
記住我


The presence of errors during anesthesia has been evident since the 1950s. Audits have indicated that human errors significantly contribute to critical incidents in this field.1,2 Education in neuroanesthesia may be more likely to prioritize quality over quantity given the typically smaller case volumes to which trainees are exposed.2 Operating in an environment with minimal error tolerance challenges the effectiveness of training individuals while upholding patient safety.2–4 The use of simulation to address these potential limitations can range from improved learner experience to skill building. Simulation-based learning has the potential to improve the competency of neuroanesthesia trainees, including in communication and teamwork skills.1,5,6
Neuroanesthesia simulation involves the use of various models and designs to recreate realistic clinical scenarios in a risk-free environment, thereby allowing trainees to gain hands-on experience and practice managing complex neurosurgical and neurological emergencies.7 The One Brain simulation program, one of the models used in neuroanesthesia simulation, provides multidisciplinary mock drills on head injuries, venous air embolism, subarachnoid hemorrhage-associated vasospasm, raised intracranial pressure in critically ill patients, and transfer to a definitive care center.8 Simulation can also be used to practice the use of evidence-based checklists and cognitive aids in the management of complex and rarely encountered neuroanesthesia scenarios.9
This focused review provides insights into the current utilization, development, models and designs, and potential strengths and limitations of simulation training in perioperative neuroscience.
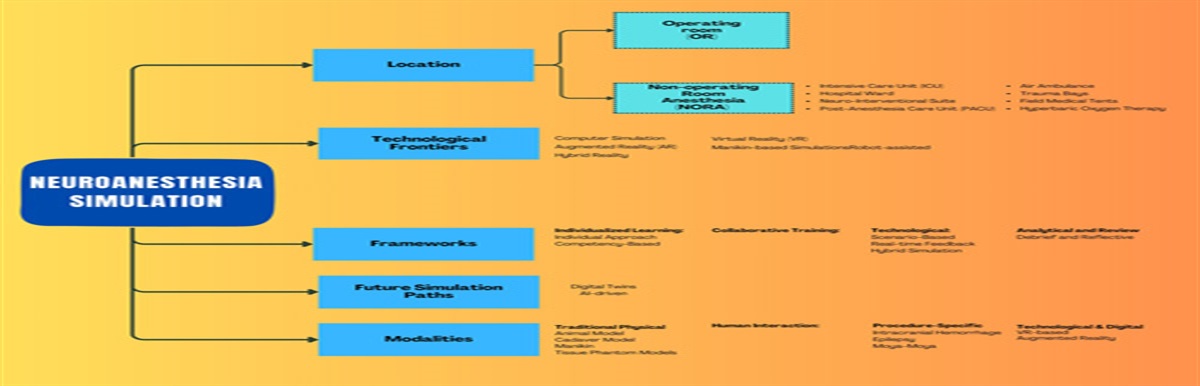
CURRENT SIMULATION MODELSSimulation models can be categorized into several types, including physical models (manikins), screen-based computer simulators, virtual reality simulators, augmented reality simulators, hybrid simulators, animal models, cadaveric models, and mathematical (computational) models (Fig. 1).10,11
 FIGURE 1:
FIGURE 1: Models, frameworks, and designs of neuroanesthesia simulation.
