
記住我

Men and women aged 45–70 years living in the semirural Finnish towns of Harjavalta and Kokemäki (6013 eligible inhabitants on 31.12.2007) were invited to participate in the Harmonica (Harjavalta Risk Monitoring for Cardiovascular Disease) Project. Institutionalized persons and individuals with previously diagnosed CVD or diabetes were excluded from this primary prevention project. Screening and interventions were performed from August 2005 to September 2007.
The study procedures have been described in detail previously [10]. Briefly, a cardiovascular risk factor survey, a tape for the measurement of waist circumference (WC), and a type 2 diabetes (T2D) risk assessment questionnaire (FINDRISC, Finnish Diabetes Risk Score, available from www.diabetes.fi/english) [11] were mailed to every eligible inhabitant. In the risk factor survey, subjects were asked to measure their WC at the level of umbilicus (inclusion criteria: WC ≥ 80 cm in women and ≥94 cm in men in Harjavalta), to report the latest measured BP (inclusion criteria: BP ≥ 140/90 mmHg), their use of antihypertensive medication, their history of gestational diabetes or hypertension, and history of coronary heart disease, myocardial infarction, or stroke of their parents or siblings. The subjects were asked to fill-in and mail the risk factor survey to the public health care center if they were willing to participate in the project. Participation and all the measurements included were free of charge for the subjects. The response rate as 74% (4450 of 6013).
The respondents with at least one above-mentioned risk factor or ≥15 points (≥12 points in Harjavalta) in the FINDRISC were invited for laboratory tests and an appointment with a trained public health nurse. The stringent inclusion criteria regarding WC and FINDRISC scores were used in Kokemäki for logistical reasons and due to limited financial resources.
Appointment with the study nurseWaiting for the nurse’s appointment, the study participants completed self-administrated questionnaires including details on education, current smoking, alcohol consumption (Alcohol Use Disorders Identification Test, AUDIT [12]) and leisure-time physical activity (LTPA). At the nurse’s appointment a physical examination (including measurements of BP, WC, height and weight) was performed and lifestyle counseling was given [10]. The presence of ongoing antihypertensive medication was confirmed from the patient and from the medical records. Subjects with hypertension, newly detected glucose disorders, metabolic syndrome (MetS), obesity, or ≥5% risk for developing a fatal CVD event according to the Systematic Coronary Risk Evaluation System (SCORE) [11] were categorized as high-risk subjects, and they were offered to have an appointment with the general practitioner (GP) of the project. The persons who attended the nurse’s or the nurse’s and GP’s appointment, were included in the present study (n = 2659).
MeasurementsBP was measured with a calibrated mercury sphygmomanometer by a trained nurse with subjects in a sitting posture after resting for at least five minutes with the cuff placed on the arm. An appropriate-sized cuff was used, depending on the circumference of the arm. In each participant, the mean of two BP readings taken at intervals of at least two minutes was used in the study. Subjects were provided with and taught to use an automatic validated BP device (Omron® M4-1, the Netherlands) for home BP monitoring, if the nurse measured the mean systolic BP ≥ 140 mmHg or the mean diastolic BP ≥ 90 mmHg and the subject did not have ongoing antihypertensive medication. These subjects were instructed to take duplicate BP measurements at home after five minutes of rest in the morning and evening for one week. The mean home BP was calculated from the recorded measurements excluding the first day [13].
Body mass index (BMI) was calculated as weight (kg) divided by the square of height (m²). MetS was defined according to the criteria of the International Diabetes Federation (IDF) [14].
Laboratory testsBlood was drawn after at least 12 h of fasting. Total cholesterol, high-density lipoprotein cholesterol (HDL-C) and triglycerides were measured enzymatically (Olympus® AU640, Japan). Low-density lipoprotein cholesterol (LDL-C) was calculated according to Friedewald’s formula [15]. A 2-h oral glucose tolerance test (OGTT) was performed by measuring fasting plasma glucose and 2-h plasma glucose after ingestion of a glucose load of 75 g anhydrous glucose dissolved in water. Glucose values were measured from capillary whole blood with HemoCue® Glucose 201+ system (Ängelholm, Sweden). The analyzer converts the result from capillary whole blood to plasma glucose (conversion factor 1.11).
Appointment with the general practitionerAn appointment with the study GP was arranged for persons with high CVD risk (as described above) within 2–4 months after the nurse’s appointment. At that time, plasma lipids and fasting plasma glucose were retested, and an ECG and laboratory tests were collected to screen for secondary hypertension or dyslipidaemia. The GP examined the patients and gave lifestyle counseling. According to the national Finnish guidelines of that time, antihypertensive medication was prescribed if systolic BP was ≥160 mmHg or diastolic ≥100 mmHg. In patients with newly detected diabetes or hypertensive target organ damage (albuminuria, left ventricular hypertrophy on ECG), antihypertensive medication was initiated if systolic BP was ≥140 mmHg or diastolic BP ≥ 90 mmHg. If the study subjects had ongoing antihypertensive medication, it was intensified if systolic BP was ≥140 mmHg or diastolic ≥85 mmHg (≥80 mmHg in patients with diabetes. An antihypertensive drug, a lipid-lowering agent, or low-dose aspirin was prescribed if the 10-year risk for developing a fatal CVD event now or extrapolated to the age of 60 years was ≥5% estimated by the SCORE system [16]. A follow-up appointment with the study GP was arranged if new medications were started, or if previous medication was modified.
