
記住我

Mental illness among prison inmates is a common and prevailing issue across the world. The occurrence rate of mental health conditions and suicide among the prison population is overrepresented compared with the general population.1,2 In Canada, one in seven male federal inmates has major depression or psychosis, with similar rates among inmates on a global scale.3,4 Rates of suicide are 3 to 6 times higher in male inmates when compared with community populations, with many studies indicating that one in seven people in custody have attempted suicide.5,6
Incarcerated women have higher rates of common mental health problems than male inmates, and higher rates of comorbidities.7
The increasing numbers of mentally ill inmates in North America was a trend observed first in the latter part of the 20th century and has been correlated with the deinstitutionalization movement.8 Those with mental illness often intersect with other marginalized populations, including racialized groups,9 as being over-represented in correctional institutions. As a result, despite there not being hospitals, correctional institutions find themselves as one of the most common mental health care providers in North America.10 Although not being recognized health care professionals, correctional officers (COs) assume the role of quasi-mental health care providers, often receiving little-to-no formal education in mental health.11
Traditionally, COs are trained to maintain security, enforce rules, and impose punitive sanctions on inmates who misbehave.12,13 Thus, COs are often inadequately prepared when required to interact with inmates with mental illnesses and de-escalate related situations.11–13 As a result, COs may face professional tensions—although they are not mental health staff, they are often confronted with situations where they must manage mental health behaviors.12 Recent events in the media have highlighted the negative mental health outcomes prevalent in current correctional systems. For example, the Ashley Smith inquest in Canada revealed that a CO was reprimanded for not intervening when an Aboriginal teenage inmate attempted suicide.14
Inadequate management of inmate mental health can harmfully affect corrections systems and inmates. In the corrections system, inmates face significant stressors such as overcrowding, separation from family and social supports, fear of assault, and limitations on privacy.12 These challenges can overwhelm inmates with mental illnesses, and given their already limited coping skills, may result in poor adaptation to the prison environment and greater incidences of misconduct.12,15 Misconduct and mental health crises, such as attempted or completed suicides, can impair prison operations by diverting staff time and resources.12 There is a great need to resolve the disconnect between correctional systems and the mental health needs of inmates.
COs are in a unique position to contribute toward mental health care. Education could improve the mental health, risk management, and humane treatment of inmates because COs would be empowered with tools to recognize risk related to mental health needs (eg, suicide risk, psychosis) that may require care or health care referrals. As well, they would be better able to provide mental health supports to inmates, such as learning tools (eg, de-escalation skills, counselling skills) to manage mental-health–related behaviors. In addition, mental health education could increase collaboration between COs and health care staff by providing a common language for discussing inmates' observed mental states and behaviors. This is especially important given that COs spend more time with inmates than health care professionals do, and may be the first to observe signs of changes in inmate mental health.12 As such, custodial supervision and mental health treatment support should not be viewed as mutually exclusive. Thus, it is important to develop best practices regarding how to educate and empower correctional staff regarding the mental health of inmates. If one considers the quasi-health professional role that COs play, a “type 1” educational problem16 comes into view: they lack the knowledge, skills, and attitudes necessary to meet the mental health needs of “clients” under their “care.”
Currently, there is limited research on the value of mental health education programs for COs.11,17 Although some programs do exist, as far as we are aware, there have been no prior reviews of this literature. Therefore, the goal of this study is to review the current state of this literature and explore the factors related to the effectiveness of mental health education programs. These findings could contribute toward best practice guidelines for future mental health training programs for COs.
