Since the outbreak of COVID-19, there have been several reports of ocular manifestations associated with the disease. Reported ocular symptoms include conjunctivitis [6], anterior uveitis, dynamic retinal vascular abnormalities such as Paracentral Acute Middle Maculopathy (PAMM) or Acute Macular Neuroretinopathy (AMN) and rarely, inflammation of the retina or choroid [4, 7].
We report a case of a severe bilateral macular dysfunction that manifested 2 months after PCR confirmation of a COVID-19 infection. The time passed between the infection and the manifestation of the eye symptoms may seem rather long, but since there was no other event in the patient’s medical history, and chest x-ray, MRI scans and laboratory tests for other potentially relevant infectious origins (such as tuberculosis, treponema, hepatitis) came back negative, we have no reason to suspect any other concurrent causes. Additionally, it is not impossible that the patient’s disease has started earlier with subclinical symptoms that progressed over weeks, and he only noticed them when his central vision became affected. APMPPE is bilateral (simultaneously or sequentially within a few days) in most patients, and the timing of onset for the disease is variable. Typically, it occurs within weeks to months following an antecedent infection with some of the patients having recurrences, most of which present within the first 6 months [8].
To the best of our knowledge, this is the third description of APMPPE following COVID-19 infection, the second bilateral case with the full description of the clinical course and treatment, and the first with long-lasting activity where progression to RPC was observed and where long-term steroid treatment and biological therapy was necessary. Olguín-Manríquez et al. documented a unilateral case of APMPPE occurring six weeks after a COVID-19 infection. However, the article does not mention treatment, or disclose the final outcome [9]. Fisher et al. reported a bilateral case that started 2 weeks after fever, cough, shortness of breath, myalgias and subsequent positive PCR test for SARS-CoV2. Their case had a 5-week course and complete resolution of the lesions and subretinal fluid following prednisone therapy with a starting dose of 60 mg followed by gradual tapering, and 20/20 final visual acuity on both eyes [10].
Ampiginous chorioretinitis shares similar demographics, angiographic and clinical features, and clinical course with RPC and the two entities most likely represent variants of the same disease [11, 12]. According to our knowledge, there are two cases of ampiginous chorioretinitis described in connection with COVID-19 infection. Carvalho et al. reported a bilateral case one week following a confirmed SARS-CoV-2 infection. They treated the patient with prednisolone 0.5 mg/kg daily with slow tapering over 2 months and the patient reached 20/20 vision in both eyes [13]. Tom et al. described a bilateral ampiginous chorioretinitis one week following a presumed SARS-CoV-2 infection, diagnosed with IgG antibody test without PCR. Their patient received a 60 mg oral prednisone starting dose, the retinal lesions did not progress, and at 3 weeks, azathioprine therapy (1.5 mg/kg) was initiated. After a 3-month oral prednisone taper and continuing azathioprine, the patient maintained 20/20 visual acuity in both eyes during their 10-month follow-up period [14].
Additionally, Providencia et al. described a unilateral serpiginous choroiditis 4 weeks after a PCR-confirmed COVID-19 infection. The patient received pulses of methylprednisolone 1 g/day for 3 days with subsequent tapering of the dose. Methotrexate 12.5 mg weekly was started simultaneously. During the follow-up, the patient’s vision improved from counting fingers to 20/100 with persistent central scotoma [15].
APMPPE is a rare, self-limited disorder and although the exact etiology of APMPPE remains unclear, it is thought to be an immune-mediated process with a possible infectious trigger. In order to establish the most likely cause in a given patient, detailed medical history and a methodical workup is crucial excluding all relevant infectious causes. Since the specific cause is difficult to ascertain in many cases, authors often define the disease as an idiopathic condition. We refrained from declaring our presented case idiopathic due to reasons explained earlier. Several case reports have described the association of APMPPE with various viral and bacterial infections [16,17,18]. APMPPE has also been described in connection with vaccinations i.e., varicella, hepatitis A, hepatitis B, meningococcal C, yellow fever, typhoid, and influenza [19,20,21] and recently there have been a few case descriptions following COVID-19 vaccination [22,23,24]. The disease has also been described in cases with pre-existing autoimmune and autoinflammatory conditions such as psoriasis, sarcoidosis, erythema nodosum, eczema, thyroiditis, granulomatosis with polyangiitis, polyarteritis nodosa, nephritis, ulcerative colitis, central nervous system vasculitis [1, 25, 26]. The risk of developing APMPPE may be influenced by genetics, as there have been reports of associations between certain genetic haplotypes such as HLA-B7 and HLA-DR2 [27].
