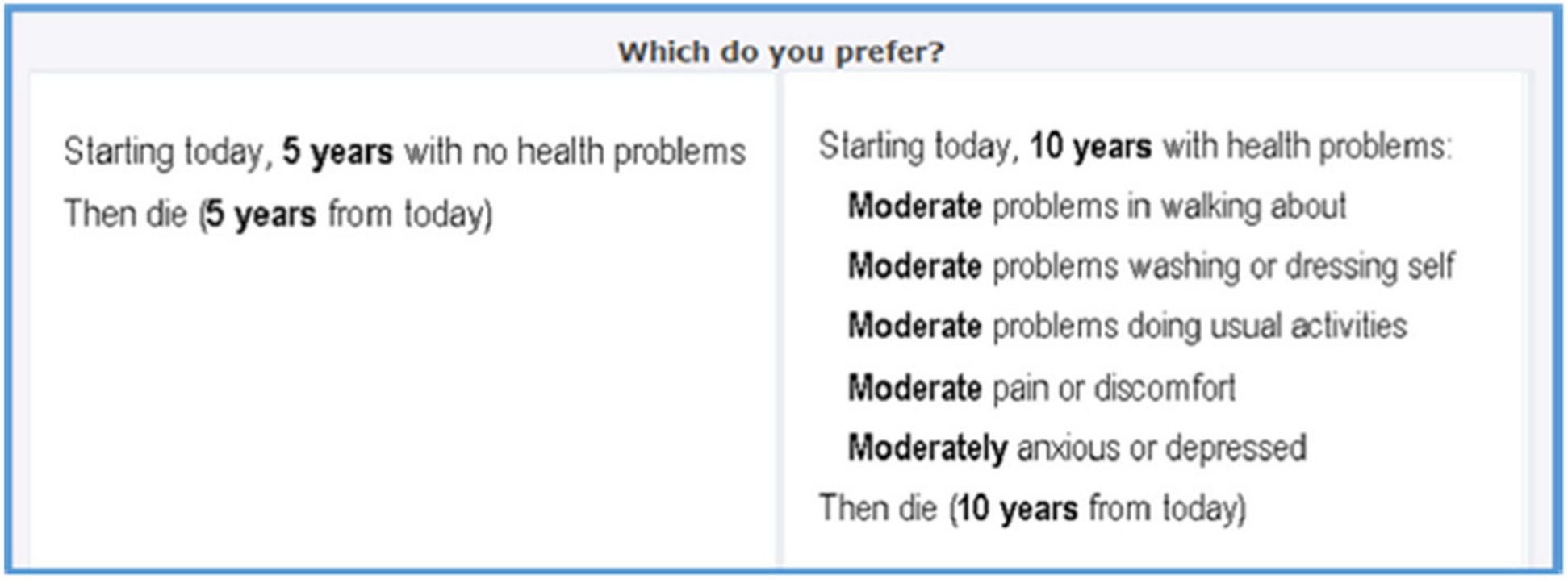
Data on the HRQoL of transplant recipients with R/R CMV are limited. To the best of our knowledge, this is the first study that aimed to determine HSUVs for transplant recipients with R/R CMV to evaluate the impact of R/R CMV on patients’ HRQoL. Vignettes describing the symptoms, conventional anti-CMV treatments, and effects of R/R CMV across various severity levels, transplant types, and transplant complications were developed. Each vignette was evaluated by respondents from the general population in the UK using the composite TTO method. The TTO preference elicitation method is widely used to determine utility values of health outcomes or health states to inform economic evaluations [16].
Overall, the results from this study demonstrated that as the severity of the health states increased, the mean HSUVs reduced. The highest mean utility value was observed for non-CS CMV, while the lowest utility value was observed for CS-symptomatic CMV with lung GL. Lower utility values were also observed for combination health states compared with non-combination health states (i.e., a lower utility value was observed for CS-symptomatic CMV with GvHD than for CS-symptomatic CMV). This finding indicates that GvHD and graft loss can have a substantial impact on the HRQoL of patients with R/R CMV post-transplant.