Physical ModelsPhysical models such as manikins are frequently used in simulation-based neuroanesthesia learning. They are designed to replicate actual patients’ anatomy and physiological responses, allowing learners to practice various procedures and interventions in a controlled environment.10,12,13 For example, anesthesiologists can practice airway management and monitoring vital signs during a craniotomy for brain tumor resection, as well as emergency airway control in a patient in a headframe.10,12,13
Screen-based Computer SimulatorsScreen-based computer simulators provide learners with a virtual environment to practice specific neuroanesthesia procedures. They can simulate scenarios such as endovascular coiling of cerebral aneurysms, deep brain stimulation surgery, and ventriculoperitoneal shunt placement.6 Anesthesiologists can also practice managing patients during minimally invasive procedures, focusing on contrast reactions and hemodynamic changes.10
Virtual Reality SimulatorsVirtual reality simulators offer a realistic and immersive experience for learners to practice neuroanesthesia procedures,14 including skull base surgery, awake craniotomy, and cervical laminectomy.10,15 Anesthesiologists can also practice managing complex airway issues, significant blood loss, and patient positioning.10,15
Augmented Reality SimulatorsAugmented realist simulators combine virtual elements with the natural environment to provide a mixed-reality experience for learners. They are able to simulate a range of procedures such as stereotactic radiosurgery, pineal region tumor resection, and Chiari malformation decompression,10 allowing anesthesiologists to practice managing patients undergoing noninvasive procedures with prolonged immobilization, challenges of airway management in the prone position, and potential cerebrospinal fluid shifts and complications.10,16
Hybrid SimulatorsHybrid simulators combine physical and virtual elements to simulate complex neurosurgical procedures such as acoustic neuroma resection, spinal cord tumor resection, and temporal lobectomy for epilepsy.10 Anesthesiologists can practice managing challenges such as prolonged surgeries near cranial nerves, potential intraoperative neurological changes, and intraoperative seizures.10
Animal ModelsAnimal models have been used to practice the management of specific neuroanesthesia scenarios. Live animals can simulate brain trauma management, intracranial hemorrhage, and spinal cord decompression, allowing learners to practice managing traumatic brain injuries, rapid changes in a bleeding brain lesion, and potential neurological changes during cranial decompression.10
Cadaveric ModelsCadaveric models offer a realistic anatomical representation for learners to practice complex neurosurgical and other procedures. These models can simulate complex cranial base surgery, intraventricular tumor resection, and anterior cervical discectomy and fusion.10 Anesthesiologists can practice managing significant blood loss and resuscitation, traumatic injuries, and airway complications.10,17,18
Mathematical (Computational) ModelsMathematical models are used to understand and predict various aspects of neuroanesthesia by simulating brain dynamics during anesthesia, neurophysiological changes during spine surgery, and cerebral blood flow during craniotomy.19 These models provide insights into the brain’s response to anesthetic agents, potential neurological changes during surgery, and blood flow dynamics during different stages of a craniotomy.19
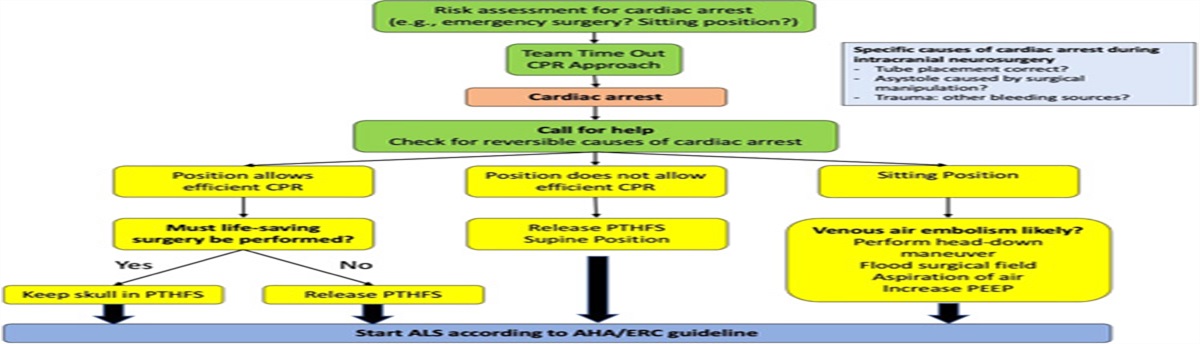
SCENARIOS IN NEUROANESTHESIA SIMULATIONSpecific scenarios can be carefully designed and scripted to recreate realistic situations that trainees may encounter in clinical practice. In these scenarios, learners are given specific roles and responsibilities and must work together to manage a patient effectively (Fig. 2). Examples of scenarios used in simulation training identified from the literature and the authors’ own experience are discussed below.