APMPPE primarily affects the choriocapillaris and inner choroid, resulting in secondary changes to the retinal pigment epithelium (RPE) and outer retina [1]. The immune-mediated destruction of the RPE results in dysfunction of the blood-retinal barrier, allowing inflammatory cells and proteins to infiltrate the retina. This leads to the formation of the characteristic placoid lesions, which represent the accumulation of inflammatory cells and debris [1].
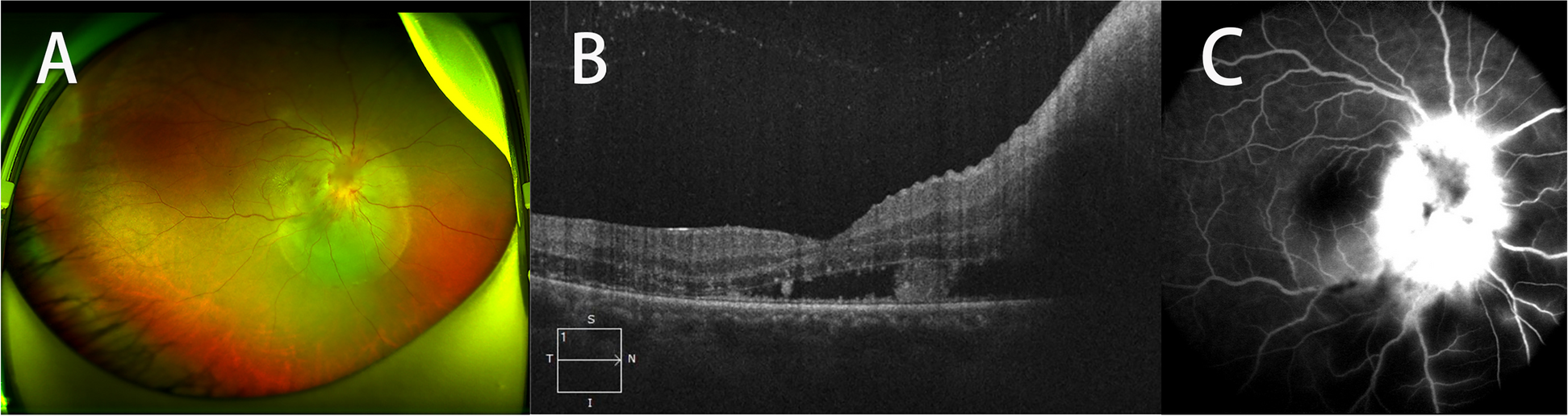
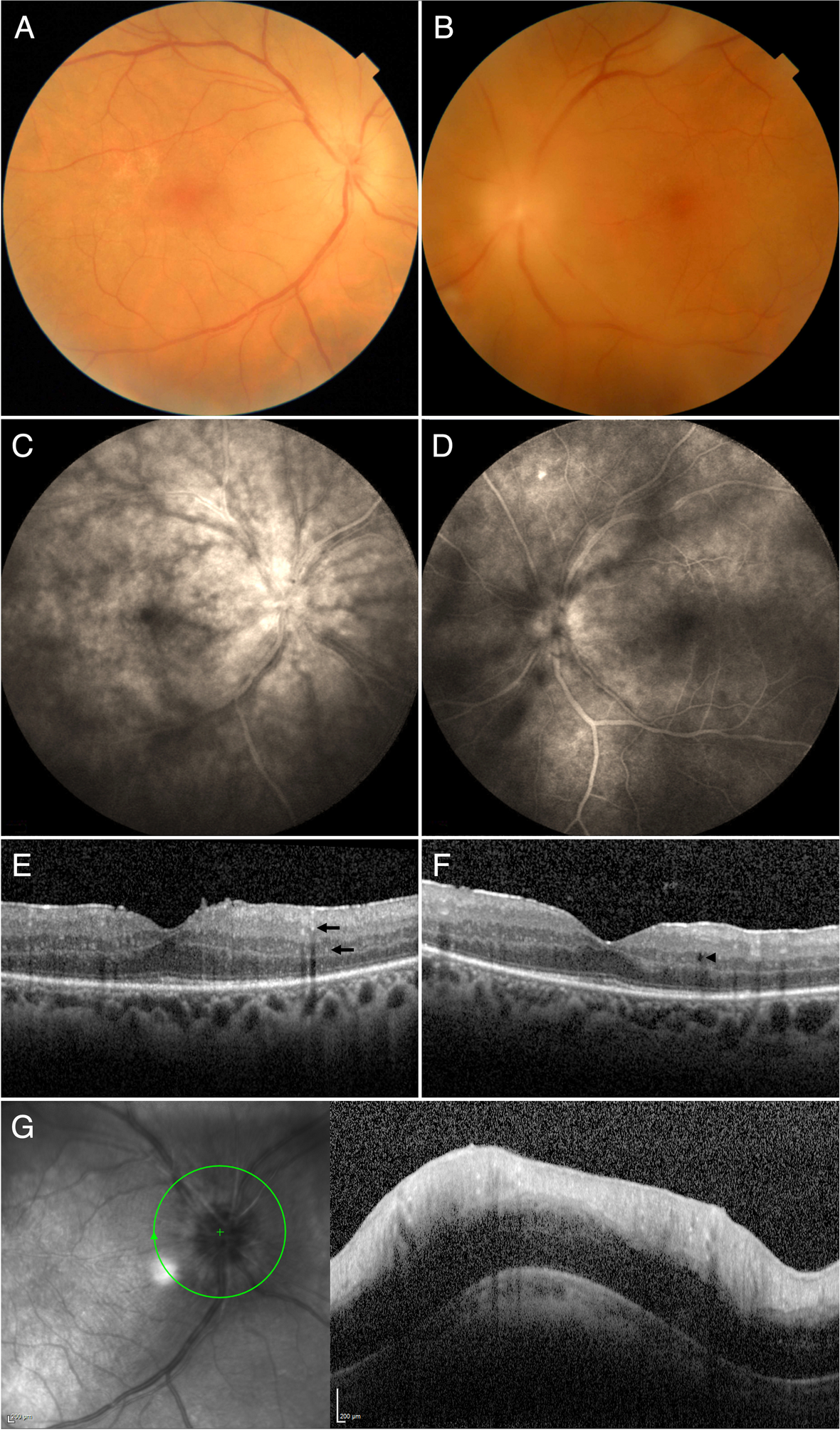
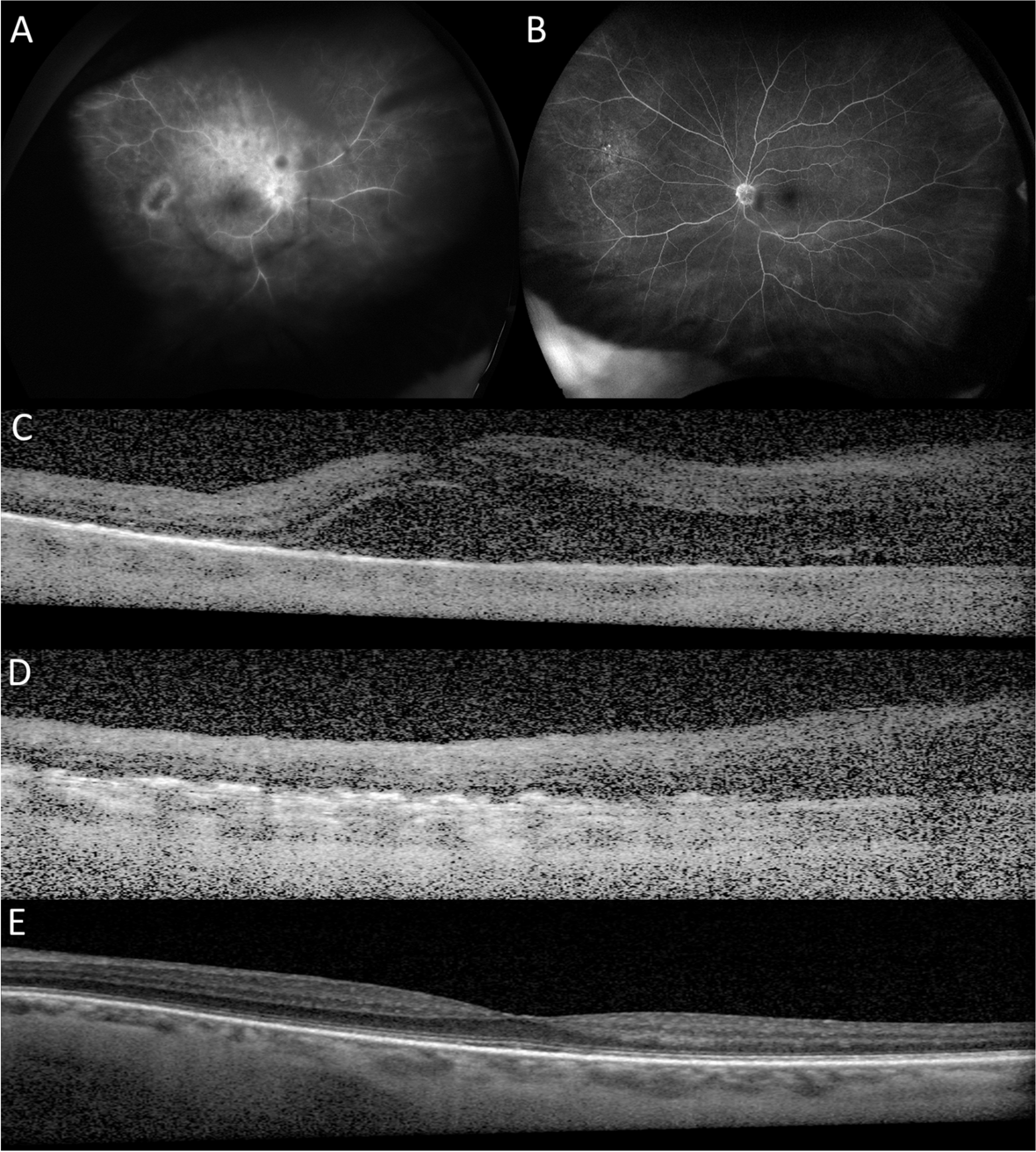
The hallmark clinical feature of APMPPE is the presence of multiple, yellow-white placoid lesions located in the posterior pole of the eye. These lesions are typically bilateral and symmetric, with a predilection for the macular area. Fluorescein angiography reveals early hypofluorescence due to blockage from the placoid lesions, followed by late staining due to leakage from the choroidal vessels. Optical coherence tomography (OCT) demonstrates hyperreflective lesions from the outer plexiform layer to the RPE often with disruption of the outer retinal layers and RPE and loss of the ellipsoid zone at the site of the placoid lesions [1]. These characteristics have been well demonstrated by the initial presentation of our patient in this report.
