based on the participant's assessment of how many of the last 4 weeks they took at least 4 doses of PrEP with the options “all the last 4 weeks (4 of 4 weeks),” “most of the last 4 weeks (3 of 4 weeks),” “half of the last 4 weeks (2 of 4 weeks),” “few of the last 4 weeks (1 of 4 weeks),” and “none of the last 4 weeks (0 of 4 weeks).” PrEP unprotected intercourse, the count of the number of acts of vaginal or anal intercourse the participant reports in which they were not protected by some form of PrEP, is an adaptation of another measure, sex-related PrEP adherence (the proportion of all sex events that were covered by PrEP use).35 It was calculated with a series of questions designed to determine the number of instances in the past 30 days of vaginal or anal sex in which there was no protection from event-driven PrEP (defined as taking PrEP between 2 and 24 hours before the sex act(s) and 2 or more doses 24 and 48 hours after the first dose), continuous PrEP (defined as taking a minimum of 4 doses of PrEP within a week of the sex act(s)), or long-acting PrEP (defined as having taken injectable PrEP within 2 months before sex act(s)). Further information about study measures has been previously published.36
AnalysesThe primary analysis compared the proportions among those who reported PrEP uptake at 3 months post baseline in those randomized to receive PrEPTECH versus the control arm using logistic regression. Secondary analyses examined PrEP uptake by 6 months and PrEP prescription with logistic regression, while PrEP coverage and 2 measures of PrEP adherence were assessed by linear regression. Covariates included in all models on an a priori basis were the baseline value of the outcome and participants' age at baseline. Covariates screened for all models were gender, highest level of education completed, health insurance status, location, language spoken at home (English only or not), gender of sex partners, recent STI diagnosis, and race/ethnicity. A potential covariate was included in the model if the variable was associated with the condition indicator at P < 0.15 and the variable was associated with the outcome at P < 0.15 in individual bivariate analyses. Baseline equivalence between the intervention and control arms of the study for key demographic and behavioral characteristics was assessed using independent sample T tests. Differential and overall attrition were assessed using the What Works Clearinghouse–recommended approach.37 Complete case analysis was used. Analyses were completed using SPSS version 29.
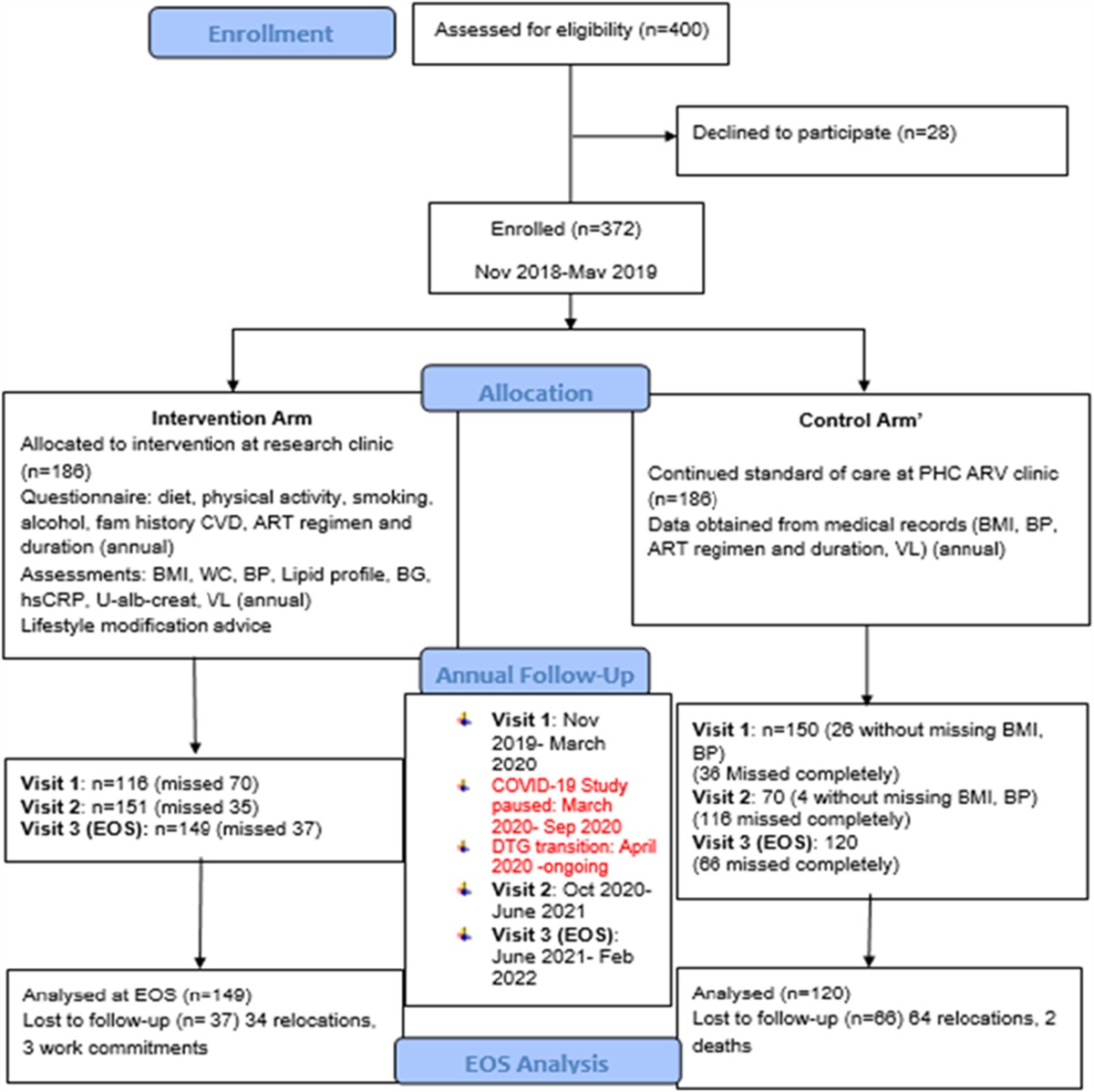
