
記住我



Corydalis yanhusuo is a perennial herbaceous plant belonging to the Papaveraceae family which can be found in China, Japan, Korea, and other Asian countries.1 It has been used for centuries in Chinese herbal medicine. Studies in cells and rodents have demonstrated anti-inflammatory, neuroprotective, anti-tumor, antihypertensive, cholesterol-lowering, and anticirrhotic properties, among others.2-8 Yet, there have also been human studies implicating it as a cause of drug-induced liver injury. In one study, rechallenging with kedaling tablets, which contain extract of corydalis, demonstrated elevations in aspartate transaminase, alanine transaminase, alkaline phosphatase (ALP), and γ-glutamyl transferase.9 In another study, a patient presented with jaundice and abdominal pain and had a cholestatic injury pattern. His cholestasis improved and then recurred. It was later discovered that he had been repeatedly taking a corydalis supplement.10 In fact, the active compound in corydalis, tetrahydropalmatine, has been implicated in hepatotoxicity as part of another Chinese herb called Jim Bu Huan.11–13 There are marijuana dispensaries in the United States which market a sleep aid containing both cannabis and corydalis. Corydalis is listed as an active ingredient. Here, we present 2 cases of drug-induced liver injury in patients who were taking this supplement.
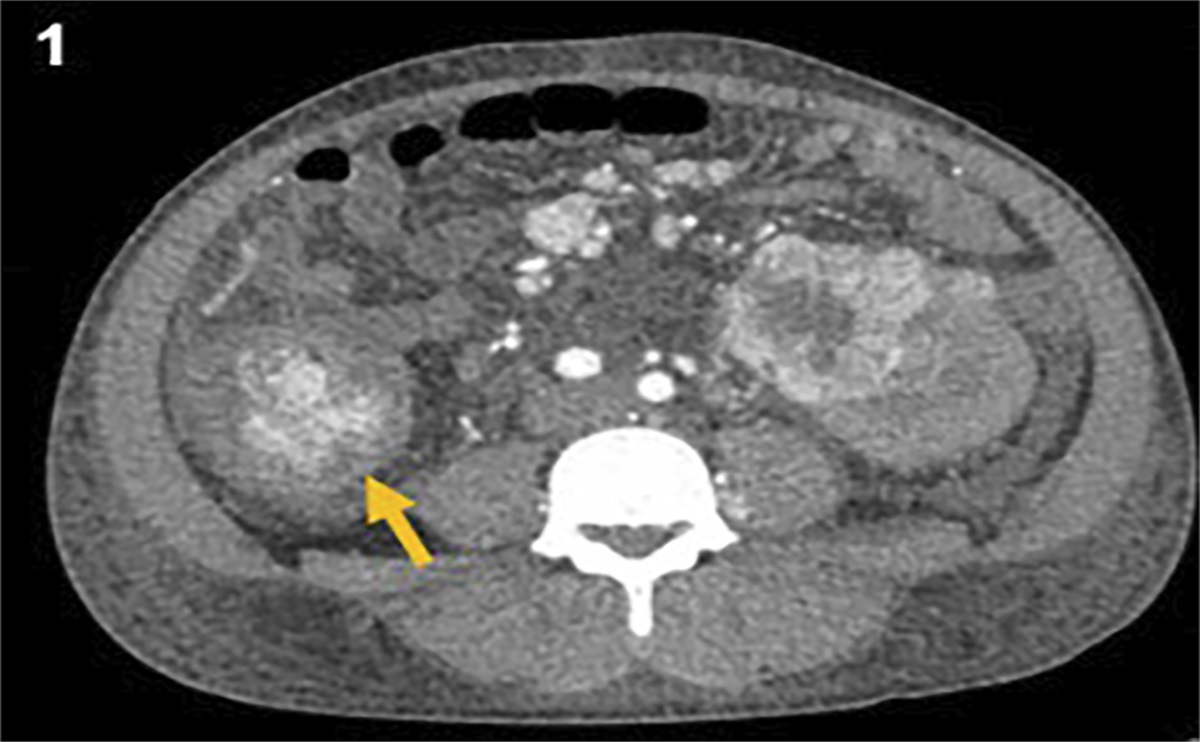