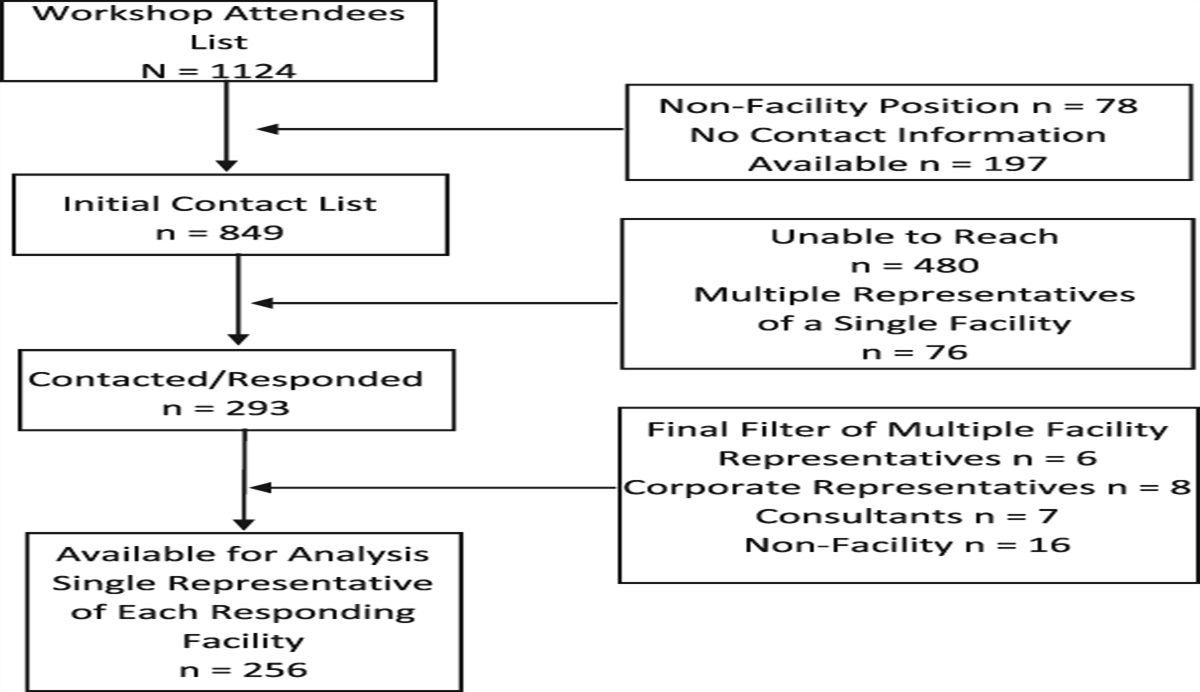
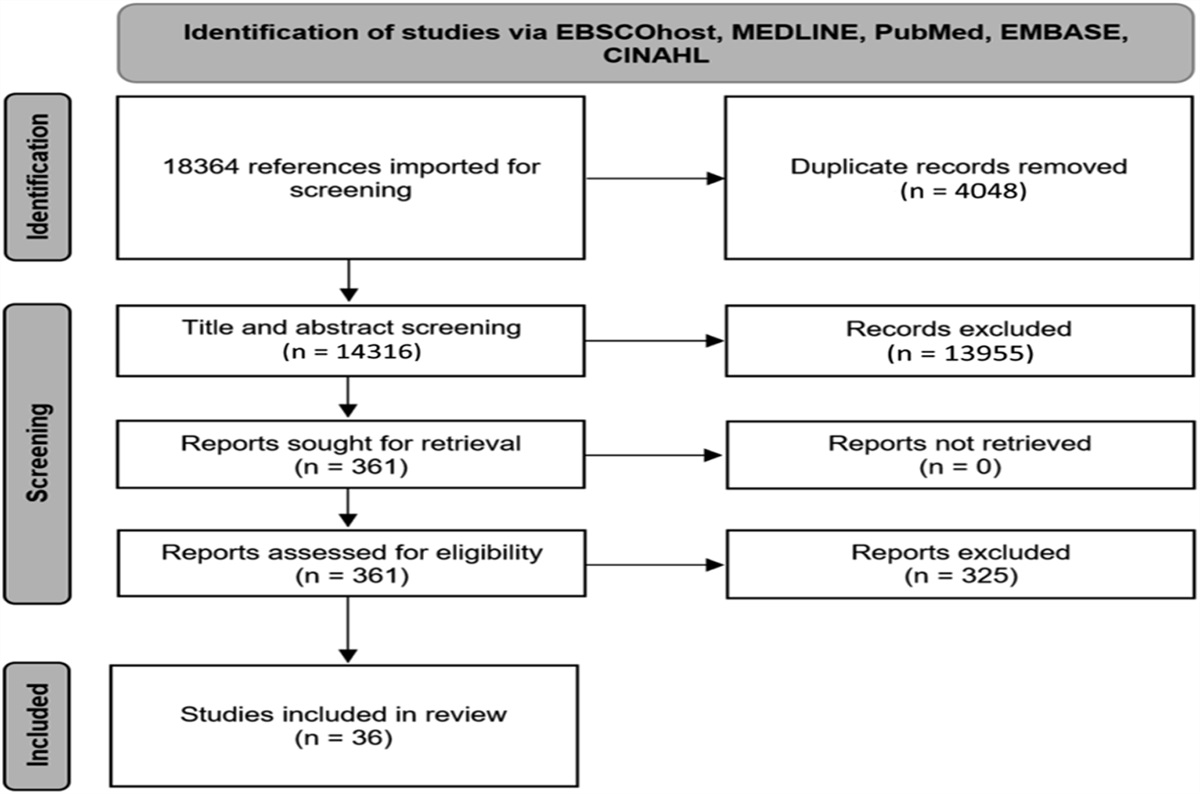
METHODSThe authors reviewed the published scientific literature to ascertain mental health education programs that are specifically designed for COs, and identify common themes related to program effectiveness. We focused on programs that had outcome measures. After discussions with stakeholders, we identified a change in CO knowledge, skills, and attitudes, or an improvement in the mental health of inmates, as being relevant. We used a narrative approach to understand themes in the literature, and to identify gaps in knowledge in the area. To increase the methodological rigor of the study, and to ensure diverse sources, we used a systematic approach to study selection and thematic analysis.18 A preliminary search was undertaken to verify that no similar research has been published. To improve on the methodology of a narrative review, such as avoiding selection bias or a lack of diversity in sources, we used components of a systematic review from the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA).19 (Fig. 1).
 Figure 1.:
Figure 1.: Flow diagram of literature search process.
The search strategy was developed with the assistance of a research librarian (S.B.). Searches were conducted of the following electronic databases: CINAHL, Criminal Justice Abstracts, EMBASE, Medline/Medline In-Process & Other Non-Indexed Citations/Medline E-Pub Ahead of Print, National Criminal Justice Reference Service (NCJRS) Abstracts, PsycINFO, Scopus, and Web of Science. A Medline search strategy was constructed to identify studies with the use of free text word and MESH terms, which was then modified for each database accordingly. All databases were searched since inception and there were no publication types or language restrictions. Searches were completed in July 2020. Searches were supplemented by also scanning the reference lists of identified relevant studies. Duplicates were removed.