RESULTS Study Participants and Differences Between ArmsFigure 1 describes the study flow. From February through September 2022, 229 MSM and TW were recruited and randomized following completion of the baseline survey, with 116 assigned to the intervention arm and 113 assigned to the control arm. Of these participants, 184 completed the 90-day survey. There was differential loss to follow-up by study arm at the 90-day survey: 98 (86.7%) of the control arm participants and 86 (74.1%) of the PrEPTECH arm participants completed at least 75% of that instrument. Response rates remained higher among control arm participants at 180 days, but not significantly so: 96 (85.0%) of the control arm participants and 89 (76.7%) of the PrEPTECH arm participants completed at least 75% of the final survey.
 FIGURE 1.:
FIGURE 1.: Flow diagram of PrEPTECH screening, enrollment, and study participation (analytic sample).
The characteristics of the study sample are summarized in Table 1. The sample was racially diverse, with 77.3% identifying as non-White, and 57.2% of the participants resided in a household where a language other than English was spoken. Demographic and other baseline characteristics of the study participants were equivalent by arm except for the highest level of schooling completed, with control arm participants showing higher levels of education.
TABLE 1. - Baseline Sociodemographic and Behavioral Characteristics Among Study Participants (Full Sample) Characteristics All Participants (%, n = 229) Intervention (%, n = 116) Control (%, n = 113) P Age (yr), mean ± SD 23.7 ± 2.8 23.6 ± 2.8 23.8 ± 2.8 0.427 Highest level of schooling completed Less than high school 9 (3.9) 5 (4.4) 4 (3.6) 0.004 Graduated high school/GED 25 (10.9) 14 (12.4) 11 (9.9) Some college/technical school 108 (47.2) 65 (57.5) 43 (38.7) Bachelor's degree 71 (31) 28 (24.8) 43 (38.7) Graduate degree 11 (4.8) 1 (0.9) 10 (9.0) Gender identity Cisgender male 209 (91.3) 104 (89.7) 105 (92.9) 0.484 Transgender female 20 (8.7) 12 (10.3) 8 (7.1) Sexual orientation Gay (or gay/queer) 159 (69.4) 79 (69.3) 80 (70.8) 0.766 Bisexual (or bisexual/queer) 44 (19.2) 23 (21.1) 20 (17.7) Other 24 (10.5) 11 (9.6) 13 (11.5) Region Broward county 15 (6.6) 7 (6.0) 8 (7.1) 0.373 Miami-Dade County 29 (12.7) 11 (29.3) 18 (15.9) San Francisco Bay Area 59 (25.8) 34 (22.1) 25 (22.1) Los Angeles County 126 (55) 64 (55.2) 62 (54.9) Race/ethnicity White 52 (22.7) 25 (21.7) 27 (23.9) 0.886 Black/African American 15 (6.6) 9 (7.8) 6 (5.3) Hispanic/Latinx 85 (37.1) 43 (37.4) 42 (37.2) Middle Eastern/North African 3 (1.3) 1 (0.9) 2 (1.8) Asian/Pacific Islander 29 (12.7) 16 (13.9) 13 (11.5) Multiracial 43 (18.8) 21 (18.3) 22 (19.5) Language other than English spoken at home 121 (57.2) 68 (58.6) 63 (55.8) 0.690 Health insurance status Public insurance 54 (24.9) 27 (25.2) 27 (24.5) 0.340 Private insurance through parent 53 (24.4) 23 (21.5) 30 (27.3) Other private insurance (through school, work, affordable care Act marketplace) 63 (29) 29 (27.1) 34 (30.9) Uninsured 27 (12.4) 14 (13.1) 13 (11.8) Other status 20 (9.2) 14 (13.1) 6 (5.5) Lives with parent or guardian 100 (44.8) 54 (47.8) 46 (41.8) 0.420 Previously took PrEP 50 (21.8) 24 (20.7) 26 (23) 0.750 Number of sex partners, lifetime, mean ± SD 42 ± 107 54 ± 146 31 ± 39 0.121 Diagnosed with an STI, past 6 mo 198 (86.5) 99 (85.3) 99 (87.6) 0.701In the logistic regression model, participants were significantly more likely to have reported PrEP uptake at 90 days post baseline (OR: 6.6, 95% CI: 2.5 to 17.3, P < 0.001; Table 2). On completion of the 90-day postbaseline survey, 64.2% of those in the PrEPTECH arm had taken PrEP since study start versus 27.3% of those in the control arm.
TABLE 2. - Likelihood of PrEP Uptake and Prescription Receipt by 90 and 180 Days of Study Enrollment and Persistent Use of PrEP at Both 90 Days and 180 Days Post Baseline, Intervention vs. Control OR* 95% CI P PrEP initiation By 90 days post baseline* 6.63 2.53 to 17.35 <0.001 By 180 days post baseline† 8.04 2.95 to 21.90 <0.001 PrEP use, past 90 d At 180 days post baseline† 2.81 0.48 to 16.31 0.25 PrEP prescription receipt By 90 days post baseline‡ 6.45 2.76 to 15.07 <0.001 By 180 days post baseline§ 5.01 2.22 to 11.29 <0.001*Covariates included in the model: number of sex partners, insurance status.
†Covariates included in the model: number of sex partners, residing with parents, and location.
‡Covariates included in the model: history of PrEP use, number of sex partners, and insurance status.
§Covariates included in the model: number of sex partners, location, history of PrEP use, and highest level of education completed.
By 180 days post baseline, the difference in reported PrEP initiation between PrEPTECH and control arm participants remained significant. By this point, 75.4% of those in the PrEPTECH arm had taken PrEP since study start versus 36% of those in the control arm. In the logistic regression model, PrEPTECH participants were significantly more likely to have reported PrEP uptake at any point over the course of the study by 180 days (OR: 8.0, 95% CI: 2.9 to 21.9, P < 0.001). However, though PrEP use within the last 3 months at 180 days post enrollment was greater in the PrEPTECH arm (73.2% in the PrEPTECH arm versus 35.1% in the control arm), that difference did not reach statistical significance in the logistic regression model (OR: 2.8, 95% CI: 0.5 to 16.3, P = 0.25).
PrEP prescription receipt was also significantly higher at 90 days and 180 days post baseline in the logistic regression model. At 90 days, 68.4% of PrEPTECH participants and 36.5% of control arm participants had received a PrEP prescription (OR: 6.5, 95% CI: 2.8 to 15.1, P < 0.001); at 180 days, 76.5% and 48.4% of PrEPTECH and control arm participants, respectively, had obtained a prescription for PrEP (OR: 5.0, 95% CI: 2.2 to 11.3, P < 0.001).