 FIGURE 2:
FIGURE 2: Various scenarios of neuroanesthesia simulation. ICP indicates Intracranial Pressure; MRI, magnetic resonance imaging.
Unexpected Aneurysm RuptureThis scripted scenario mimics the catastrophic situation of intraoperative aneurysm rupture, where the neurosurgeon asks for acute blood pressure lowering or even flow arrest.20 Trainees learn how to rapidly reduce cardiac output in order to decompress the aneurysm sac and improve surgical visualization by temporary induction of asystole with adenosine, rapid ventricular pacing, or ventricular fibrillation.
Venous Air EmbolismThis scenario mimics a potentially life-threatening situation in sitting position craniotomies and allows trainees to learn management strategies for venous air embolism, including the important role of changes in position during acute management.
Emergency Airway ManagementThis simulation scenario has contributed to the development of clinical frameworks for emergency high-risk airway management in neuroanesthesia.12,17 In a mannequin study by Brockerville et al.,12 the most effective device for emergency airway control during surgery for deep brain stimulation and intraoperative imaging with a stereotactic headframe was assessed. The authors found that a laryngeal mask airway (LMA) was adequate and timely for securing the airway compared with intubation with a direct or video laryngoscope. In a subsequent study utilizing a cadaveric model, Gruenbaum et al17 confirmed that the LMA was the quickest and most reliable primary technique for securing an emergency airway during an awake craniotomy.
Complications of the Prone PositionThe prone position is routinely used in neurosurgical practice to facilitate access to posterior neuroanatomical structures.21 Unintentional tracheal extubation is an uncommon but life-threatening complication for patients in the prone position.22 It is challenging to perform emergency airway management for accidental extubation in a patient in the prone position, and simulation has helped identify effective airway rescue strategies in this scenario. In a randomized crossover mannikin study, the LMA and video laryngoscope were comparable airway management strategies for accidental extubation in the prone position.23 The authors of that study recommend re-intubation with a channeled blade-type video laryngoscope as a valuable method of airway rescue, considering that tracheal intubation can provide greater stability than a LMA. The results from a simulation study by Yamamoto et al.24 suggested that a LMA should be considered as first-line airway device in accidental tracheal extubation in the prone position as compared with advanced airway management devices such as the video laryngoscope and fiberscope. Simulation for other scenarios in the prone position, including code blue, massive hemorrhage, and anaphylaxis, should be developed.
Technical SkillsRefining technical skills for procedures such as tracheal intubation and insertion of lumbar drains, epidural catheters, central venous lines, and arterial lines is an essential facet of neuroanesthesia training. Epidural anesthesia is among the most challenging procedures for anesthesia trainees to learn,25 and residents found the use of a 3D-printed thoracic spine model helpful for learning lumbar epidural placement, central line insertion, and cricothyroidotomy techniques.13
Remote LocationsAs new technologies such as intraoperative magnetic resonance imaging have gained popularity during neurosurgical interventions, preprocedural simulation can assist operating room staff in anticipating and preventing possible complications arising during real patient cases. Chowdhury et al26 reported 2 cases of preprocedural simulation of right frontal craniotomy and prone positioning in planning intraoperative magnetic resonance imaging-guided neurosurgery, which allowed refinement of procedural checklists and enhanced multidisciplinary coordination for improved patient management during the procedure.