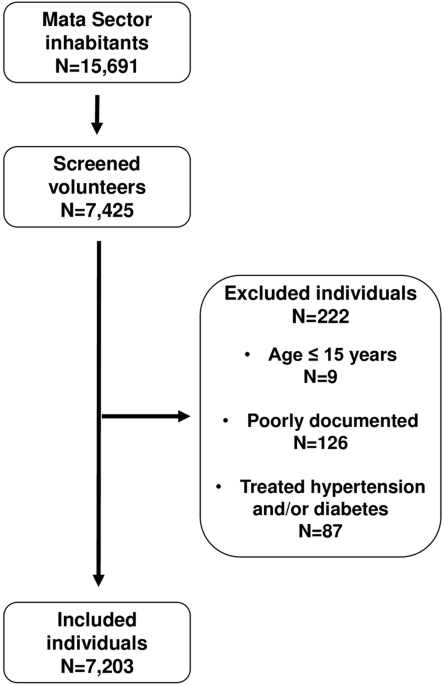
Definitions and formation of study groupsThe formation of study groups is illustrated in Fig. 1. Persons were defined as normotensives if they had no antihypertensive medication at enrollment, and the mean of nurse-measured BP was <140/90 mmHg or the average of home BP values was <135/85 mmHg. Screen-detected hypertension was diagnosed if the subject had no antihypertensive medication, and the mean of home BP measurements were ≥135 mmHg for systolic BP or ≥85 mmHg for diastolic BP [13]. Subjects having ongoing antihypertensive medication at enrollment were regarded as the medicated group.
Fig. 1
Formation of study groups.
Glucose metabolism disorders were categorized as T2D (fasting glucose ≥7.0 mmol/l or 2-h postload plasma glucose ≥12.2 mmol/l) [17]—those patients later referred as having newly diagnosed diabetes—and prediabetes including impaired glucose tolerance (IGT: 2-h postload plasma glucose 8.9–12.2 mmol/l), and impaired fasting glucose (IFG: 6.1-6.9 mmol/l).
LTPA level was categorized as low (LTPA for ≥30 min at a time for maximum of three times a week), moderate (LTPA for ≥30 min at a time for four to five times a week), and high (LTPA ≥ 30 min at a time for six or more times a week).
MortalityData on mortality was obtained from Statistics Finland. Statistics Finland is an independently acting government agency belonging to the administrative sector of the Ministry of Finance. Statistics Finland has collected information on causes of death of Finnish citizens according to the International Classification of Diseases and Related Health Problems, 10th Revision (ICD-10) from the year 1996. We categorized the causes of death as deaths from all causes and deaths from cardiovascular causes: diseases of the circulatory system, I00-I99 (excluding I26 pulmonary embolism with acute cor pulmonale and I26.9 pulmonary embolism without acute cor pulmonale) and vascular dementia, F01.0-F01.9. For each person, the date of the invitation to the Harmonica project was the start date of the observational period. Follow-up time of mortality ended on December 31st, 2018.
Statistical analysesThe descriptive statistics were presented as means with standard deviation (SD), as medians with interquartile range (IQR) or counts with percentages. Group differences in baseline were investigated through a series of one-way analysis of variances (ANOVA) and chi-square test with post hoc comparisons using Hommel’s correction. Kaplan-Meier’s survival analysis were performed to estimate cumulative all-cause and CVD mortality. Adjusted Kaplan-Meier cumulative mortality rates were estimated using two propensity score-based techniques, stratification and weighting (MMWS, marginal mean weighting through stratification) [18]. MMWS is an extension of propensity score matching that combines propensity score stratification and inverse probability of treatment weighting. Adjustments were made for age, gender, total cholesterol, newly diagnosed diabetes, education years, current smoking, LTPA, and BMI. We used Cox proportional hazards model to calculate the adjusted hazard ratios (HR) for death and the Fine and Gray competing risks regression model to calculate subhazard ratios (sHR) due to CVD mortality (with other causes death as a competing event). The proportional hazards assumption was tested graphically and by use of a statistical test based on the distribution of Schoenfeld residuals. The normality of variables was evaluated graphically and by using the Shapiro–Wilk W test. Stata 16.0 (StataCorp LP, College Station, TX, USA) was used for the statistical analyses.
留言 (0)