PrEP Adherence Among Users of Continuous PrEPPast 30-day self-reported adherence among those on continuous PrEP was not significantly different between study arms assessed either as a categorical variable or continuous variable (Table 3). At 90 days, mean adherence was 20.3 days (SD = 10.8) and 16.8 days (SD = 12.3) among the control and intervention arms, respectively (P = 0.17), while at 180 days, the past 30-day adherence was 19.7 days (SD = 10.0) and 17.8 days (SD= 11.7) among the control and intervention arms, respectively (P = 0.42).
TABLE 3. - PrEP Adherence (Categorical and Continuous) and Coverage at Both 90 and 180 Days Post Baseline, Intervention vs. Control, Assessed by Linear Regression Models β (SE) 95% CI P PrEP adherence, categorical 90 days post baseline* −0.169 (0.314) −1.076 to 0.175 0.156 180 days post baseline† 0.088 (0.381) −0.529 to 1.000 0.540 PrEP adherence, continuous 90 days post baseline‡ −0.090 (2.726) −7.586 to 3.278 0.432 180 days post baseline§ −0.010 (2.921) −6.084 to 5.621 0.937 PrEP coverage By 90 days post baseline‖ −0.024 (2.412) −5.394 to 4.155 0.798 By 180 days post baseline¶ −0.075 (2.106) −5.969 to 2.386 0.397*Covariates included in the model: location and age.
†Covariates included in the model: location.
‡Covariates included in the model: previous STI infection and age.
§Covariates included in the model: age and highest level of education completed.
‖Covariates included in the model: gender of sex partners.
¶Covariates included in the model: gender of sex partners and location.
At 90 and 180 days post baseline, control arm participants had more sex acts in the past 90 days that were unprotected by PrEP: At 90 days, 5.2 instances of vaginal or anal sex not protected by PrEP (SD = 10.5) were reported by intervention arm participants and 8.2 by control arm participants (SD = 11.8), and at 180 days post baseline, control participants reported engaging in a mean of 9.4 (SD = 14.6) sex acts not protected by PrEP, while intervention arm participants reported engaging in 4.7 (SD = 8.7) unprotected sex acts. In multiple linear regression analyses, this difference in PrEP coverage was not statistically significant (P = 0.798 at 90 days post baseline and P = 0.397 at 180 days post baseline).
DISCUSSIONThis study confirms that the PrEPTECH telehealth intervention was successful in connecting a racially diverse group of young MSM and TW, in which more than half of participants resided in a household where a non-English language was spoken, to PrEP. Previous studies have shown that PrEP telehealth can provide PrEP to various populations (eg, residents of a primarily rural state16–18 and patients at big city clinics19,21) and that PrEP telehealth is viewed favorably relative to traditional forms of PrEP delivery,14,21,25 but due to their observational study designs, none confirmed the extent to which access to PrEP was attributable to the PrEP telehealth intervention. The success of this randomized controlled study in increasing PrEP uptake suggests telehealth is an important avenue for addressing inequities in PrEP access, a persistent problem in the United States38 and globally.39
Overall, the findings of this study underline how telehealth may augment HIV prevention efforts. There are a plethora of venues now offering PrEP telehealth in the United States, some targeting particular populations or localities and others nationwide.12 Further investment to enhance the awareness of these efforts and their appeal and accessibility to people put at risk of HIV is warranted.
By the same token, this study suggests there are obstacles that may hinder some people seeking PrEP through telehealth. As in some past studies of PrEP telehealth implementation,16,19,21 a sizable minority of intervention arm participants (26.8% in this study) did not access PrEP throughout the course of the study. While past research found PrEP telehealth care is favored for its convenience and efficiency, those benefits may come with costs: overcoming competing priorities, loss of provider–patient rapport, obstacles for those lacking technological skills or access, and hurdles related to independently completing laboratory testing (such as dislike of needles and difficulty collecting a proper sample for dried blood spot testing).40 Future work should explore participant experiences and identify facilitators and barriers to PrEP access among study participants. The rate of PrEP uptake reported here suggests that while telehealth for PrEP is an important tool, more work could be conducted to increase acceptance and utilization. Community-based PrEP services may better serve certain people in need of PrEP (eg, those without a stable address or consistent internet access). Expanding the options for obtaining PrEP and partnerships between telehealth and community health care providers may help people find avenues for PrEP care that best meet their needs. Stimulating demand for PrEP will also be important because no amount of convenience will entice people to use PrEP if there is no interest in it.