Teamwork and Nontechnical SkillsAs the complexity of neurosurgical cases increases, training in advanced cognitive skills, teamwork, and communication should be integrated into medical education. The use of simulation for cognitive training involves practicing scenarios that require trainees to analyze information, make informed decisions, and adapt to changing environments.27 Training processes that involve higher-order decisions have been shown to decrease errors and improve competency and critical thinking in simulation environments.7,28 In prior studies of neurosurgical procedures, multidisciplinary simulation designs improved interdisciplinary communication skills, coordination, and team-based learning.20,29,30 Collaborative debriefing sessions can also facilitate reflective practice and promote metacognition.31
OthersOther perioperative complications, including intraoperative brain bulge, delayed emergence, postoperative neurological deficits, acute delirium, nerve injuries, and sudden visual loss, all lend themselves to the creation of simulation scenarios.
SIMULATION AND OUTCOMESWhile experts agree that simulation training can improve patient safety, there are limited published studies that establish a direct correlation between simulation and improved patient outcomes in neuroanesthesia.32–34 While not specific to neuroanesthesia, 2 systematic reviews and meta-analyses reviewed more than 50 studies to understand the link between simulation training in anesthesiology and improved patient outcomes.35,36 Zendejas et al35 found that simulation-based education was associated with small to moderate (nonstatistically significant) improvements in patient outcomes compared with no simulation training, whereas Lorello et al36 found that anesthesia simulation was associated with a statistically significant moderate to large effect size for all outcomes assessed (satisfaction, knowledge, time, skills, and behavior) except for patient outcomes. Although the benefits of simulation in education are well documented, the challenge may lie in quantifying any impact on patient care and health outcomes. It is important to recognize that the majority of simulation studies constitute a low evidence base; therefore, their findings should be interpreted with caution.
ECONOMIC CONSIDERATIONS OF SIMULATIONEconomic considerations are a critical factor when integrating simulation-based training into medical education. While the benefits of neuroanesthesia simulation are evident, there are challenges related to initial investment costs and resource allocation.37 High-fidelity simulators, simulation center set-up, and training of faculty members require up-front financial commitments. In a study published in 2018, the cost of high-fidelity models such as realistic spine replicas ranged from USD225 for a partial thoracic spine without soft tissue to more than USD6000 for a combined lumbar and thoracic epidural model.8 In addition, models that include soft tissue, which cost about USD1500 per model, require constant replacement.13 Although these simulation models are commercially available, high purchase prices and maintenance costs frequently lead to limited utilization in anesthesia training.13 Low-resource settings present additional challenges that can significantly impact the implementation and effectiveness of neuroanesthesia simulation, including limited infrastructure, financial constraints, and sustainability.37 Han et al.13 proposed the utilization of 3D printing when creating models for medical education due to its cost-effectiveness and adaptability. The 3D-printed thoracic spine model used in those authors’ simulation study was developed at a cost of USD40.01; however, this cost included the material expenses but not the charges for operating a 3D printer and assembly tools.13
When establishing simulation training, it is imperative to consider the overall economic factors rather than only the material costs of simulation. Neuroanesthesia simulation improves provider efficiency, reduces medical errors, and improves patient outcomes,1,8,27,38 and these additive benefits could lead to reduced health care costs in the long run.
UNANSWERED QUESTIONSAlthough simulation-based training offers numerous benefits, several challenges hinder its widespread implementation. The investment costs of high-fidelity mannequins and quality simulation equipment can weaken institutional budgets, limiting access to these training resources.13 In addition, the shortage of time is a challenge faced by all health care professionals, as the demands of clinical schedules restrict time for educational and other initiatives. Maintaining the realism of simulation can also be challenging, particularly when replicating rare and complex neurological conditions.39 A restriction inherent to simulation is the necessity to acknowledge that participants are aware that the presented crisis is purposefully orchestrated.2 This highlights an inherent cognitive limitation intrinsic to human cognition. There is a lack of high-quality evidence showing that simulation improves patient outcomes, including by reducing complications and improving safety.
