
記住我


The world is experiencing an aging population. Currently, there are over 703 million people worldwide aged over 65 years of age, projected to reach 1.5 billion by 2050.1 Advances in anesthetic and surgical techniques have allowed elderly and potentially frail patients to undergo neurosurgical procedures that might otherwise have been too risky. As a result, neuroanesthesiologists are increasingly likely to encounter frail patients in their daily practice and need to understand the impact of frailty on postoperative outcomes to offer optimal clinical care to this complex surgical population.2
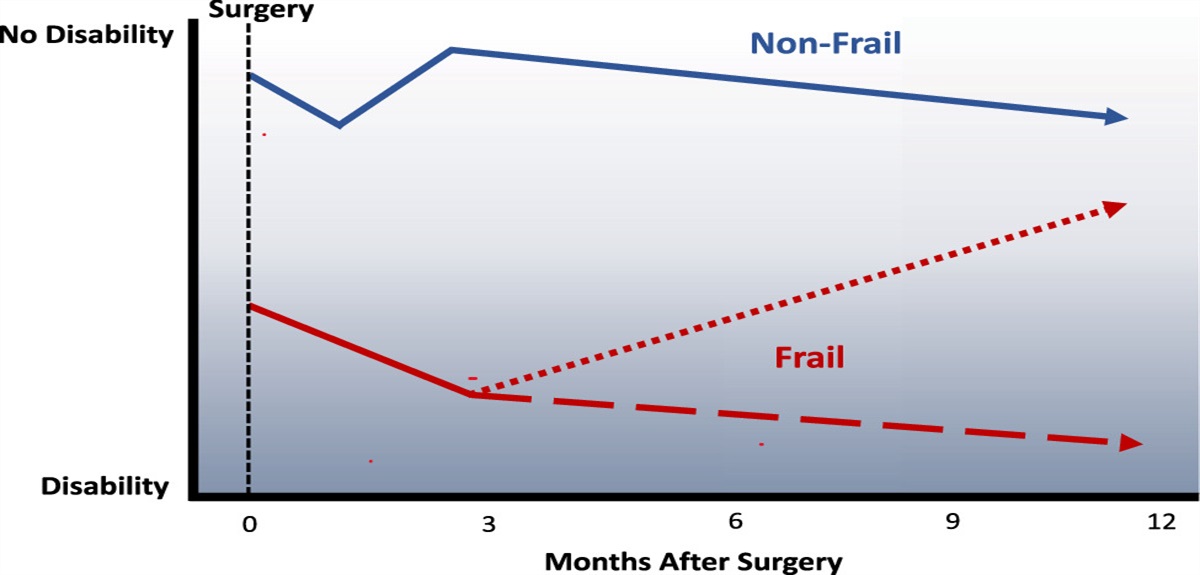
Frailty is a complex and multidimensional concept first defined by Fried et al3 in 2001 as an age-related syndrome of physiological decline. Frailty is a marker of fragility and is characterized by diminished physiological reserve and vulnerability to adverse health outcomes in general. For the frail patient, even a minor change in health status, let alone a major neurosurgical procedure, may result in an inability to return to their prestress or presurgery baseline function. Therefore, a frail elderly person with exhausted physiological and neurological reserve is much more likely to have debilitating effects after surgery, with a reduced probability of recovering their independence (Fig. 1).
 FIGURE 1: Simplified trajectory of recovery for frail and non-frail patients after surgical procedures. Frail patients (red line) have greater disability at baseline than non-frail patients (blue line), and a greater risk of experiencing complications and increases in disability in the first 3 months after surgery. However, after 12 months, the majority of patients with frailty experience improvement in disability from baseline status (red dotted line), unlike non-frail patients. Importantly, a minority of frail patients experienced a progressive increase in disability over the year after surgery (red dashed line). Adapted and modified from the results of McIsaac et al, 2020.4 Adaptations are themselves works protected by copyright. So in order to publish this adaptation, authorization must be obtained both from the owner of the copyright in the original work and from the owner of the copyright in the translation or adaptation.