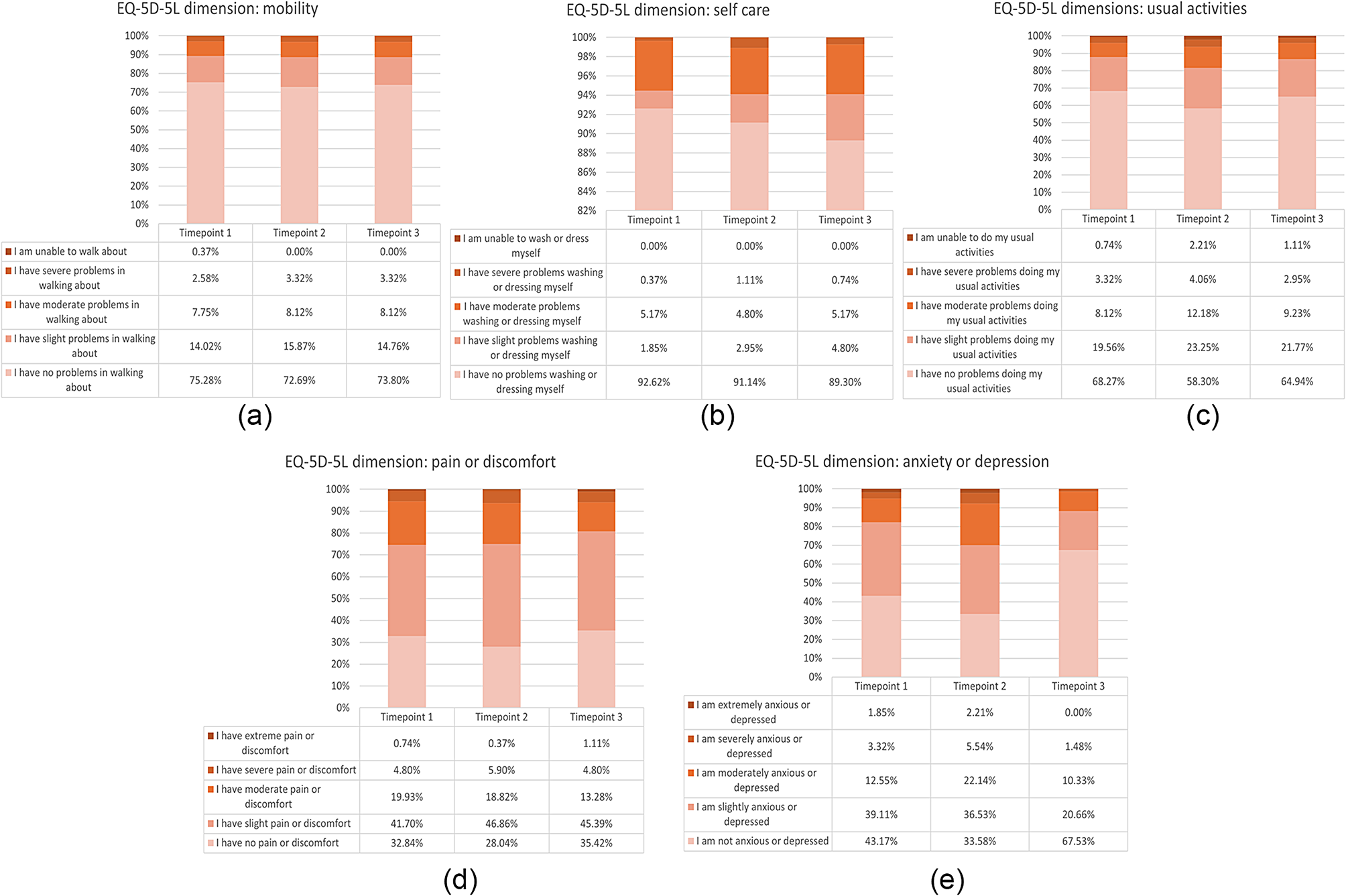
The mean utility values for the most severe health state (CS-symptomatic CMV with lung GL) and the least severe health state (non-CS CMV) were compared with the UK EQ-5D-3L tariff [29] to contextualize the disease-specific utilities estimated for the vignettes in this study with generic utility values. CS-symptomatic CMV with lung GL had a HSUV of 0.289 which was similar to that of the 21322 EQ-5D-3L health state (0.293) [29]. This EQ-5D-3L health state suggests some problems with mobility, no problems with self-care, inability to perform usual activities, moderate pain or discomfort, and moderate anxiety or depression. Non-CS CMV had a HSUV of 0.815, similar to the utility value of the 21211 EQ-5D-3L health state (0.814). This EQ-5D-3L health state indicates some problems with mobility, no problems with self-care, some problems performing usual activities, no pain or discomfort, and no anxiety or depression. These comparisons suggest that for our study, patients would experience utility equivalent to moderate or severe problems in at least three health dimensions measured by the EQ-5D-3L.
In addition, when clinical health states were kept constant, GvHD was valued less severely than both kidney GL and lung GL, and lung GL was valued more severely than kidney GL. Thus, the extent of the impact of R/R CMV and subsequent organ loss on post-SOT HRQoL was dependent on the type of SOT received.
The background characteristics that had a statistically significant impact on the variance of health state utility values were gender, age, education level, and survey completion time. However, it should be noted that the R2 values were low for each health state, which suggests that these covariates are only accounting for a small proportion of variation in utility values. Therefore, it is likely that other unobserved factors influenced utility valuation. The associations of age and survey completion time on variance in health state utility values are consistent with those found in previous studies using TTOs [30]. Although a statistically significant impact of education level on health state utility values was observed, the absolute differences were marginal. Other studies have mixed findings on the association of education level with health state utility values [31, 32].