This study also draws attention to the complications of attaining optimal PrEP adherence and persistence of use. By 180 days, PrEP use in the study arms had begun to converge, though remaining higher in the PrEPTECH arm. This is likely reflective of the intervention design, which moved participants toward receipt of PrEP at the outset but did not have strong mechanisms for advancing intervention arm participants toward PrEP maintenance if they did not engage early in the study. Greater efforts to continue to encourage PrEP use would be warranted, especially considering the high rates of PrEP discontinuation seen in other clinical settings (and particularly among young Black MSM).41
The intervention's lack of effect on adherence may be due to lack of statistical power (because this comparison concerned only the subset of participants in each arm who initiated continuous PrEP) or characteristics of the intervention. The customizable medication reminders made available through PrEPTECH, which were intended to enhance PrEP adherence, were used by only 8 participants. Interventions incorporating daily reminders have shown promise, but effective PrEP adherence interventions have incorporated multiple components alongside daily prompts, such as two-way SMS messaging allowing for personalized interaction, discussion forums, and educational content.42 A multimodal approach is likely needed to maintain optimal PrEP adherence.43
Limitations and StrengthsThere are study limitations worth noting. Restricting enrollment to young MSM and TW in just 4 locales limits the generalizability of our findings beyond those regions and populations. Because we did not recruit any participants aged 15–17 years, we cannot draw any conclusions about how well PrEPTECH would work for that age group. The provision of free services (laboratory testing and a preliminary supply of PrEP) limits generalizability as well. The provision of a starter dose of free PrEP to all in the intervention arm makes it difficult to disentangle the effects of that initial free supply from the effects of the telehealth platform. The reliance of this study on self-report data is another potential limitation because in self-report study, participants may tend to overestimate their PrEP use compared with assessments using medication event monitoring systems or measurement of plasma or blood concentrations,44,45 which were not undertaken due to cost. The lack of participant blinding was another unavoidable limitation to the study design. The differential attrition between study arms at 90 days of follow-up may draw into question the significance of the differences observed at that time point. We theorize that the lower response rate among intervention arm participants may have been due to exhaustion with multiple contacts related to the intervention, which the control arm, naturally, did not experience. The study also featured several strengths, including its priority population of focus, retention rates nearly 80% at both time points, tracking PrEP use over a period of 6 months, attention to significant covariates, and the relevance of PrEP telehealth because the COVID-19 pandemic inspired a boom of interest in telehealth interventions.9
CONCLUSIONSThis study, the first published randomized controlled trial of a PrEP telehealth intervention, confirms that telehealth can provide access to PrEP for critical populations. A streamlined telehealth PrEP care system can be a valuable pathway to PrEP for people facing health inequities and various barriers to PrEP access, but PrEP telehealth may not adequately serve all and would benefit from being coupled with other strategies to support adherence.
ACKNOWLEDGMENTSR.K.E., R.B., and J.D.K. conceived the study, participated in its design and coordination, and helped to draft the manuscript. T.-H.P.D. participated in the coordination of the study. D.-M.T.M. and O.L.S. participated in the design of the study and performed statistical analysis. All authors read and approved the final manuscript. The authors thank our colleagues who supported this study: Colleen Sargent, Karin Coyle, Sarah Han, Nixa Sanchez, Jason Burrage, Ryan Carmody, Angela Cesaro, Laiah Idelson, Jay Lykens, Emma Schlamm, and Bhupendra Sheoran. Most of all, the authors thank the community partners, PrEPTECH Community Advisory Board, and participants in the PrEPTECH study for their critical involvement. Clinical Trials Number: NCT04902820.