FIGURE 1: Simplified trajectory of recovery for frail and non-frail patients after surgical procedures. Frail patients (red line) have greater disability at baseline than non-frail patients (blue line), and a greater risk of experiencing complications and increases in disability in the first 3 months after surgery. However, after 12 months, the majority of patients with frailty experience improvement in disability from baseline status (red dotted line), unlike non-frail patients. Importantly, a minority of frail patients experienced a progressive increase in disability over the year after surgery (red dashed line). Adapted and modified from the results of McIsaac et al, 2020.4 Adaptations are themselves works protected by copyright. So in order to publish this adaptation, authorization must be obtained both from the owner of the copyright in the original work and from the owner of the copyright in the translation or adaptation.This review summarizes the tools available to measure frailty in the neurosurgical population and the prevalence of frailty in both spine and intracranial surgical cohorts. Current evidence on the relationship of frailty with postoperative outcomes, and interventions to improve outcomes, will also be discussed. Finally, areas to focus future research are outlined.
MEASUREMENT OF FRAILTY IN NEUROSURGICAL PATIENTSDespite its widely accepted definition, frailty is measured and screened using a variety of measurement tools in both clinical practice and research. The 2 main models of frailty are the deficit accumulation and phenotypic approaches. The deficit accumulation approach postulates that health deficits accumulate as people age and that greater deficits confer greater risk.5 Therefore, frailty results from the accumulation of these deficits and may be disproportionate to age. In contrast, the frailty phenotype proposes that comorbidity is an etiological risk factor for frailty, and disability results from frailty, although frailty is not synonymous with either of these.3 This distinct clinical frailty syndrome, which has been validated to predict patient outcomes, includes weakness, slowness, low levels of physical activity, exhaustion, and weight loss.3
Frailty measurement tools, including those with specific application to neurosurgical populations, are summarized in Table 1. Each tool has distinct advantages and disadvantages, and not all have been specifically validated for use in neurosurgical populations. The modified Frailty Index (mFI)7 and the 5-factor mFI (mFI-5)8 are simplified versions of the Frailty Index (FI) commonly used in administrative or large databases, similar to the Risk Analysis Index.9 The Clinical Frailty Scale6 has been recommended for surgical populations given its ease of use, practical nature, and excellent predictive ability.12 Frailty tools that have been validated for specific spine pathologies include the “Adult Spinal Deformity FI”11 and the “Metastatic Spinal Tumor FI.”10 In contrast, no specific validated frailty tools for surgical patients with intracranial pathology were identified in the current literature.
TABLE 1 - The Advantages and Disadvantages of the Most Common Frailty Measurement Tools, Including Those With Specific Application to Neurosurgical Populations Frailty tool Description Advantages Disadvantages General assessment tools Clinical Frailty Scale (CFS)6 Categorizes an individual using descriptors and pictograms to assess the level of vulnerability, with a range from 1 (very fit) to 9 (terminally ill) • Good predictive capacity for adverse health effects and postoperative outcomesASD indicates adult spinal deformity; CSHA, Canadian Study of Health and Ageing; FI, Frailty Index; 5i-mFI, 5-item modified Frailty Index; mFI, modified Frailty Index; MST, metastatic spinal tumor; NSQIP, National Surgical Quality Improvement Program; RAI, Risk Analysis Index; RAI-A, Administrative Risk Analysis Index; RAI-C, Clinical Risk Analysis Index.
