
記住我


A 5-year-old girl presented to our hospital with a painless neck swelling dating from 6 months ago. Initial evaluation showed no changes in her appetite, weight, bowel habits, or sleep pattern. There were also no associated symptoms. The patient’s parents denied any changes in her voice or breathing pattern recently, and no history of radiation exposure. There was no past history of medical diseases. Family history was unremarkable in both parents’ families.
On physical examination, height and weight were within normal ranges for age. General examination of the patient showed normal appearance, body built, and complexion. Vital signs showed a pulse count of 86, Blood pressure of 100/60 mmHg, Temperature of 37.2 ℃, and a respiratory rate of 23. Thus, there were no remarkable changes that could raise suspicion of hypo or hyperthyroidism. She had an olive-sized palpable non-tender right thyroid nodule that moved with deglutition, and a few lymph nodes were palpated at the right side of the neck at levels II and III (upper and middle deep cervical lymph nodes).
The thyroid function test results were all within normal ranges. Neck ultrasonography (Fig. 1) showed an enlarged right thyroid lobe with a large solid, wider than taller nodule of mixed echogenicity with microcalcifications (A), its size was about 19 × 14 mm, and radiologically classified as TIRADS IV, this was accompanied by an enlarged upper right upper cervical (B), lower cervical (C), and paratracheal (D) LNs showing cortical thickening, and the lower cervical LNs showed similar echogenicity to the thyroid nodule.
Fig. 1
Neck ultrasonography showing A right thyroid lobe with a single nodule (19 × 14 mm) with cystic and solid parts, ill-defined outline, and foci of micro-calcifications. B Right upper cervical lymph nodes and C right lower cervical lymph nodes, both being distorted with abnormal shape and absent hila. D Paratracheal lymph nodes
The clinical and radiologic findings raised the suspicion of a malignant thyroid nodule, thus requiring a biopsy. Fine needle aspiration cytology was performed showing bloody material and no detected atypical cells, Bethesda I. Based on the earlier findings, the possibility of carcinoma could not be excluded and a diagnostic right lobectomy with an intraoperative frozen section was planned after MDT discussion and counseling with the patient’s family. Since the FNAC results were not conclusive for PTC and there were no symptoms or signs suggestive of distant metastases, preoperative metastasis workup was not recommended for the patient.
A preoperative laryngeal examination was carried out by an otolaryngologist and confirmed the presence of bilateral freely mobile vocal cords.
The right lobectomy was performed through a Kocher collar incision, and the specimen was sent for intraoperative frozen section examination. The result was conclusive for poorly differentiated papillary thyroid cancer. This was followed by a completion left hemithyroidectomy and right central (levels VI and VII) and lateral lymph node dissection (levels II, III, and IV) (Fig. 2) which was carried out after extending the incision into a hockey stick neck incision in the right side. The recurrent laryngeal nerves were identified on both sides and marked to be safe and uninjured, the tumor was on the anterior surface of the right thyroid away from the right recurrent laryngeal nerve. This with the fact that no changes happened to the voice or the breathing of the child after the surgery disputed the need to perform a post-operative laryngeal examination.
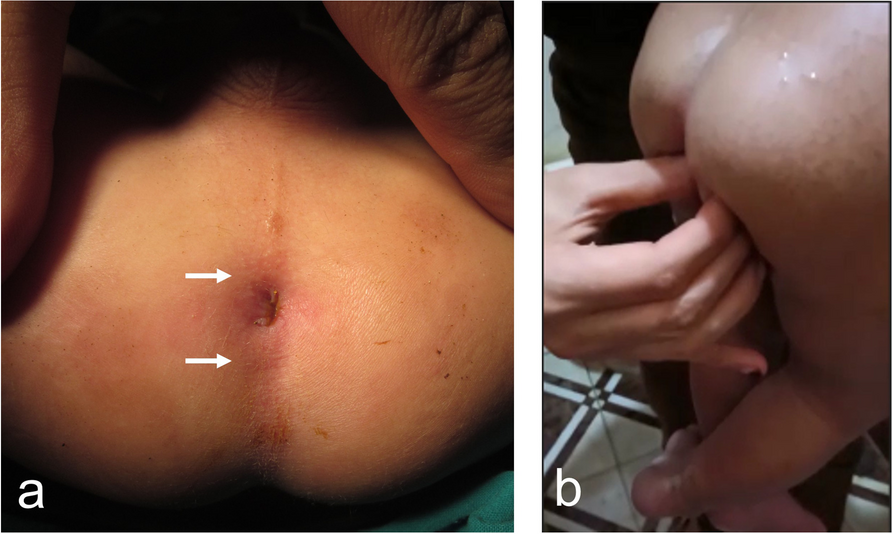
Fig. 2
Intraoperative images showing A preoperative assessment of the mass, B right thyroid lobectomy, C lateral neck dissection, and D postoperative samples of the left thyroid lobe, central lymph node compartment, and the lateral groups of lymph nodes
Examination of prepared slides from the right lobe revealed infiltration by tumor tissue (2.5 × 1.5 × 1 cm) in size, formed of atypical epithelial cells, mostly arranged in trabecular and insular patterns. These exhibit a moderate degree of nuclear atypia with mitotic activity of about 3/10 HPFs. There is difficulty identifying nuclear grooving and pseudo inclusions. However, minute foci showed an attempt for papillary configuration (< 5% of tumor tissue). No significant tumor necrosis. The surrounding thyroid tissue showed unremarkable changes. Tumor tissue was seen reaching the capsule, with extrathyroidal extension and multiple satellites. No perineural tumor invasion was detected in the examined material (Fig. 3). The left lobe revealed variable-sized thyroid follicles lined by low cuboidal to flat cells and containing eosinophilic colloid. It was free from tumor tissue. Free thymic tissue was also noted. Sections prepared from the right central nodes revealed infiltration of ten out of eleven nodes dissected, while five out of thirty-four lateral cervical nodes were infiltrated.
Fig. 3
Pathological examination of the right thyroid lobe nodule showing A papillary structures and psammoma bodies, B papillary formation and grooving, and C papillae and capsule infiltration
The patient was then referred to a nuclear medicine physician. Adjuvant radioactive iodine 131 (RAI131) therapy was decided since the patient was categorized as high risk according to the ATA classification system. The activity of RAI therapy was decided to be 30 mci. The benefits and risks of RAI131 for the patient and her family were discussed with the parents. A whole-body scan with SPECT-CT was performed 4 days after RAI 131 intake showing increased uptake of the tracer at the thyroid bed, clear lung fields, no bony metastasis, and no uptake by the cervical LNs.
Then the patient started Levothyroxine suppressive therapy (75 µg daily). Six months after receiving RAI 131, an assessment of response was performed with a whole-body iodine scan (2 mci), which revealed a complete resolution of the previous uptake seen in the post-treatment scan. Serum-stimulated thyroglobulin level was within normal range and neck ultrasound was free. The patient was scheduled for regular follow-up visits every 6 months, to be monitored by neck imaging and laboratory tests. After more than 1 year of follow-up, she was free from local, nodal, or distant recurrence.
留言 (0)