REFERENCES 1. Chou R, Evans C, Hoverman A, et al. Preexposure prophylaxis for the prevention of HIV infection: evidence report and systematic review for the US preventive services task force. JAMA. 2019;321:2214–2230. 2. Mayer KH, Molina JM, Thompson MA, et al. Emtricitabine and tenofovir alafenamide vs emtricitabine and tenofovir disoproxil fumarate for HIV pre-exposure prophylaxis (DISCOVER): primary results from a randomised, double-blind, multicentre, active-controlled, phase 3, non-inferiority trial. Lancet. 2020;396:239–254. 3. Liegeon G, Ghosn J. Long-acting injectable cabotegravir for PrEP: a game-changer in HIV prevention? HIV Med. 2023;24:653–663. 4. Antoni G, Tremblay C, Delaugerre C, et al. On-demand pre-exposure prophylaxis with tenofovir disoproxil fumarate plus emtricitabine among men who have sex with men with less frequent sexual intercourse: a post-hoc analysis of the ANRS IPERGAY trial. Lancet HIV. 2020;7:e113–e120. 5. Celum C, Baeten J. PrEP for HIV prevention: evidence, global scale-up, and emerging options. Cell Host Microbe. 2020;27:502–506. 6. Centers for Disease Control and Prevention. Core indicators for monitoring the Ending the HIV epidemic initiative (preliminary data): National HIV Surveillance System data reported through June 2023; and preexposure prophylaxis (PrEP) data reported through March 2023. HIV Surveill Data Tables. 2023;4. https://www.cdc.gov/hiv/library/reports/surveillance-data-tables/vol-4-no-3/index.html. Accessed January 11, 2023. 7. Segal K, Fitch L, Riaz F, et al. The evolution of oral PrEP access: tracking trends in global oral PrEP use over time. J Int Aids Soc. 2021;24:27–28. 8. Tuckson RV, Edmunds M, Hodgkins ML. Telehealth. N Engl J Med. 2017;377:1585–1592. 9. Patel P, Kerzner M, Reed JB, et al. Public health implications of adapting HIV pre-exposure prophylaxis programs for virtual service delivery in the Context of the COVID-19 pandemic: systematic review. JMIR public Health Surveill. 2022;8:e37479. 10. Brawley S, Dinger J, Nguyen C, et al. Impact of COVID-19 related shelter-in-place orders on PrEP access, usage and HIV risk behaviors in the United States [Abstract]. J Int Aids Soc. 2020:178. 11. Touger R, Wood BR. A review of telehealth innovations for HIV pre-exposure prophylaxis (PrEP). Curr Hiv/AIDS Rep. 2019;16:113–119. 12. Dawson L, Frederiksen B, Gomez I. PrEP Access in the United States: The Role of Telehealth [Issue Brief]. Kaiser Family Foundation; 2022. Available at: https://www.kff.org/hivaids/issue-brief/prep-access-in-the-united-states-the-role-of-telehealth. Accessed January 11, 2023. 13. John SA, Rendina HJ, Grov C, et al. Home-based pre-exposure prophylaxis (PrEP) services for gay and bisexual men: an opportunity to address barriers to PrEP uptake and persistence. PLoS One. 2017;12;e0189794. 14. Riba A, Obafemi O, Weise J, et al. P443 transitioning to telehealth PrEP delivery during the COVID-19 pandemic: uptake and patient perceptions [poster]. Sex Transm Infect. 2021;97(suppl 1):A174. 15. Wong KYK, Stafylis C, Klausner JD. Telemedicine: a solution to disparities in human immunodeficiency virus prevention and pre-exposure prophylaxis uptake, and a framework to scalability and equity. Mhealth. 2020;6:21. 16. Hoth A, Shafer C, Dillon D, et al. Iowa TelePrEP: a public-health-partnered telehealth model for human immunodeficiency virus preexposure prophylaxis delivery in a rural state. Sex Transm Dis. 2019;46:507–512. 17. Chasco EE, Shafer C, Dillon DM, et al. Bringing Iowa TelePrEP to scale: a qualitative evaluation. Am J Prev Med. 2021;61:S108–S117. 18. Chasco EE, Hoth AB, Cho H, et al. Mixed-methods evaluation of the incorporation of home specimen self-collection kits for laboratory testing in a telehealth program for HIV pre-exposure prophylaxis. AIDS Behav. 2021;25:2463–2482. 19. Stekler JD, McMahan V, Ballinger L, et al. HIV pre-exposure prophylaxis prescribing through telehealth. J Acquir Immune Defic Syndr. 2018;77:e40–e42. 20. Auchus IC, Jaradeh K, Tang A, et al. Transitioning to telehealth during the COVID-19 pandemic: patient perspectives and attendance at an HIV clinic in San Francisco. AIDS Patient Care STDs. 2021;35:249–254. 21. Player MS, Cooper NA, Perkins S, et al. Evaluation of a telemedicine pilot program for the provision of HIV pre-exposure prophylaxis in the Southeastern United
留言 (0)