Many neurosurgical pathologies are seen more frequently in older patients, bringing associated frailty to elderly surgical populations. Examples include benign and malignant intracranial neoplasms, falls causing head injury and intracranial bleeding, spinal fractures secondary to reduced bone density, and degenerative spine disease.13 Frailty is increasing in the overall surgical population, with a 30% prevalence in nononcologic surgery in older adults and higher in patients with cancer.14
Frailty prevalence varies depending on the neurosurgical population surveyed, likely due to the use of different frailty assessment tools, as well as population differences, including age distribution. In a recent systematic review, 20% to 40% of metastatic spinal tumor patients, 12% to 56% of adult spine deformity patients, and 10% to 83% of degenerative spine disease patients were frail.15 In patients with brain tumors, the prevalence of frailty also varied widely, with a 5% to 15% prevalence in patients over 65 years of age,16 and up to 57% in patients over 80 years of age.17 In another systematic review, frailty also varied by tumor subtype; the lowest prevalence was observed in pituitary tumor resection (1.5%), rising to 8.2% for other intracranial tumors excluding pituitary, and to as high as 55% for intracranial meningiomas.18 Finally, a recent systematic review found that ~30% of patients with aneurysmal subarachnoid hemorrhage (SAH) were frail.19
RELATIONSHIP BETWEEN FRAILTY AND POSTOPERATIVE OUTCOMESThe importance of understanding the relationship between frailty and postoperative outcomes has been a focus in the recent literature. Previous studies have consistently shown that frailty in patients undergoing intracranial neurosurgery and spine surgery is associated with poor outcomes,15,18 including higher mortality, complication and reoperation rates, longer hospital length of stay, non–home discharge disposition, readmission rates, and overall costs. Interestingly, one study highlighted a significantly increased risk of acute short-term postoperative complications in frail geriatric patients undergoing cranial surgery for primary central nervous system neoplasm, but no difference in long-term complications at readmission time points.20
Using a variety of definitions, frailty has been correlated with clinically important outcomes (mortality, survival, complications, length of stay, costs, discharge disposition, and readmission) after intracranial surgery, with mFI-5 being the most commonly used measurement tool.18 Other syntheses of the literature have attempted to examine the effects of frailty based on different tumor subtypes, given that each has a unique trajectory and prognosis. In a recent systematic review, the relationship between frailty and outcomes differed between brain tumor subtypes in subtle ways, highlighting that analyzing all tumor types together may underestimate the prognostic value of frailty.21
GlioblastomaIn the aforementioned systematic review, Qureshi et al21 identified 16 recent studies focused on glioblastoma and reported significant relationships between frailty and overall survival, extended hospital lengths of stay, postoperative complications, and extra-familial aid postdischarge. Some authors have argued that elderly patients with significant comorbidity may be less likely to tolerate surgery or adjuvant chemotherapy, and may also be less likely to be offered aggressive treatment, both of which may contribute to worse prognoses for this demographic.22 A recent study suggested that frailty should not hinder offering treatment as elderly patients with low Karnofsky Performance Status scores (a percentage-based score classifying patients as to their level of functional impairment) can still show significant improvement postoperatively.23 However, the lack of validated frailty tools together with the highly progressive nature of malignant brain tumors makes the role of using frailty to guide care in this population unclear at this time.
Intracranial MeningiomaStudies have indicated that higher mFI scores are independently associated with overall postoperative morbidity and mortality in patients with meningioma.21 Kuwabara et al24 found that an mFI-5 score of 2 or more predicted poor outcomes in older patients better than chronological age.24 Another study in patients who underwent skull base meningioma resection found similar perioperative complications in older compared with younger patients, though worse baseline functional status was predictive of complications.25 Among all intracranial tumor types, frailty is an important risk factor for poor outcomes and frailty assessment should be part of the preoperative evaluation.
Chronic Subdural HemorrhageFrailty predicts worse outcomes for patients undergoing surgical drainage of chronic subdural hemorrhage, including higher major complication rates, non–home discharge, and 30-day mortality.26,27 In terms of choice of frailty assessment tools, the Clinical Frailty Scale may be a superior predictor of worse functional outcomes after chronic subdural hemorrhage than the mFI.28 In contrast, the initial Glasgow Coma Scale score was a better predictor of mortality and discharge disposition than age or frailty in patients with acute subdural hematoma in one study.29 Due to the preliminary nature of these analyses, the prognostic value of frailty indices requires further validation in this patient population.