CASE REPORTSA 51-year-old woman with a history of temporal lobe epilepsy status post right temporal lobectomy taking oxcarbazepine presented to the outpatient gastroenterology clinic for abnormal laboratory values. She was referred by her primary care provider. She reported no symptoms including no weight loss, abdominal pain, jaundice, myalgia, arthralgia, or pruritus. Medications included oxcarbazepine which was increased from 75 to 150 mg twice daily for 3–5 months prior. Two months before, she had also started taking a supplement marketed for sleep which she had purchased from a cannabis dispensary. It contained corydalis as an active ingredient. She had no family history of liver disease. She did not use alcohol, tobacco, cocaine, or intravenous drugs. She had no history of blood transfusions or tattoos. Physical examination was unremarkable including a benign abdomen. Laboratory values are presented in Table 1, patient 1. Ultrasound was negative. Liver biopsy revealed severe acute hepatitis with features of ongoing and resolving portal and lobular injury (Figure 1). At the initial visit, she was instructed to continue oxcarbazepine and discontinue the supplement. Her transaminases began to resolve; however, she then restarted the supplement. Her transaminases rebounded, and she once again discontinued the supplement. Ultimately, her transaminases improved to 57 and 51 for aspartate transaminase and alanine transaminase, respectively (refer to Figure 2).