Several knowledge gaps exist in neuroanesthesia simulation. Standardized simulation models tailored for neuroanesthesia are required, and there is limited evidence on the real-world efficacy of simulation training. One example of a script and design used in neuroanesthesia simulation is a scenario involving a severe traumatic brain injury patient in which trainees are presented with a scripted case where they must manage the patient’s airway, monitor intracranial pressure, administer appropriate medications, and make critical decisions regarding the neurological status. This scenario allows trainees to refine their skills in the management of a complex patient and make time-sensitive decisions that can significantly impact patient outcomes. Importantly, effective feedback mechanisms, long-term skill retention, integration with multidisciplinary teams, cost-effectiveness evaluations, and considerations for cultural and geographical variations also need to be explored.
Future developments may see the integration of advanced technologies such as artificial intelligence into neuroanesthesia simulations, which could enhance the realism and adaptability of simulation.40 Artificial intelligence algorithms could respond dynamically to a learner’s actions, creating a more personalized and challenging learning experience.40 Advances in medical imaging and data analytics could also enable the creation of patient-specific simulations34 in which learners could use patient data in a tailored learning experience that resembles real clinical scenarios. Furthermore, as interest in telemedicine increases, telesimulations could be adapted to link simulators between an instructor and trainees in remote locations.41–43 Simulating telemedicine interactions would help develop skills for remote patient assessment, decision-making, and communication.42
CONCLUSIONSSimulation training in neuroanesthesia has the potential to play a crucial role in providing a safe learning environment for practitioners to practice and gain experience in managing complex scenarios associated with neurosurgical and neurological emergencies. The optimal use of simulation will depend on a variety of factors, including the local or institutional availability of equipment, personnel, and financial resources. Research on the efficacy of simulation training to improve patient and trainee outcomes is needed.
REFERENCES 1. Higham H, Baxendale B. To err is human: use of simulation to enhance training and patient safety in anaesthesia. Br J Anaesth. 2017;119:i106–i114. doi:10.1093/bja/aex302 2. Bhatt R, Khanna P. Simulation in neuroanesthesia: how much to learn. ? J Neuroanaesth Crit Care. 2018;5:83–86. doi:10.1055/s-0038-1667209 3. Khandelwal A, Jangra K, Katikar M, et al. Choosing neuroanaesthesia as a career: marching towards new horizons. Indian J Anaesth. 2021;65:35–42. doi:10.4103/ija.IJA_1531_20 4. Chawla S, Devi S, Calvachi P, et al. Evaluation of simulation models in neurosurgical training according to face, content, and construct validity: a systematic review. Acta Neurochir (Wien). 2022;164:947–966. doi:10.1007/s00701-021-05003-x 5. Lunde L, Moen A, Jakobsen R, et al. Exploring healthcare students’ interprofessional teamwork in primary care simulation scenarios: collaboration to create a shared treatment plan. BMC Med Educ. 2021;21:416. doi:10.1186/s12909-021-02852-z 6. Sameera V, Bindra A, Rath GP. Human errors and their prevention in healthcare. J Anaesthesiol Clin Pharmacol. 