Cerebral AneurysmFrailty has been shown to be similarly predictive of worse outcomes after intracranial aneurysm surgery. A simplified measure of frailty (eg, mFI-5) was an independent predictor of in-hospital complications after surgery for unruptured cerebral aneurysms and was a more useful predictor of postoperative outcome in younger patients (<75 y of age) compared with chronological age.24 In another retrospective study of patients with angiogram-negative SAH, frailty was a better predictor of mortality and discharge to home compared with both the Hunt-Hess and Fisher scores.30 However, frailty did not predict mortality after aneurysmal SAH.19 Frailty may, therefore, have a role in some aspects of prognostication in these populations, although prospective validation is needed and represents a key challenge for surgical decision-making.31
Spine SurgeryAs with intracranial procedures, frailty has consistently been shown to predict adverse events, discharge destination, and mortality in spine surgery patients using a variety of assessment tools.15,32 Using the mFI-11, frailty was a more robust indicator of outcomes after spine surgery than age alone.33,34 Although frailty predicted perioperative adverse events, the mFI did not predict patient-reported outcomes at 3 and 12 months after spine surgery, with most patients achieving a clinically meaningful improvement regardless of frailty status.35
INTERVENTIONS TO IMPROVE OUTCOMES FOR FRAIL NEUROSURGICAL PATIENTSSeveral methods and interventions have been described to improve outcomes for frail patients.
Frailty Screening and Bundled Care PathwaysFrailty represents a potentially modifiable characteristic in the neurosurgical population with significant implications for clinical decision-making, risk stratification, and improving value-based care. Frailty screening may guide appropriate patient selection, escalation in postoperative monitoring, and multidisciplinary engagement. In a broad surgical population, a frailty screening initiative implemented as part of a pragmatic quality improvement program demonstrated mortality reduction across all patient groups, with greater benefit in those with higher levels of frailty, possibly due to greater multidisciplinary involvement and surveillance.36 Similarly, Schmidt et al2 proposed the implementation of a specific neurosurgical comprehensive pathway for the care of the frail patient, with the aim of maintaining independence and preventing frailty-associated disability. In a recent retrospective analysis, a standardized protocol for complex spine surgery was associated with reduced length of hospital stay and intensive care utilization but not complications, although this study was not specific to frail patients.37 While promising, such pathways require further refinement and prospective validation for frail patients with spine and intracranial pathologies.
PrehabilitationPrehabilitation interventions to increase physiological reserve and functional capacity may improve outcomes in frail patients; however, there is currently a lack of sufficient evidence to understand the optimal structure and delivery of such programs.38 Whether prehabilitation improves outcomes in neurosurgical patients specifically is unknown, with sparse literature available on this topic. In other surgical populations, 2 randomized controlled trials in elective colorectal39 and cancer surgery40 did not demonstrate improved postoperative outcomes with prehabilitation, possibly due to suboptimal adherence to prehabilitation protocols.
Role of Surgery to Improve FrailtyThere is increasing evidence that frailty may improve after some surgical interventions, particularly if the patient’s functional impairment is related to a reversible neurological pathology (Fig. 1). This concept is supported by an observational study comparing the trajectory of operative and nonoperative approaches in patients with adult spinal deformity.41 In that study, frailty scores improved in those undergoing surgery despite having greater deformity than those who did not undergo surgery and who were more likely to develop severe frailty. In another study, although frail patients undergoing surgery for degenerative spine disease were more likely to experience short-term adverse events, these patients achieved similar long-term improvements in patient-reported outcomes and quality of life.35 Finally, a large prospective longitudinal study on recovery after elective noncardiac surgery found that although frail patients experienced early increases in disability and complications they ultimately observed greater reductions in disability than non-frail patients regardless of the frailty assessment tool used Fig. 1.4
UNANSWERED QUESTIONS/FUTURE RESEARCHThe literature examining frailty in neurosurgical patients has grown rapidly in recent years, but several areas of focus are needed going forward. Although frailty is now established as a key risk factor for poor outcomes, a range of frailty measurement tools have been used. Rigorous, prospective studies are required to validate either existing or neurosurgery-specific frailty measurement tools, including in both spine and intracranial surgery patients. Another key area of needed research is to establish evidence-based interventions to improve outcomes for frail patients, which will likely be multidimensional in nature (Fig. 2). Such interventions will likely focus on standardized frailty screening, multidisciplinary involvement, evidence-based care pathways, prehabilitation, and rehabilitation, and enhanced postoperative surveillance programs. Furthermore, the optimal patient selection, including frailty thresholds, for inclusion in such pathways remains unknown.