Table 1. - Pertinent laboratory values when assessing for hepatotoxicity for patient 1 and patient 2 Normal value Patient 1 Patient 2 Hepatitis A IgM Negative Negative Negative Hepatitis B core IgM Negative Negative Negative Hepatitis B surface Ag Negative Negative Negative Hepatitis C Ab Negative Negative Negative Anti-smooth muscle Ab <1:20 <1:20 1:20 Anti-mitochondrial Ab 0.0–20.0 35.3 <20.0 CMV IgM <0.9 0.2 — CMV IgG <0.9 0.9 — CMV DNA Negative — Negative EBV IgM Negative Positive Negative EBV IgG Negative Positive Positive Iron 37–175 140 229 TIBC 202–478 363 331 % saturation 15.0–55.0 38.6 49.5 Ferritin 11–336 1,025 4,923 Alpha-1 Antitrypsin 101–187 134 215 HIV 1 & 2 Ab Negative Negative Negative Tissue transglutaminase IgA <15.0 0.5 — Ceruloplasmin 16.0–39.0 26.6 32.3Ab, antibody; Ag, antigen; CMV, cytomegalovirus; EBV, Epstein-Barr virus; IgA, immunoglobulin A; IgG, immunoglobulin G; IgM, immunoglobulin M; TIBC, total iron binding capacity.
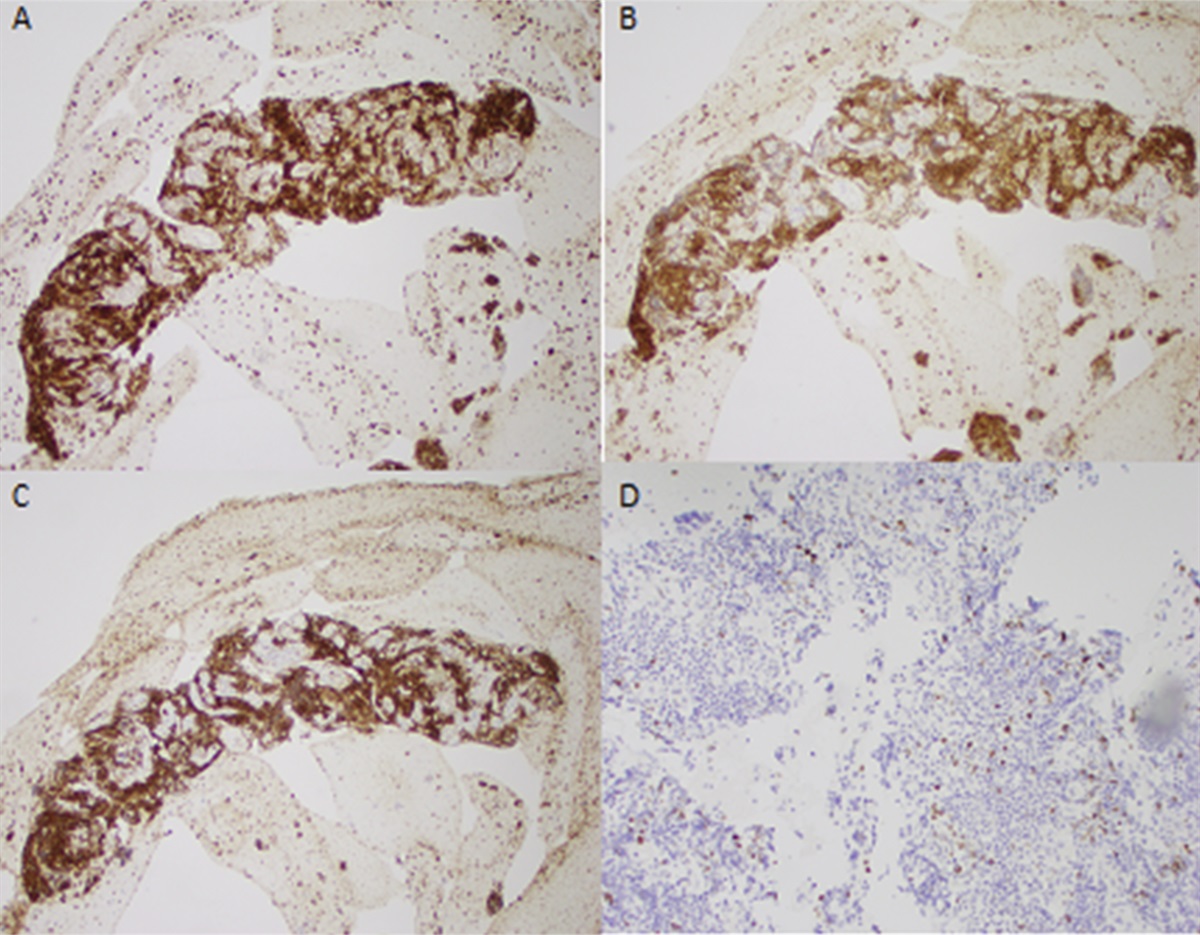
 Figure 1.:
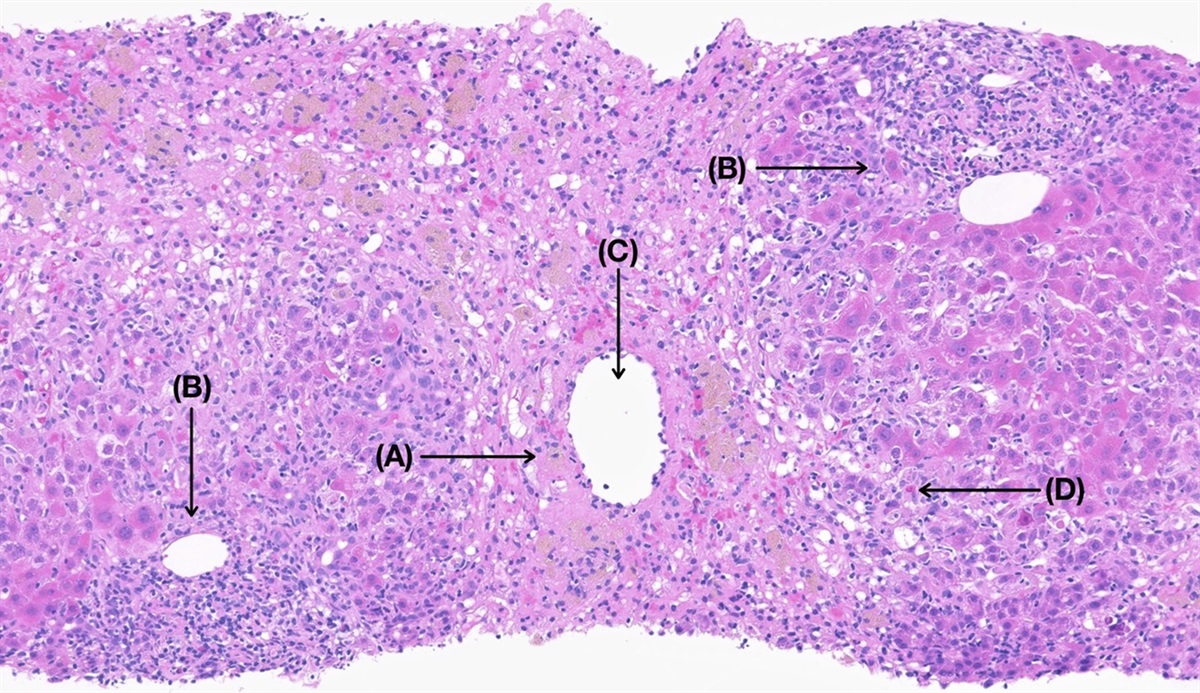
Figure 1.: Histopathologic finding of liver biopsy for patient 1. (A, B) Hematoxylin and eosin sections showing severe portal inflammation and bridging necrosis. (C) CD3 stain highlighting T-lymphocyte infiltration. (D) CD163 stain highlighting macrophage infiltration. (E, F) Trichrome and reticulin stains confirming preserved architecture.
 Figure 2.:
Figure 2.: Corydalis-induced elevation in aspartate aminotransferase (AST), alanine aminotransferase (AST), and alkaline phosphatase (ALP). Patient began taking the supplement between March 10, 2022, and February 10, 2022. February 10, 2022, is her initial presentation. She ceased consumption and then restarted between March 10, 2022, and April 10, 2022. Patient 2 began taking the supplement before May 9, 2022, which was the initial presentation. Patient 2 continued to stay abstinent from the supplement after initial presentation.
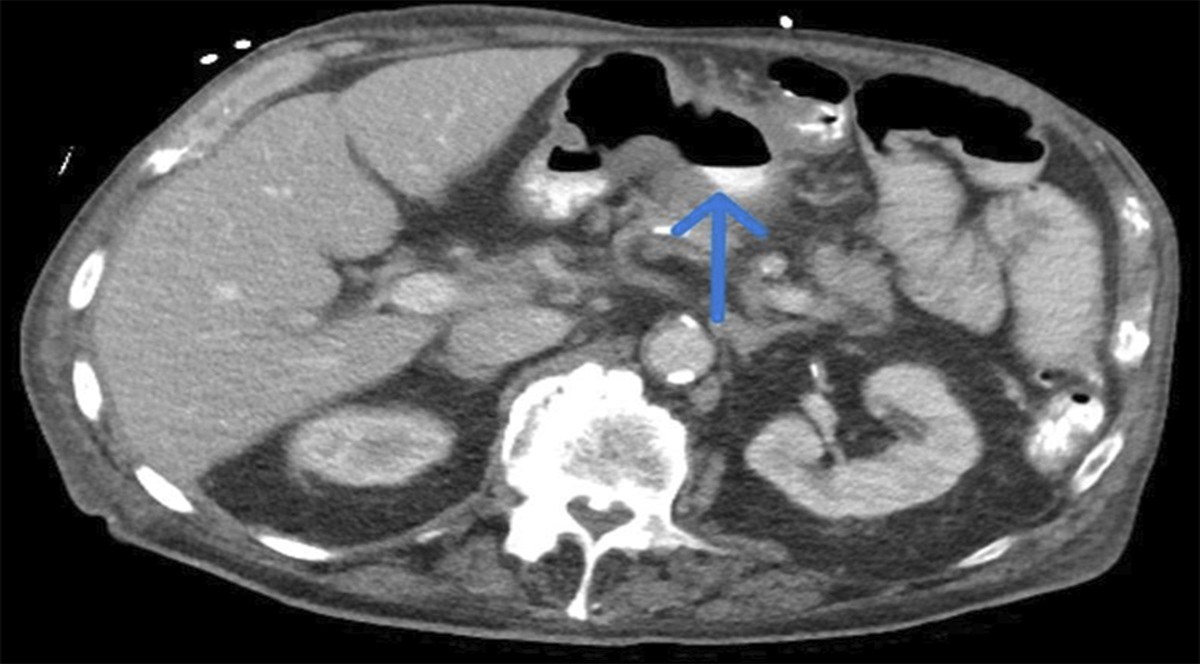
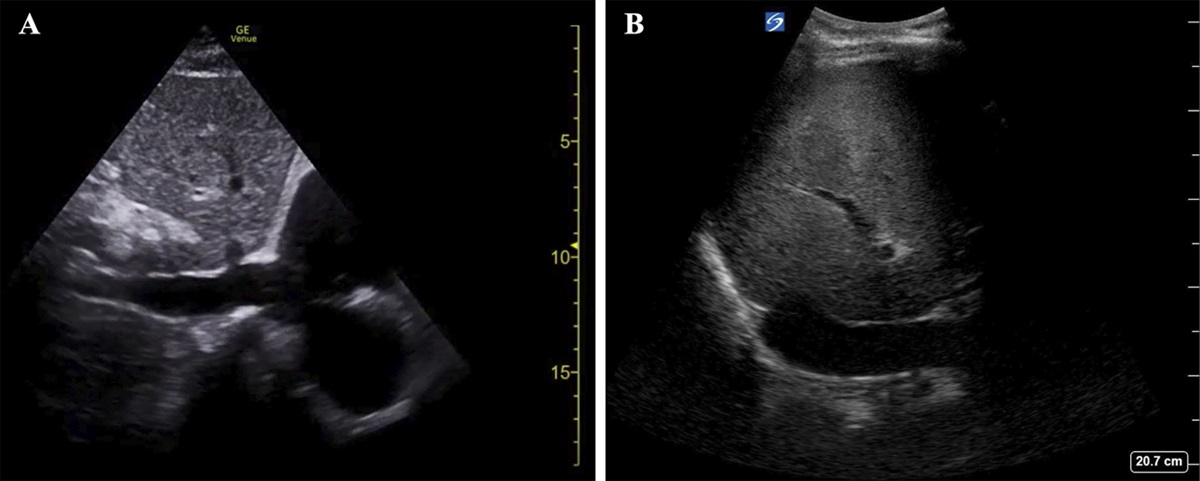
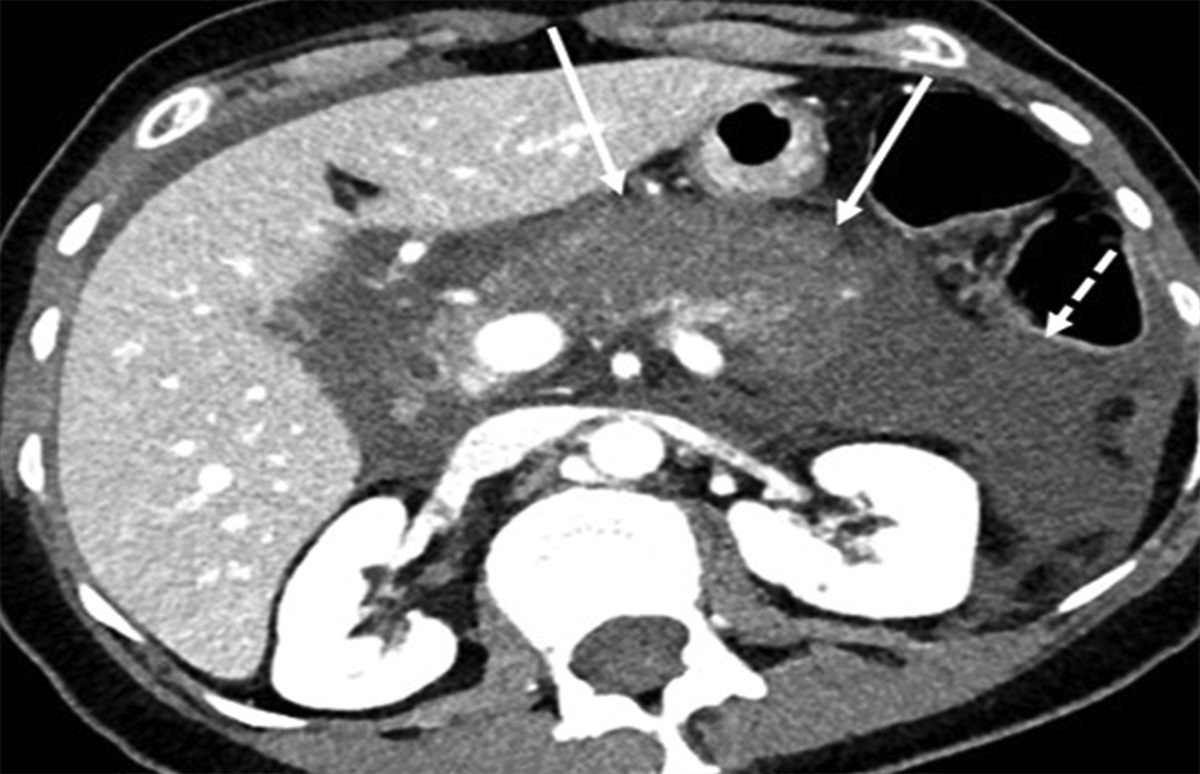
A 52-year-old man without a past medical history presented to his family medicine physician with 2 weeks of dark urine, fatigue, nausea, and nonbloody nonbilious vomiting. The patient was instructed to go to the emergency department, and he was admitted. Further history taking revealed a recent hiking trip to Colorado. Initially, he had denied any over-the-counter medications. Physical examination was notable for jaundice and a benign abdomen. Laboratory values for his 2-day admission are presented in Table 1, Patient 2. Abdominal and pelvic computed tomography with contrast was negative. Gastroenterology and infectious disease were consulted. Infectious studies were negative. Ultrasound revealed borderline hepatomegaly and echogenicity as well as mild splenomegaly. Infectious disease started him on doxycycline for possible rocky mountain spotted fever for which he completed a 10-day course. Transaminases, ALP, and bilirubin remained persistently elevated; however, the patient was asymptomatic and elected to continue work-up outpatient. It