Any studies that fulfilled the following inclusion criteria were included for further review: systematic reviews, randomized controlled trials, nonrandomized trials with a before-and-after measure, observational epidemiologic studies with a control group, studies without a controlled group, case reviews, and mixed methods. The search was inclusive of articles that described interventions globally. An initial sample revealed that the few studies in languages other than English were not on topic; therefore, we decided to review only English language studies. We excluded letters, commentaries, opinion pieces, and dissertations.
Two reviewers (J.Q. and R.M.) completed a single review of titles and abstracts with quality checks, followed by a duplicate and independent review of all full texts that were selected. Flow of information is reported in the PRISMA diagram (Fig. 1).
A data extraction framework was created to extract key characteristics from the selected studies. Studies were evaluated using the Oxford Centre for Evidence-Based Medicine Levels of Evidence scale.20 Because of the lack of quantitative or high-quality studies, we conducted a thematic analysis of the programs. Papers were reviewed by three team members with relevant expertise: a continuing professional development (CPD) lead (S.D.), a forensic psychiatrist (J.Q.), and a correctional psychiatrist (R.M.). This approach added interpretive rigour via researcher triangulation21 and used a conventional content analysis approach22 to categorize the studies into general mental health, counselling skills specific, and suicide prevention programs, and further to describe the key characteristics and findings of each program within those categories.