 FIGURE 2:
FIGURE 2: Potential components of a multidimensional approach to improving outcomes for frail patients undergoing neurosurgical procedures upon which to focus future research.
CONCLUSIONAs the neurosurgical population ages, frailty is an increasingly important factor in patient selection, perioperative risk stratification, and optimization to reduce complications. Frailty is measured using the phenotypic or deficit accumulation models, with simplified models such as the Clinical Frailty Scale or mFI commonly used in studies in neurosurgical patients. Increasing frailty consistently predicts worse patient outcomes across a range of neurosurgical procedures, including early complications, disability, non–home discharge, and mortality. Evidence for interventions to improve outcomes for frail patients is limited in the neurosurgical population, although bundled care pathways, exercise programs, and multidisciplinary involvement show promise. Surgery itself may be an intervention to improve frailty in selected patients, and future research should focus on identifying effective interventions to improve both short-term complications and long-term outcomes.
REFERENCES 1. United Nations Department of Economics and Social Affairs, Population Division. New York: World Population Ageing 2019: Highlights; 2019. Accessed December 18, 2023. https://www.un.org/development/desa/pd/news/world-population-ageing-2019-0 2. Schmidt E, Balardy L, Geeraerts T, et al. Geriatric neurosurgery: the unfolding of a new subspecialty. Neurosurg Focus. 2020;49:E2. doi:10.3171/2020.7.FOCUS20509 3. Fried LP, Tangen CM, Walston J, et al. Frailty in older adults: evidence for a phenotype. J Gerontol A Biol Sci Med Sci. 2001;56:M146–M156. doi:10.1093/gerona/56.3.m146 4. McIsaac DI, Taljaard M, Bryson GL, et al. Frailty and long-term postoperative disability trajectories: a prospective multicentre cohort study. Br J Anaesth. 2020;125:704–711. doi:10.1016/j.bja.2020.07.003 5. Mitnitski AB, Mogilner AJ, Rockwood K. Accumulation of deficits as a proxy measure of aging. ScientificWorldJournal. 2001;1:323–336. doi:10.1100/tsw.2001.58 6. Rockwood K, Song X, MacKnight C, et al. A global clinical measure of fitness and frailty in elderly people. CMAJ. 2005;173:489–495. doi:10.1503/cmaj.050051 7. Velanovich V, Antoine H, Swartz A, et al. Accumulating deficits model of frailty and postoperative mortality and morbidity: its application to a national database. J Surg Res. 2013;183:104–110. doi:10.1016/j.jss.2013.01.021 8. Subramaniam S, Aalberg JJ, Soriano RP, et al. New 5-factor modified Frailty Index using American College of Surgeons NSQIP data. J Am Coll Surg. 2018;226:173–181 e8. doi:10.1016/j.jamcollsurg.2017.11.005 9. Hall DE, Arya S, Schmid KK, et al. Development and initial validation of the risk analysis index for measuring frailty in surgical populations. JAMA Surg. 2017;152:175–182. doi:10.1001/jamasurg.2016.4202 10. De la Garza Ramos R, Goodwin CR, Jain A, et al. Development of a Metastatic Spinal Tumor Frailty Index (MSTFI) using a nationwide database and its association with inpatient morbidity, mortality, and length of stay after spine surgery. World Neurosurg. 2016;95:548–555 e4. doi:10.1016/j.wneu.2016.08.029 11. Miller EK, Neuman BJ, Jain A, et al. An assessment of frailty as a tool for risk stratification in adult spinal deformity surgery. Neurosurg Focus. 