The increasing incidence of colorectal cancer worldwide has highlighted the need to develop and assess diagnostic technologies that are effective and represent ‘value for money’ [5]. For findings to be dependable and comprehensive, analyses need to take into account all relevant diagnostic and therapeutic components and their impact, including the effect of undergoing an invasive examination. Failing to do so effectively implies that, in economic evaluations, a colonoscopy is considered no less unpleasant than any other approach, as well as that, practically, there is no additional benefit in developing less invasive diagnostic methods. Most people with lower bowel symptoms do not have serious bowel disease [5], but if they all have colonoscopy and some associated ‘disutility’, the cumulative disutility across the population will be considerable.
It is well known that undergoing a colonoscopy examination is unpleasant, but, to the best of our knowledge, there is a lack of empirical estimates of the decrement in preference-based HRQoL that can be used in economic analyses. To quantify the effect of the procedure, we collected data at three points in time: (i) T1: before the colonoscopy, to capture a patient’s health status prior to the procedure; (ii) T2: during bowel preparation, to capture a component of the procedure that patients find to be particularly unpleasant; and, (iii) T3: shortly after colonoscopy, to capture HRQoL after the procedure. For this, we used the EQ-5D-5 L, a multi-attribute instrument that enables the calculation of utility values and, by extension, QALYs. We provide granular estimates of utility values for different patient characteristics (including sex, age group, ethnicity, BMI etc.), gastrointestinal symptoms and diagnosis.
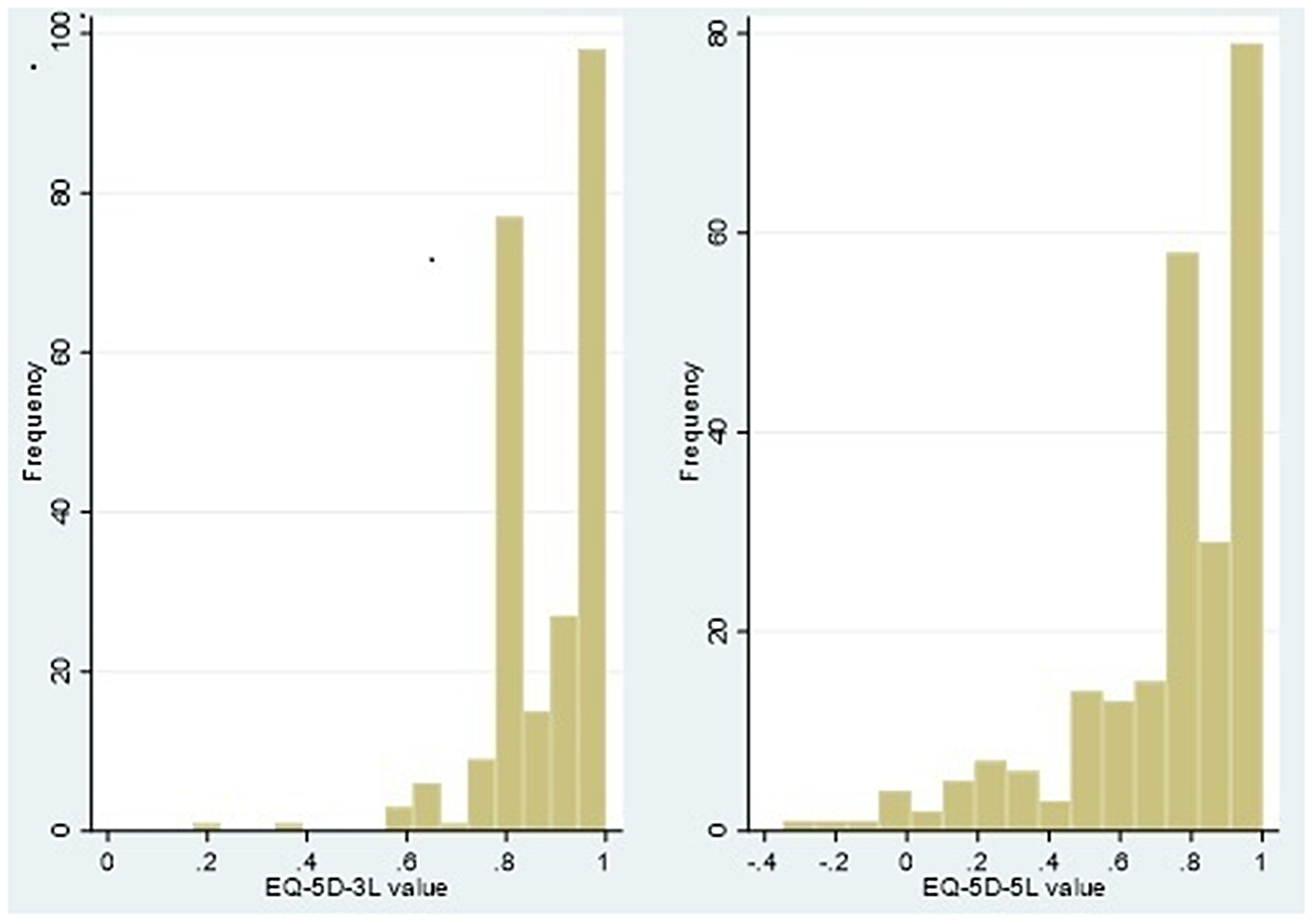
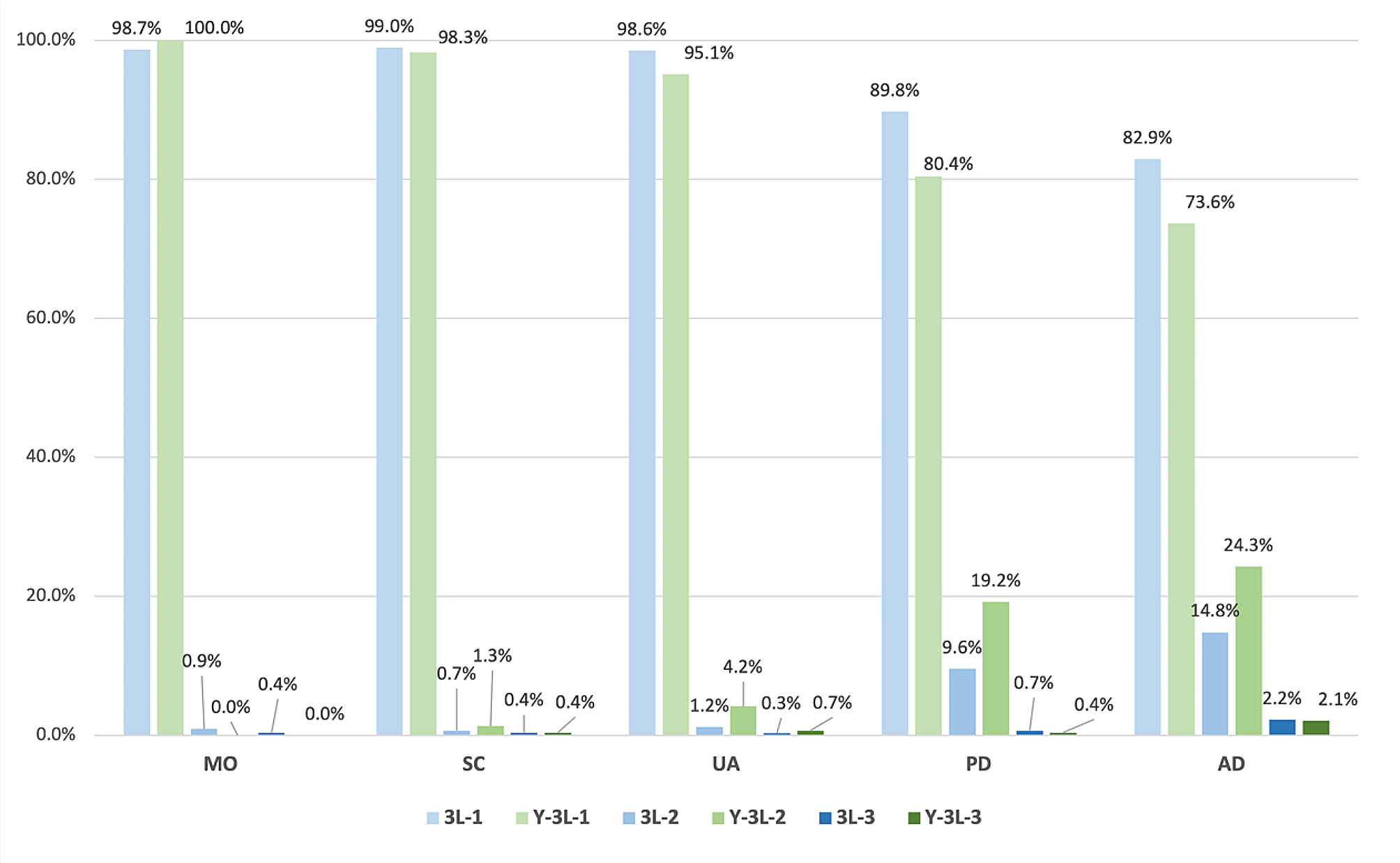
Despite respondents presenting with gastrointestinal symptoms, the commonest response to the EQ-5D-5 L was ‘no problems’ in all dimensions (11111). At T1, the mean EQ-5D-5L value across all respondents was 0.76 (SD: 0.21), with males reporting higher values than female respondents (0.82 vs 0.71 respectively, p-value < 0.001). These values, and the fact that on average, males tend to report higher EQ-5D-5L values, are comparable to observations in the general population in England [17]. At T2, there was a notable drop in the mean EQ-5D value across all participants (-0.33, p-value < 0.001), in line with the greater number of participants reporting higher levels of anxiety. This reduction was prominent amongst females, White British and people classified as obese. At T3, after colonoscopy, there was a notable and statistically significant rebound in HRQoL compared to the previous assessment point, with the mean EQ-5D score across all patients ending up exceeding the score at baseline.