In contrast to APMPPE, the lesions observed in RPC are often more numerous, with a range of 50 to 100, and can be found throughout the posterior pole, mid-periphery, and far-periphery. These lesions may predate or occur simultaneously with macular involvement. RPC is characterized by the widespread distribution of both active and healed lesions scattered across the fundus, leading to a prolonged progressive and relapsing clinical course [2] The development of pigmented chorioretinal atrophy is a typical feature of RPC as the lesions heal [3].
Progression in APMPPE is not unheard of, in a retrospective analysis of a cohort of 86 patients with SC by Gupta et al., it was found that over the course of several months to years, 20 patients who initially presented with a clinical picture resembling APMPPE had progressed to SC [28].
The exact mechanisms by which SARS-CoV-2 affects the eye are still not fully understood. It has been suggested that COVID-19 may cause tissue damage by directly infecting cells through the angiotensin-converting enzyme 2 (ACE-2) receptor in the presence of transmembrane serine protease 2 (TMPRSS2) [29]. In the eye, ACE-2 receptors are expressed in the retinal ganglion cell layer, inner plexiform layer, inner nuclear layer, and photoreceptor outer segments, TMPRSS2 is expressed in multiple retinal neuronal cells, vascular and perivascular cells, and in retinal Müller glial cells [30]. Once the virus enters the eye, it can cause an inflammatory response, leading to various ocular manifestations [7, 29].
At present, there is no standardized treatment protocol for APMPPE, and mild, self-limiting cases may not require treatment. However, systemic corticosteroids have been the mainstay of treatment in most cases with neurological involvement, in cases where vision is considered threatened or when RPC is suspected [31, 32] They have been shown to result in resolution of visual symptoms and retinal lesions in the majority of patients. In addition, immunosuppressive agents, such as azathioprine, mycophenolate mofetil, cyclosporine or adalimumab, have been used in refractory cases. [12, 33, 34] Nonetheless, treatment should be tailored to each individual patient's disease course and response to therapy.
There is very limited evidence regarding the use of adalimumab in the treatment of APMPPE. However, a report of two cases of RPC by Asano et al. described adalimumab to be effective in managing the disease and allow the systemic corticosteroid to be tapered without any relapses [33] The rationale for initiating steroid-sparing therapy in our patient was the suspicion of RPC and the need for continued moderate-dose prednisolone treatment. Although methotrexate or mycophenolate mofetil are most commonly used as first-line agents in our clinic, adalimumab was chosen based on the rheumatological consultation and the discussion with the patient.





留言 (0)