2021;37:328–335. doi:10.4103/joacp.JOACP_364_19 7. Chernikova O, Heitzmann N, Stadler M, et al. Simulation-based learning in higher education: a meta-analysis. Rev Educ Res. 2020;90:499–541. doi:10.3102/0034654320933544 8. Chawla R, Pahade A. Simulation in neuroanesthesia: need of the hour in India. J Neuroanaesth Crit Care. 2018;5:184–186. doi:10.1055/s-0038-1675326 9. Hoefnagel A, Rajan S, Martin A, et al. Cognitive Aids for the Diagnosis and Treatment of Neuroanesthetic Emergencies: Consensus Guidelines on Behalf of the Society for Neuroscience in Anesthesiology and Critical Care (SNACC) Education Committee. J Neurosurg Anesthesiol. 2019;31:7–17. doi:10.1097/ANA.0000000000000551 10. Reis G, Yilmaz M, Rambach J, et al. Mixed reality applications in urology: requirements and future potential. Ann Med Surg (Lond). 2021;13:66. doi:10.1016/j.amsu.2021.102394 11. Brusamento S, Kyaw B, Whiting P, et al. Digital health professions education in the field of pediatrics: systematic review and meta-analysis by the Digital Health Education Collaboration. J Med Internet Res. 2019;21:e14231. doi:10.2196/14231 12. Brockerville M, Unger Z, Rowland NC, et al. Airway management with a stereotactic headframe in situ – a mannequin study. J Neurosurg Anesthesiol. 2018;30:44–48. doi: 10.1097/ANA.0000000000000402 13. Han M, Portnova AA, Lester M, et al. A do-it-yourself 3D-printed thoracic spine model for anesthesia resident simulation. PLoS One. 2020;15:e0228665. doi:10.1371/journal.pone.0228665 14. McGuire L, Alaraj A. Competency assessment in virtual reality-based simulation in neurosurgical training Alaraj A. Comprehensive Healthcare Simulation: Neurosurgery. Chicago, IL: Springer; 2018. 15. Flexman A, Wang T, Meng L. Neuroanesthesia and outcomes: evidence, opinions, and speculations on clinically relevant topics. Curr Opin Anaesthesiol. 2019;32:539–545. doi:10.1097/ACO.0000000000000747 16. Ameri G, Rankin A, Baxter J, et al. Development and evaluation of an augmented reality ultrasound guidance system for spinal anesthesia: preliminary results. Ultrasound Med Biol. 2019;45:2736–2746. doi:10.1016/j.ultrasmedbio.2019.04.026 17. Gruenbaum S, Bilotta F, Bertasi T, et al. Emergency airway management during awake craniotomy: comparison of 5 techniques in a cadaveric model. J Neurosurg Anesthesiol. 2022;34:74–78. doi:10.1097/ANA.0000000000000731 18. Beaven A, Griffin D, James H. Highly realistic cadaveric trauma simulation of the multiply injured battlefield casualty: an international, multidisciplinary exercise in far-forward surgical management. Injury. 2021;52:1183–1189. doi:10.1016/j.injury.2020.09.023 19. Kotcherlakota S, Pelish P, Hoffman K, et al. Augmented reality technology as a teaching strategy for learning pediatric asthma management: mixed methods study. JMIR Nurs. 2020;3:e23963. doi:10.2196/23963 20. Calcagno H, Lucke-Wold B, Noles M, et al. Integrated otolaryngology and anesthesia simulation model for crisis management of cavernous carotid artery injury. Arch Neurol Neuro Disord. 2018;1:30–41. doi:10.22259/2638-504x.0101007 21. Sengupta D, Dube S, Rajagopalan V, et al. Modified prone positioning during neurosurgery: sphinx and concorde positions revisited. J Neuroanaesth Crit Care. 2021;8:123–125. doi:10.1055/s-0040-1715356 22. Jérome L, Diabira S, Gentili M. Airway management with a laryngeal mask after accidental tracheal extubation of a patient in prone position for surgical kyphoplasty. Anaesthesiol Intensive Ther. 2020;52:173–174. doi:10.5114/ait.2020.95169 23. Oshika H, Koyama Y, Taguri M, et al. Supraglottic airway device versus a channeled or non-channeled blade-type videolaryngoscope for accidental extubation in the prone position: a randomized crossover manikin study. Medicine. 2018;97:e11190. doi:10.1097/MD.0000000000011190 24. Yamamoto N, Ishii A, Miyashita T, et al. Airway management strategy for accidental tracheal extubation in the prone position: a simulation study. J Clin Anesth. 