2017;43:E3. doi:10.3171/2017.10.FOCUS17472 12. McIsaac DI, Harris EP, Hladkowicz E, et al. Prospective comparison of preoperative predictive performance between 3 leading frailty instruments. Anesth Analg. 2020;131:263–272. doi:10.1213/ANE.0000000000004475 13. Stovell MG, Jenkinson MD. Neurosurgery in octogenarians. Br J Neurosurg. 2014;28:611–615. doi:10.3109/02688697.2014.889809 14. McIsaac DI, Wong CA, Huang A, et al. Derivation and validation of a generalizable preoperative Frailty Index using population-based health administrative data. Ann Surg. 2019;270:102–108. doi:10.1097/SLA.0000000000002769 15. Moskven E, Charest-Morin R, Flexman AM, et al. The measurements of frailty and their possible application to spinal conditions: a systematic review. Spine J. 2022;22:1451–1471. doi:10.1016/j.spinee.2022.03.014 16. Torres-Perez P, Alvarez-Satta M, Arrazola M, et al. Frailty is associated with mortality in brain tumor patients. Am J Cancer Res. 2021;11:3294–3303. 17. Zhu J, Qiu X, Ji C, et al. Frailty as a predictor of neurosurgical outcomes in brain tumor patients: a systematic review and meta-analysis. Front Psychiatry. 2023;14:1126123. doi:10.3389/fpsyt.2023.1126123 18. Huq S, Liu J, Romano R, et al. Frailty in patients undergoing surgery for brain tumors: a systematic review of the literature. World Neurosurg. 2022;166:268–278 e8. doi:10.1016/j.wneu.2022.07.039 19. Fortunato M, Lin F, Uddin A, et al. Frailty as a predictor of outcomes in subarachnoid hemorrhage: a systematic review and meta-analysis. Brain Sci. 2023;13:1498. doi:10.3390/brainsci13101498 20. Shahrestani S, Lehrich BM, Tafreshi AR, et al. The role of frailty in geriatric cranial neurosurgery for primary central nervous system neoplasms. Neurosurg Focus. 2020;49:E15. doi:10.3171/2020.7.FOCUS20426 21. Qureshi HM, Tabor JK, Pickens K, et al. Frailty and postoperative outcomes in brain tumor patients: a systematic review subdivided by tumor etiology. J Neurooncol. 2023;164:299–308. doi:10.1007/s11060-023-04416-1 22. Bruno F, Pellerino A, Palmiero R, et al. Glioblastoma in the elderly: review of molecular and therapeutic aspects. Biomedicines. 2022;10:644. doi:10.3390/biomedicines10030644 23. Barak T, Vetsa S, Nadar A, et al. Surgical strategies for older patients with glioblastoma. J Neurooncol. 2021;155:255–264. doi:10.1007/s11060-021-03862-z 24. Kuwabara M, Ikawa F, Michihata N, et al. The 5-factor modified Frailty Index as a more useful associated factor than chronological age after unruptured cerebral aneurysm surgery: a nationwide registry study. Neurosurgery. 2023;92:329–337. doi:10.1227/neu.0000000000002203 25. Przybylowski CJ, Shaftel KA, Hendricks BK, et al. Perioperative complication profile of skull base meningioma resection in older versus younger adult patients. J Neurol Surg B Skull Base. 2022;83:411–417. doi:10.1055/s-0041-1736408 26. Zaki PG, Bolger J, Rogowski B, et al. The utility of the 5-factor modified Frailty Index in outcome prediction for patients with chronic subdural hematoma treated with surgical drainage. World Neurosurg. 2023;179:e328–e341. doi:10.1016/j.wneu.2023.08.085 27. Sastry RA, Pertsch N, Tang O, et al. Frailty and outcomes after craniotomy or craniectomy for atraumatic chronic subdural hematoma. World Neurosurg. 