was later discovered that the patient had been using a sleep supplement containing corydalis as an active ingredient. He had taken it once per month for the past year, twice within a 6-week span, and twice immediately before admission. On discontinuance of the supplement, his laboratory values improved (refer to Figure 2).
DISCUSSIONDrug-induced liver injury may present in 3 ways. Direct hepatotoxicity occurs with agents intrinsically damaging to the liver. The injury is dose-dependent, reproducible and has a short onset on the order of 1–5 days.14 It can present with a spectrum of laboratory and histological findings. The most common form is an acute necrosis with marked transaminase elevation and normal to minimally elevated ALP and bilirubin, commonly seen with acetaminophen overdose.15,16 The other direct forms of hepatotoxicity typically have less robust elevations in transaminases, ALP, and bilirubin, and the key is in the histology. These other histological presentations include fatty liver, sinusoidal obstruction, and nodular hyperplasia.15,17,18 Direct hepatotoxicity is contrasted with idiosyncratic injury in which the agent causes hepatotoxicity not due to intrinsic toxicity but due to immune-mediated means.19,20 It is not dose-dependent, not reproducible, and onset is typically greater than 5 days. The most common form of idiosyncratic injury is markedly elevated transaminases with acute hepatitis on histology.19 Herbal agents typically fall under this category. Other