2020;63:109786. doi:10.1016/j.jclinane.2020.109786 25. Rajagopalan S, Shah K, Guffey D, et al. Predictors of difficult epidural placement in pregnant women: a trainees’ perspective. J Anaesthesiol Clin Pharmacol. 2019;35:548–552. doi:10.4103/joacp.JOACP_340_18 26. Chowdhury T, Bergese SD, Soghomonyan S, et al. The role of simulation in planning intraoperative magnetic resonance imaging-guided neurosurgical procedures: a case report. A A Case Rep. 2017;8:158–160. doi:10.1213/XAA.0000000000000452 27. Builes-Aguilar A, Díaz-Gómez J, Bilotta F. Education in neuroanesthesia and neurocritical care: trends, challenges and advancements. Curr Opin Anesthesiol. 2018;31:520–525. doi:10.1097/ACO.0000000000000628 28. Turkot O, Banks M, Lee S, et al. A review of anesthesia simulation in low-income countries. Curr Anesthesiol Rep. 2019;9:1–9. doi:10.1007/s40140-019-00305-4 29. Ciporen J, Gillham H, Noles M, et al. Crisis management simulation: establishing a dual neurosurgery and anesthesia training experience. J Neurosurg Anesthesiol. 2018;30:65–70. doi:10.1097/ANA.0000000000000401 30. Lucke-Wold B, Gillham H, Baskerville M, et al. Establishing a multidisciplinary cavernous carotid injury simulation to train neurosurgical, otolaryngology, and anesthesia residents. J Vis Exp. 2021;175:e56403. doi:10.3791/56403 31. Patel D, Dawoud F, Lucke-Wold B, et al. Crisis management simulation: the value of interdisciplinary debriefing. Acta Sci Neurol. 2021;4:39–45. 32. Young S, Dunipace D, Pukenas E, et al. Can simulation improve patient outcomes? Int Anesthesiol Clin. 2019;57:68–77. doi:10.1097/AIA.0000000000000240 33. Sollid S, Dieckman P, Aase K, et al. Five topics health care simulation can address to improve patient safety: results from a consensus process. J Patient Saf. 2019;15:111–120. doi:10.1097/PTS.0000000000000254 34. Green M, Tariq R, Green P. Improving patient safety through simulation training in anesthesiology: where are we. Anesthesiol Res Pract. 2016;2016:4237523. doi:10.1155/2016/4237523 35. Zendejas B, Brydges R, Wang A, et al. Patient outcomes in simulation-based medical education: a systematic review. J Gen Inter Med. 2013;28:1078–1089. doi:10.1007/s11606-012-2264-5 36. Lorello G, Cook D, Johnson R, et al. Simulation-based training in anaesthesiology: a systematic review and meta-analysis. Br J Anaesth. 2014;112:231–245. doi:10.1093/bja/aet414 37. So H, Chen P, Wong G, et al. Simulation in medical education. J R Coll Physicians Edinb. 2019;49:52–57. doi:10.4997/JRCPE.2019.112 38. Morris N, Czeisler B, Sarwal A. Simulation in neurocritical care: past, present, and future. Neurocrit Care. 2019;30:522–533. doi:10.1007/s12028-018-0629-2 39. Boggs S, Luedi M. Nonoperating room anesthesia education: preparing our residents for the future. Curr Opin Anaesthesiol. 2019;32:490–497. doi:10.1097/ACO.0000000000000743 40. Mishra S, Gupta R, Biswas S. Role of telemedicine in anesthesia: are we ready yet? Bali J Anesthesiol. 2021;5:230–233. doi:10.4103/bjoa.BJOA_51_21 41. Sharma D. Advancing neuroanesthesia and neurocritical care during the COVID-19 pandemic and infodemic: focus on education, innovation, and collaboration. J Neuroanaesth Crit Care. 2020;7:52–53. doi:10.1055/s-0040-1713018 42. McCoy C, Sayegh J, Alrabah R, et al. Telesimulation: an innovative tool for health professions education. AEM Educ Train. 2017;1:132–136. doi:10.1002/aet2.10015 43. Sidi A, Gravenstein N, Vasilopoulos T, et al. Simulation-based assessment identifies longitudinal changes in cognitive skills in an anesthesiology residency training program. J Patient Saf. 2021;17:e490–e496. doi:10.1097/PTS.0000000000000392
留言 (0)