Strengths of this study include the use of multiple sources of evidence to inform the development of the vignettes, including relevant data from the existing literature and qualitative interviews with healthcare professionals experienced in treating patients with post-transplant R/R CMV. This ensured that the final vignettes accurately represented the experience of patients with post-transplant R/R CMV. The use of multiple evidence sources is also consistent with recommendations on the generation of HRQoL data outlined in a recent NICE consultation document [13]. Furthermore, the study included a large sample size that was representative of the UK general public in terms of age and sex for the online TTO survey, which is the recommended approach of valuation by NICE [33]. The application of robust quality control criteria ensured that the final set of utility data were of a high quality.
The study should, however, be considered in light of the limitation that an online, self-completion valuation approach was used rather than conducting face-to-face interviews. The decision to use this approach was driven by the impact of social restrictions caused by the COVID-19 pandemic and a desire to minimize risk of infection to participants due to COVID-19. Face-to-face interviews are the favored mode of administration for preference elicitation surveys using the TTO method. Previous studies have compared face-to-face interviewer-assisted TTO surveys with online unassisted interviews and found the data quality to be poorer in unassisted interviews [34,35,36]. Whilst these studies compared identical protocols based on a standard face-to-face format, our study included additional elements to inform respondents, such as an instructional video explaining the TTO process and a practice TTO task that the respondents had to complete before moving on to the main survey. Data quality was evaluated using several quality checks. A relatively high proportion of responses were excluded following the quality checks, which may be due to the choice of mode of administration, however, the sample size for analysis was still sufficient for the analysis (n = 738) and the analysis population is broadly representative of the UK general population for age and gender [27]. The demographic data collected in this study was limited to sex, age, education, and current health to minimize the cognitive burden on respondents since the TTO task was cognitively demanding.


留言 (0)