idiosyncratic modes of injury include chronic hepatitis, cholestatic hepatitis, and mixed hepatitis.19,21 Finally, we have indirect hepatotoxicity in which the action of an agent causes the injury, for example, antipsychotics leading to a fatty liver and immunomodulatory agents such as anti-tumor necrosis factors reactivating hepatitis B.22,23
We present 2 patients who were both taking the same over-the-counter sleep aid containing corydalis as an active ingredient. The patient in case 1 exhibited a largely hepatocellular pattern of injury. The rise and fall of her transaminases coincided with rechallenge, implicating it as probable to highly probable drug-induced liver injury based on the Roussel Uclaf Causality Assessment Method (Table 2, patient 1).24 Her oxcarbazepine had been increased in the previous months; however, her dose was not adjusted during this time. She was immunoglobulin M and immunoglobulin G positive for Epstein-Barr virus and did not have any accompanying symptoms. Finally, she had serology consistent with a primary biliary cholangitis, yet her transaminases were markedly elevated. Interestingly, anti-mitochondrial antibody has been shown to be positive in 10% of drug-induced liver injury cases.25 In her case, she had markedly elevated transaminases with acute hepatitis on histology, consistent with idiosyncratic hepatotoxicity commonly seen with herbal agents. Her treatment was discontinuance of the offending agent with normalization of her transaminases.
