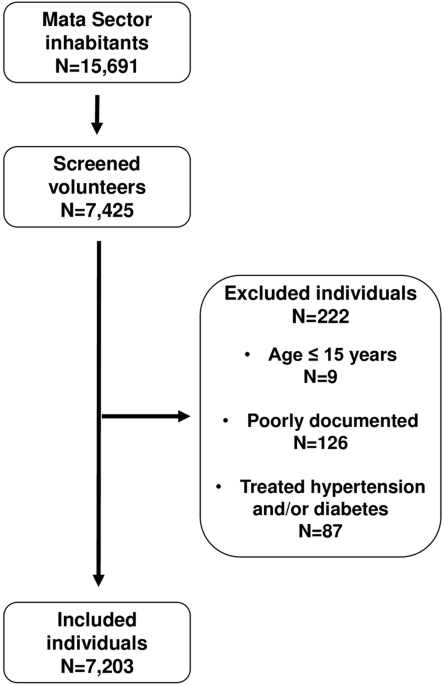
Data were from the ALSPAC birth cohort, which investigates factors that influence childhood development and growth. Altogether, pregnant women resident in Avon, UK with expected dates of delivery from 1st April 1991 to 31st December 1992 were invited to take part in the study. The initial number of pregnancies enroled is 14,541, of which there was a total of 14,676 foetuses. When the oldest children were approximately 7 years of age, an attempt was made to bolster the initial sample size with eligible cases who had failed to join the study originally resulting in 14,901 children alive at 1 year of age. Regular clinic visits of the children commenced at 7 years of age and are still ongoing into adulthood. In this study, 1574 participants had who had complete ST, LPA, MVPA at age 15 years and arterial measurements at age 17 years were eligible for analyses. Ethical approval for the study was obtained from the ALSPAC Ethics and Law Committee and the Local Research Ethics Committees. Informed consent for the use of data collected via questionnaires and clinics was obtained from participants following the recommendations of the ALSPAC Ethics and Law Committee at the time [23,24,25]. Consent for biological samples has been collected in accordance with the Human Tissue Act (2004). Please note that the study website contains details of all the data that is available through a fully searchable data dictionary and variable search tool (http://www.bristol.ac.uk/alspac/researchers/our-data/).
Physical activity and sedentary time assessment
ST, LPA and MVPA were assessed with ActiGraphTM AM7164 2.2 (LLC, Fort Walton Beach, FL, USA) accelerometer worn on the waist for 7 days at 15-year clinic visits [26,27,28]. A valid day was defined as providing data for at least 10 h per day (excluding sequences of 10 or more minutes with consecutive zero counts) and children were only included in the analyses if they provided at least 3 valid days of recording (two weekdays and one weekend day). The devices capture movement in terms of acceleration as a combined function of frequency and intensity. Data are recorded as counts that result from summing postfiltered accelerometer values (raw data at 30 Hz) into epoch units. Data were processed using Kinesoft software, version 3.3.75 (Kinesoft), according to established protocol. Activity counts per minute threshold as proposed by Everson were used to calculate the amount of time spent; MVPA, >2296 counts per minute (cpm); for LPA, 100–2296 cpm; and for ST, 0–<100 cpm [6, 22, 29]. The Evenson cutpoint used in stratifying activity threshold has been suggested as the most appropriate cut point for youth having shown the best overall performance across all intensity levels [30, 31]. ST and LPA were grouped in tertiles as low, middle and high tertile categories. MVPA was classified according to PA guideline recommendations of <40 min/day as low, 40–<60 min/day as moderate and ≥60 min/day as high [12]. The low category was the reference category.
Anthropometry and body composition
Anthropometry (height and weight) of participants at age 15 years was assessed in line with standard protocols and body mass index (BMI) was computed as weight in kilograms per height in metres squared [7, 22]. Body composition (total body fat mass, trunk fat mass and lean mass) was assessed using a dual-energy X-ray absorptiometry scanner at 15 years as previously described [2, 7, 22]. All participants had attained puberty by the 17-year clinic visit assessment using a time (years) to age at peak height velocity objective assessment derived from Superimposition by Translation And Rotation mixed-effects growth curve analysis [22, 32]. The participant’s mother’s socioeconomic status was grouped according to the 1991 British Office of Population and Census Statistics classification [33].
Vascular phenotype
At age 17 years cfPWV was computed from pressure waveforms obtained using the Vicorder device (Skidmore Medical, Bristol, UK) observing standard protocols as detailed earlier [2, 7, 22]. All measurements were taken independently by one of two trained vascular technicians (inter-observer mean difference 0.2 m/s, SD 0.1) [2, 22]. cIMT from the right and left common carotid arteries at 17 years was assessed by ultrasound using a linear 12 MHz transducer (Vivid7, GE Medical, Chicago, Illinois) [7, 22] Interobserver variability for cIMT was assessed in a separate sample of 25 young adults (coefficient of variation: 4.4 ± 2.2%) [2, 6, 7, 22]. For our analysis, we computed the mean of the average measurement of the right and left common carotid arteries as cIMT. Carotid elasticity was computed as the difference between the baseline (end diastole) and peak (systole) vessel diameter.