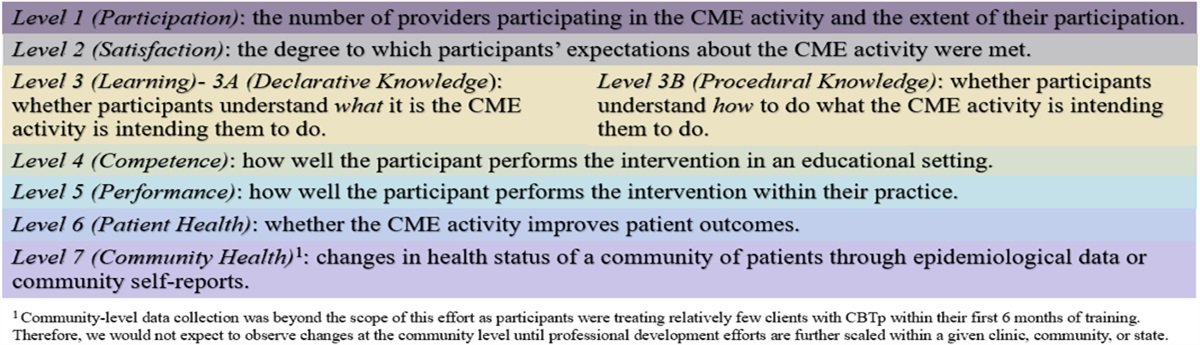
The Moore expanded outcomes framework is used in developing and evaluating continuing medical education by assessing learners and evaluating instructional activities against seven levels of outcome.23 Outcome measurements assist in identifying the strengths and limitations of educational activities. This study adapted the framework to include outcomes relevant in a correctional setting (Table 1) and evaluated the quality of the CO mental health education programs (Supplemental Table 1, https://links.lww.com/JCEHP/A205). One of the study authors (K.S.), an advanced practice clinical leader with specialized training in education, used this framework to evaluate the quality of the CO education programs.
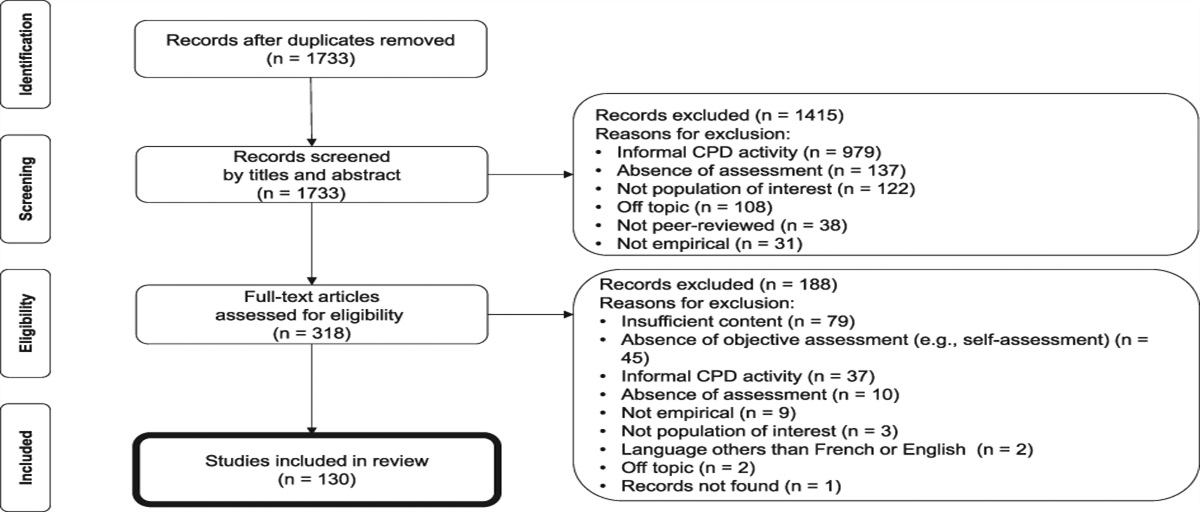
TABLE 1. - Adapted Moore's Outcomes Framework Outcomes Framework Description Level 1 participation Number of correctional staff who attended the mental health education program Level 2 satisfaction The degree to which the expectations of the participants about the setting and delivery of the mental health education program were met Level 3A learning: Declarative knowledge The degree to which participants state what the mental health education program intended them to know Level 3B learning: Procedural knowledge The degree to which participants state how to do what the mental health education program intended them to know how to do Level 4 competence The degree to which participants show in an educational setting how to do what the mental health training program intended them to be able to do Level 5 performance The degree to which participants do what the mental health education program intended them to be able to do in their practice Level 6 inmate mental health The degree to which the mental health status of inmates improves because of changes in practice behavior of participants Level 7 improved mental health for inmates The degree to which the mental health status of all mentally ill inmates improves in the correctional system Adapted from Moore Framework to include correctional officers (instead of physicians), inmate mental health (instead of patient health) at Level 6, and improved mental health for inmates (instead of community health).23One thousand twenty three unique research papers were identified by the literature search. Nine hundred fifty eight studies were excluded on screening the titles and abstracts. Sixty five full articles were assessed for eligibility; 11 were included in the final analysis and are listed in https://links.lww.com/JCEHP/A221. All studies were considered to be of low quality (level 4) as per the Oxford Centre for Evidence-Based Medicine Levels of Evidence Scale.20 All of the studies achieved Level 3 outcomes on Moore outcomes framework (Supplemental Table 1, https://links.lww.com/JCEHP/A205).