Table 2. - Roussel Uclaf Causality Assessment Method values for patient 1 and patient 2 Patient 1 Patient 2 R ratio 20.5 15 Time to onset +2 +1 Course +2 +2 Risk factors 0 0 Concomitant drugs −1 or −2 0 Exclusion of other causes of liver injury +2 +2 Previous information on hepatotoxicity of the drug +1 +1 Response to readministration +3 0 Total 8–9 6Patient 1 total is consistent with probable to highly probable drug-induced liver injury, and patient 2 total is consistent with probable drug-induced liver injury.
In case 2, the patient's symptoms and laboratory values were more severe than seen in case 1, including both hepatocellular and cholestatic pattern of injury. His work-up was negative outside of a mildly elevated anti-smooth muscle antibody. His transaminases coincided with starting and stopping the sleep aid. His Roussel Uclaf Causality Assessment Method is presented in Table 2, patient 2, consistent with probable drug-induced liver injury.24 The mechanism for his injury was less clear. He had a mix of acute hepatocellular and cholestatic hepatitis seen with idiosyncratic injury. Similarly, in his case, discontinuance of corydalis resulted in full recovery.
These cases add to a growing body of evidence implicating corydalis as hepatotoxic. Furthermore, they illustrate the importance of investigating the ingredients found in supplements before use.
DISCLOSURESAuthor contributions: S. Engman: composed and edited the manuscript. F. Puello: edited manuscript. K. Khoury and D. Shah: edited manuscript and identified patients. DM Miller and K. Isidan: assembled liver biopsy images with caption. S. Engman is the article guarantor.
Financial disclosure: None to report.
Informed consent was obtained for this case report.
REFERENCES 1. Jiang L, Li M, Zhao F, et al. Molecular identification and taxonomic implication of herbal species in genus corydalis (Papaveraceae). Molecules. 2018;23(6):1393. 2. Yu Q, Wu L, Liu T, et al. Protective effects of levo-tetrahydropalmatine on hepatic ischemia/reperfusion injury are mediated by inhibition of the ERK/NF-κB pathway. Int Immunopharmacol. 2019;70:435–45. 3. Sun R, Song Y, Li S, et al. Levo-tetrahydropalmatine attenuates neuron apoptosis induced by cerebral ischemia-reperfusion injury: Involvement of c-Abl activation. J Mol Neurosci. 2018;65(3):391–9. 4. Xue F, Chen T. L-tetrahydropalmatine inhibits the progression of glioblastoma tumor by suppressing the extracellular-signal-regulated kinase/nuclear factor-kappa B signaling pathway. Curr Top Nutraceutical Res. 2020;19(2):164–71. 5. Wang X, Zhao R, Zhang H, Zhou M, Zhang M, Qiao T. Levo-tetrahydropalmatine attenuates progression of abdominal aortic aneurysm in an elastase perfusion rat model via suppression of matrix metalloproteinase and monocyte chemotactic protein-1. Med Sci Monit. 2018;24:652–60. 6. Sun C, Chen Z, Wang H, Ding K. Tetrahydropalmatine prevents high-fat diet-induced hyperlipidemia in golden hamsters (Mesocricetus auratus). Med Sci Monit. 2018;24:6564–72. 7. Yu Q, Cheng P, Wu J, Guo C. PPARγ/NF-κB and TGF-β1/Smad pathway are involved in the anti-fibrotic effects of levo-tetrahydropalmatine on liver fibrosis. J Cell Mol Med. 2021;25(3):1645–60. 