Cardiometabolic and lifestyle factors
Heart rate and systolic and diastolic BP were measured with Omron monitor at age 15 years as previously detailed [7, 22]. Hypertensive systolic BP was categorised as ≥130 mmHg based on clinical guidelines in paediatrics [34]. Using standard protocols, fasting blood samples at age 15 years were collected, spun and frozen at −80 °C and a detailed assessment of fasting glucose, insulin, high-sensitivity C-reactive protein, low-density lipoprotein cholesterol, high-density lipoprotein cholesterol and triglycerides has been reported (coefficient of variation was <5%) [2, 7, 22]. Homeostatic model assessment for insulin resistance (HOMA-IR) was computed from (fasting insulin × fasting glucose/22.5) [35]. Questionnaires to assess smoking behaviour were administered at age 15-year clinic visits. A specific question regarding whether participants smoked in the last 30 days was used as an indicator of current smoking status. At the 17-year clinic visit, participants were briefly asked about their personal and family (mother, father and siblings) medical history such as a history of hypertension, diabetes, high cholesterol and vascular disease [36].
Statistical analysis
Cohort descriptive characteristics were summarized as means and standard deviation, medians and interquartile ranges, or frequencies and percentages. We explored sex differences using Independent t tests, Mann Whitney-U tests, or Chi-square tests for normally distributed, skewed or dichotomous variables, respectively. Multicategory variables were analysed using a one-way analysis of variance. Normality was assessed by histogram curve, quantile-quantile plot and Kolmogorov-Smirnov tests. A logarithmic transformation of skewed variables was conducted and normality was confirmed prior to further analysis.
Mediating path analyses using structural equation models separately examined the mediating role of total body fat mass, trunk fat mass, lean mass, systolic BP, diastolic BP and HOMA-IR on the associations of ST, LPA, or MVPA with each of cfPWV, cIMT and carotid elasticity. Analyses were adjusted for age, sex, the time between exposure and outcome measure, high sensitivity C-reactive protein, heart rate, systolic BP, smoking status, family history of hypertension/diabetes/high cholesterol/vascular disease, socioeconomic status, high-density lipoprotein cholesterol, low-density lipoprotein cholesterol, triglyceride, lean mass or total fat mass, glucose and insulin, with ST, LPA, or MVPA depending on the mediator and predictor. β from the mediation analyses are standardized regression coefficients. The path models had three equations per regression analysis: the associations of ST, LPA, or MVPA with total body fat mass, trunk fat mass, lean mass, systolic BP, diastolic BP or HOMA-IR (Equation 1); the associations of total body fat mass, trunk fat mass, lean mass, systolic BP, diastolic BP or HOMA-IR with cfPWV, cIMT and carotid elasticity (Equation 2); and the associations of ST, LPA and MVPA with cfPWV, cIMT and carotid elasticity (Equation 3, total effect) and Equation 3’(direct effect) accounted for the mediating role of total body fat mass, trunk fat mass, lean mass, systolic BP, diastolic BP, or HOMA-IR on the longitudinal associations of ST, LPA and MVPA with cfPWV, cIMT and carotid elasticity. The proportion of mediating or suppressing roles was estimated as the ratio of the difference between Equation 3 and Equation 3’ or the multiplication of Equations 1 and 2 divided by Equation 3 and expressed in percentage. A mediating or indirect role is confirmed when there are statistically significant associations between (a) the predictor and mediator, (b) the predictor and outcome, (c) the mediator and outcome and (d) the longitudinal associations between the predictor and outcome variable was attenuated upon inclusion of the mediator [37]. However, when the magnitude of the association between the predictor and outcome is increased upon inclusion of a third variable, a suppression is confirmed [37]. Path analyses were conducted with 1000 bootstrapped samples.
The separate associations of ST, LPA and MVPA categories with each of cfPWV, cIMT and carotid elasticity were examined using linear mixed-effect models. The optimal model was one with sex and predictor as a factor and a random intercept modelled on the subject level. We selected a random effect variance component type and determined the effect of the predictor on the outcome variables. Whilst the mixed effect model assumes that the data are missing at random and is robust for accounting for missing data at follow-up, we elected to additionally conduct 20 cycles of multiple imputations to account for missing data, that have been shown to have a relative efficiency of over 98% in simulating real data [2, 6, 7, 38, 39]. The analysis strategy was adjusted for sex and the time difference between predictor and outcome measures, age, low-density lipoprotein cholesterol, insulin, triglyceride, high-sensitivity C-reactive protein, high-density lipoprotein cholesterol, heart rate, systolic BP, glucose, fat mass, lean mass, smoking status, family history of hypertension/diabetes/high cholesterol/vascular disease and socioeconomic status with an additional adjustment for ST, LPA, or MVPA depending on the predictor.
Lastly, sex-based linear regression analyses were conducted for the associations of ST, LPA and MVPA with each of cfPWV, cIMT and carotid elasticity, adjusting for the above-listed covariates except sex. Based on the evidence that elevated BP may cause premature cardiac damage in youth [40], analyses were conducted for the associations of ST, LPA and MVPA with each of cfPWV, cIMT and carotid elasticity according to systolic hypertension status, adjusting for the above-listed covariates, except systolic BP. Collinearity diagnoses were performed and results with a variance inflation factor <5 were accepted. Differences and associations with a two-sided p value < 0.05 were considered statistically significant, and conclusions were based on effect estimates and their confidence intervals. Sidak correction for potential multiple comparisons was applied. The time difference in years between the exposure measurement at age 15 years and the measurement of vascular outcome at age 17 years was included in the model and controlled. Analyses involving 10% of a sample of 10,000 ALSPAC children at 0.8 statistical power, 0.05 alpha and two-sided p value would show a minimum detectable effect size of 0.084 standard deviations if they had relevant exposure for a normally distributed quantitative variable [41]. All statistical analyses were performed using SPSS statistics software, Version 27.0 (IBM Corp, Armonk, NY, USA).


留言 (0)