2021;145:e242–e251. doi:10.1016/j.wneu.2020.10.022 28. Kesserwan M, Bergin B, Trivedi A, et al. Assessment of frailty in predicting surgical outcomes in patients with chronic subdural hematomas: retrospective chart review. World Neurosurg. 2021;146:e168–e174. doi:10.1016/j.wneu.2020.10.061 29. Rawanduzy C, McIntyre MK, Afridi A, et al. The effect of frailty and patient comorbidities on outcomes after acute subdural hemorrhage: a preliminary analysis. World Neurosurg. 2020;143:e285–e293. doi:10.1016/j.wneu.2020.07.106 30. McIntyre M, Gandhi C, Dragonette J, et al. Increasing frailty predicts worse outcomes and increased complications after angiogram-negative subarachnoid hemorrhages. World Neurosurg. 2020;134:e181–e188. doi:10.1016/j.wneu.2019.10.003 31. Caffes N, Wenger N, Cannarsa G, et al. Unruptured cerebral aneurysms in elderly patients: key challenges and management. Ann Med. 2021;53:1839–1849. doi:10.1080/07853890.2021.1990393 32. Veronesi F, Borsari V, Martini L, et al. The impact of frailty on spine surgery: systematic review on 10 years clinical studies. Aging Dis. 2021;12:625–645. doi:10.14336/AD.2020.0904 33. Kazim SF, Dicpinigaitis AJ, Bowers CA, et al. Frailty status is a more robust predictor than age of spinal tumor surgery outcomes: a NSQIP analysis of 4,662 patients. Neurospine. 2022;19:53–62. doi:10.14245/ns.2142770.385 34. Flexman AM, Charest-Morin R, Stobart L, et al. Frailty and postoperative outcomes in patients undergoing surgery for degenerative spine disease. Spine J. 2016;16:1315–1323. doi:10.1016/j.spinee.2016.06.017 35. Beauchamp-Chalifour P, Flexman AM, Street JT, et al. The impact of frailty on patient-reported outcomes after elective thoracolumbar degenerative spine surgery. J Neurosurg Spine. 2021:1–9. EPub August 6. doi:10.3171/2021.2.SPINE201879 36. Hall DE, Arya S, Schmid KK, et al. Association of a frailty screening initiative with postoperative survival at 30, 180, and 365 days. JAMA Surg. 2017;152:233–240. doi:10.1001/jamasurg.2016.4219 37. Ayrian E, Sugeir SH, Arakelyan A, et al. Impact of a perioperative protocol on length of ICU and hospital stay in complex spine surgery. J Neurosurg Anesthesiol. 2021;33:65–72. doi:10.1097/ANA.0000000000000635 38. Mohamed B, Ramachandran R, Rabai F, et al. Frailty assessment and prehabilitation before complex spine surgery in patients with degenerative spine disease: a narrative review. J Neurosurg Anesthesiol. 2023;35:19–30. doi:10.1097/ANA.0000000000000787 39. Carli F, Bousquet-Dion G, Awasthi R, et al. Effect of multimodal prehabilitation vs postoperative rehabilitation on 30-day postoperative complications for frail patients undergoing resection of colorectal cancer: a randomized clinical trial. JAMA Surg. 2020;155:233–242. doi:10.1001/jamasurg.2019.5474 40. McIsaac DI, Hladkowicz E, Bryson GL, et al. Home-based prehabilitation with exercise to improve postoperative recovery for older adults with frailty having cancer surgery: the PREHAB randomised clinical trial. Br J Anaesth. 2022;129:41–48. doi:10.1016/j.bja.2022.04.006 41. Passias PG, Segreto FA, Bortz CA, et al. Probability of severe frailty development among operative and nonoperative adult spinal deformity patients: an actuarial survivorship analysis over a 3-year period. Spine J. 2020;20:1276–1285. doi:10.1016/j.spinee.2020.04.010
留言 (0)