8. Du Q, Meng X, Wang S. A comprehensive review on the chemical properties, plant sources, pharmacological activities, pharmacokinetic and toxicological characteristics of tetrahydropalmatine. Front Pharmacol. 2022;13:890078. 9. Wang J. Repetitive drug-induced liver injury with kedaling tablets. Clin Toxicol (Phila). 2021;59(9):853–4. 10. Kang HS, Choi HS, Yun TJ, et al. A case of acute cholestatic hepatitis induced by Corydalis speciosa Max [in Korean]. Korean J Hepatol. 2009;15(4):517–23. 11. Centers for Disease Control and Prevention CDC. Jin bu huan toxicity in adults: Los Angeles, 1993. MMWR Morb Mortal Wkly Rep. 1993;42(47):920–2. 12. Kaptchuk TJ. Acute hepatitis associated with jin bu huan. Ann Intern Med. 1995;122(8):636. 13. Brown AC. Liver toxicity related to herbs and dietary supplements: Online table of case reports. Part 2 of 5 series. Food Chem Toxicol. 2017;107(Pt A):472–501. 14. Zimmerman HJ. Hepatotoxicity: The adverse effects of drugs and other chemicals on the liver. Gastroenterology. 2000;118:984–5. 15. Hoofnagle JH, Björnsson ES. Drug-induced liver injury–types and phenotypes. N Engl J Med. 2019;381(3):264–73. 16. Larson AM, Polson J, Fontana RJ, et al. Acetaminophen-induced acute liver failure: Results of a United States multicenter, prospective study. Hepatology. 2005;42(6):1364–72. 17. McKenzie R, Fried MW, Sallie R, et al. Hepatic failure and lactic acidosis due to fialuridine (FIAU), an investigational nucleoside analogue for chronic hepatitis B. New Engl J Med. 1995;333(17):1099–105. 18. DeLeve L, Shulman H, McDonald G. Toxic injury to hepatic sinusoids: Sinusoidal obstruction syndrome (veno-occlusive disease). Semin Liver Dis. 2002;22(1):27–42. 19. Chalasani N, Bonkovsky HL, Fontana R, et al. Features and outcomes of 899 patients with drug-induced liver injury: The DILIN prospective study. Gastroenterology. 2015;148(7):1340–52.e7. 20. Kullak-Ublick GA, Andrade RJ, Merz M, et al. Drug-induced liver injury: Recent advances in diagnosis and risk assessment. Gut. 2017;66(6):1154–64. 21. de Boer YS, Kosinski AS, Urban TJ, et al. Features of autoimmune hepatitis in patients with drug-induced liver injury. Clin Gastroenterol Hepatol. 2017;15(1):103–12.e2. 22. Kumra S, Herion D, Jacobsen LK, Briguglia C, Grothe D. Case study: Risperidone-induced hepatotoxicity in pediatric patients. J Am Acad Child Adolesc Psychiatry. 1997;36(5):701–5. 23. Di Bisceglie AM, Lok AS, Martin P, Terrault N, Perrillo RP, Hoofnagle JH. Recent US Food and Drug Administration warnings on hepatitis B reactivation with immune-suppressing and anticancer drugs: Just the tip of the iceberg? Hepatology. 2015;61(2):703–11. 24. Roussel Uclaf Causality Assessment Method (RUCAM) in Drug Induced Liver Injury. (https://www.ncbi.nlm.nih.gov/books/NBK548272/) (2019). Accessed August 10, 2023. 25. Weber S, Benesic A, Buchholtz ML, Rotter I, Gerbes AL. Antimitochondrial rather than antinuclear antibodies correlate with severe drug-induced liver injury. Dig Dis. 2021;39(3):275–82.
留言 (0)