Findings were broadly in line with intuition and previous evidence. Patients with symptoms suggesting a bowel condition were anticipated to be experiencing some problems with pain/discomfort and anxiety prior to diagnosis and treatment initiation. Similarly, it is expected that pain and anxiety would have intensified on the day before the scheduled colonoscopy examination, while undergoing bowel preparation in anticipation of a hospital appointment for an invasive procedure [4]. After the procedure, at T3, EQ-5D-5 L values had rebounded and exceeded those of T2, with more patients reporting no problems with pain/discomfort or anxiety/depression than at T2. It is likely that this is due to the discomfort associated with the preparation and procedure subsiding, and it is also possible that, by this time, the anxiety associated with the prospect of undergoing an invasive procedure is allayed.
To our knowledge, our study is unique in measuring the effect of a colonoscopy using a generic multi-attribute instrument and presenting findings in terms of preference-based HRQoL (utility). Previous studies aiming to explore the impact of colonoscopy on HRQoL have done so by using instruments that do not allow the derivation of utility values [4, 18, 19], a necessary component for the calculation of QALYs in cost-utility analyses. An exception is a recent study by Bulamu et al. [20], where EQ-5D-5 L was used in addition to the cancer-specific EORTC Quality of Life Utility Measure-Core 10 dimensions (QLU-C10D). However, the aims of these study were different—to assess the sensitivity and discriminant validity of two instruments—and responses were sought well after colonoscopy had taken place (median times 38 days and 423 days after colonoscopy, for first and second assessment, respectively), rather than shortly before, during and shortly after the procedure.
Our study has certain limitations which warrant careful interpretation of its findings. First, the population of study participants presented little ethnic diversity: nearly 92% of the participants identified as White British. This is in line with the broader sample of all RECEDE participants, where 1809 out of 1978 patients (91.4%) identified as White British and reflects findings that, in the UK, ethnic minorities are more likely to be diagnosed as emergencies, rather than through the two-week-wait pathway. Given this, it may be reasonable to consider EQ-5D-5 L values derived in this study to be largely applicable to a White British population, though there is no obvious reason why responses of participants of other ethnicities might be systematically different, especially when it comes to dimensions of interest in the EQ-5D-5 L such as mobility, self-care, usual activities, pain/discomfort, anxiety/depression. Secondly, findings reported here are based on a complete-case analysis; participants with incomplete data (most commonly not having returned a complete EQ-5D-5 L questionnaire at a single assessment point) were, pragmatically, excluded from the analysis. Methods are available to impute missing data and, while these can increase the number of responses, they require ascertaining the mechanism that caused missingness and add an additional level of uncertainty [21]. Thirdly, the degree to which a generic HRQoL such as the EQ-5D-5 L is sensitive enough to capture the effect of a procedure on HRQoL is debatable. While, it is expected that condition-specific instruments might be better at detecting changes in this population [20], measures derived from non-preference-based HRQoL scales are not appropriate for use in economic evaluations [10], thus a balance needs to be struck between sensitivity and useability. Last, it can be argued that the most accurate indication of the HRQoL decrement due to undergoing a colonoscopy would be obtained by participants completing the EQ-5D-5 L while they are physically undergoing the examination. As this is, for obvious reasons, not advisable, the thirds assessment took place after the procedure (within 24 h). It is likely that, at the end of the procedure, patients are given an (informal) indication of the colonoscopy findings, thus it is possible that a drop in anxiety levels at T3 is, at least partially, due to participants receiving reassurance that SBD was not identified. Nonetheless, looking across patients who were and were not diagnosed with SBD showed EQ-5D-5 L scores to follow a similar, increasing trajectory between T2 and T3, though this increase was not statistically significant in patients diagnosed with SBD (p = 0.623).

留言 (0)