EFT has emerged as a new marker of cardiometabolic risk due to its intimate proximity with the myocardium, the coronary arteries, and its endocrine metabolic features [6].
The large visceral fat storage known as EFT is situated around the large coronary arteries and between the epicardium and pericardium. Through the cytokine pathway, this tissue contributes to the development of atherosclerosis and has significant endocrine and paracrine activity [12].
Maternal diabetes modifies the fetal environment, which causes more and earlier fat deposition in the epicardial fat compared to other fat stores [8].
In the current study, we found that IDMs have LV hypertrophy. They also have global myocardial dysfunction in comparison to healthy individuals using two dimensional conventional echocardiography and TDI. These findings are consistent with those reported by Farag et al. [13]. We found that IDM with poorly controlled diabetes has a significantly higher ESPAP in comparison to healthy individuals.
Chronic fetal hyperinsulinemia causes fetal macrosomia and increases the cardiac mass due to a larger mass of myocardial nuclei, an increase in the number of myocardial cells, and hypertrophy of myocardial fibers. There are more insulin receptors in the fetal heart, which makes it easier for protein and fat synthesis regardless of how much glycogen is deposited, which makes IDM more susceptible to HCM and increased LV dimensions [14].
We found that there was a statistically significant difference between study groups as regards EFT, with a higher mean among IDM patients with poorly controlled diabetes. It is followed by IDM with well controlled diabetes, and the lowest level was in healthy control. These findings agree with those of Vela-Huerta et al. [9] who reported the same findings. The altered fetal environment, including hyperinsulinemia and hyperglycemia resulting from maternal diabetes, results in greater and earlier fat deposition in epicardial fat than in other fat stores [8].
In the current study, EFT was positively correlated with neonatal birth weight. Similar to our findings, Jackson et al. [15] reported that in the fetuses of diabetic mothers, EFT correlates directly with both EFW and abdominal circumference. Both of these are previously validated sonographic markers of an adverse fetal response to the diabetic state.
The presence of hyperglycemia, hyperinsulinemia, and inflammatory processes enhances the placental supply of nutrients to the developing fetus, including not only glucose but also amino acids and free fatty acids, thereby exerting an impact on fetal growth, causing macrosomia, and fat deposition in the epicardial space, resulting in higher EFT [16].
Our study also showed that there was a statistically significant positive correlation between EFT and each of the IVSd, IVSs, and ESPAP measurements and a significant negative correlation with the LVIDd and LVIDs measurements. This agrees with the results reported by Vela-Huerta et al. [9].
Hypertrophic cardiomyopathy is a prevalent cardiac anomaly observed in around 40% of pregnancies affected by diabetes. Myocardial hypertrophy is distinguished by the augmentation of both the interventricular septum and ventricular walls [17] caused by an altered fetal environment regarding hyperglycemia and hyperinsulinemia, which are similar mechanisms attributed to higher EFT found in IDM [9].
Our study illustrated that there was a statistically significant positive correlation between EFT, each of IVRT, and Tei of LV. Similar to our findings, Ghandi et al. [18] found that there was a statistically higher incidence of diastolic dysfunction in cases of IDMs than in the healthy control group.
Underdeveloped fetal ventricular compliance and, as a result, diastolic dysfunction because of a thicker cardiac wall occurs in IDMS [19]. Increased epicardial fat mechanically affects LV and RV diastolic filling, causing diastolic dysfunction [11].
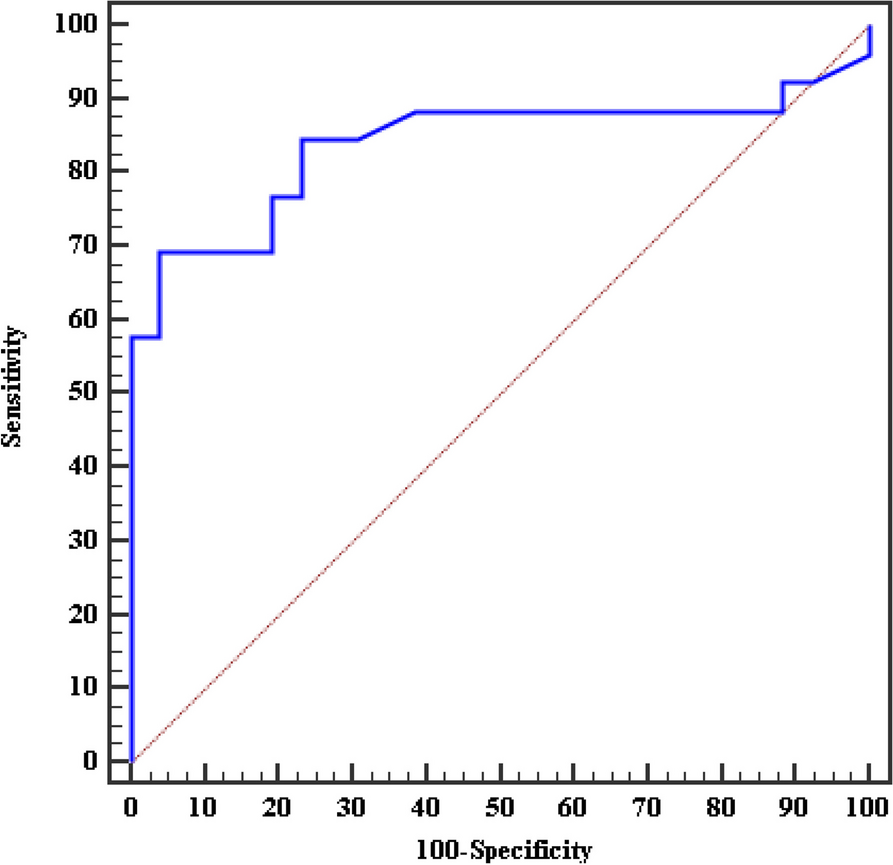
We found that the sensitivity and specificity test for EFT in the detection of cases of diabetic mothers was 100% at a cutoff value of 3.950 mm, and for differentiation between controlled and uncontrolled diabetic mothers, the sensitivity was 66.7% and the specificity was 72.2 at a cutoff value of 5.100 mm.
The main reason for EFT to be a reliable marker is that it is not affected by changes in subcutaneous and muscle tissues [20]. The altered fetal environment, including hyperinsulinemia and hyperglycemia resulting from maternal diabetes, results in greater and earlier fat deposition in epicardial fat than in other fat stores [8].
The limitations of the present study were the need for further studies with larger number of patients, and the need for long-term follow-up period to understand the etiology and clinical implications of the echocardiographic findings.



留言 (0)