General Mental Health Education ProgramsWalsh and Freshwater evaluated the delivery of a mental health education program on 24 prison staff.24 Staff were predominantly prison officers although other disciplines and nursing staff also attended. 18 hours of content were delivered in modules over three consecutive days by a facilitator with relevant experience working in prisons. Content included six modules covering mental health education and practical communication skills. Teaching methods included didactic lectures, discussions, and participant workbooks. The program was evaluated with a post-training questionnaire. Most participants reported attitudinal changes (eg, they would act less judgmentally) and increased confidence in responding to inmates with mental health issues. Participants also fed back that the practical aspects, professionally credible facilitator, and interactive nature of the course supported their learning.
Parker24 evaluated the effectiveness of an education program delivered to 48 to 57 COs working in a prison-special housing (“supermax”) unit. The program consisted of weekly 2-hour sessions over 5 weeks delivered in modules by facilitators with relevant experience (eg, medical school psychiatry faculty, basic science faculty, a prison administrator, consumers, and family members). Teaching methods included didactic lectures, discussions, and role plays. When compared with the 9 months preceding the training program, results showed the total number of incidents reported, use of force by COs, and battery by bodily waste decreased in the 9 months after the program.
The Memphis Crisis Intervention Team (CIT) program is a 40-hour course commonly used for law enforcement officers in the United States.13 The curriculum includes information about mental illness and education in crisis response skills. CIT had been delivered previously on a small scale to COs, who found interacting with consumers and their families particularly useful.13 Davidson evaluated the CIT program's effectiveness when delivered to 100 COs and 179 law enforcement officers.13 Participants' knowledge of mental illness, self-efficacy when responding to mental health crises, and perceptions of de-escalation skills were measured with pre-post questionnaires and 1 month after the program had ended. Results indicated that similar to law enforcement officers, COs' knowledge, self-efficacy, and perception of verbal de-escalation skills improved immediately after the program. One month after the program, there was a significant decline in participants' self-efficacy and perception of verbal de-escalation skills compared with immediate postprogram results, but there was no change in participants' knowledge. Davidson suggested placing emphasis on role-plays in the curriculum, as opposed to didactic content, to improve outcomes.13 However, the participants who completed the 1-month follow-up questionnaire were not representative of the sample population that participated in the program, so these results may not be generalizable to the entire law enforcement and correctional population.
Maltman and Hamilton investigated the effects of a 2-hour personality disorder awareness workshop for 67 prison staff, most of whom were COs.25 Teaching methods included didactic lectures, discussions, and group activities. Twenty six staff responded to a questionnaire that was distributed before the workshop and 2 months postworkshop. The questionnaire measured attitudes related to interacting with people with personality disorders (eg, security vs. vulnerability, enjoyment vs. loathing, purpose vs. futility). Results indicated that staff's attitudes regarding security versus vulnerability improved, but attitudes in all other domains remained the same.
DeHart and Iachini evaluated the impact of a 3-hour trauma-centered mental health curriculum delivered to 50 COs from 20 prisons in the same department of corrections.11 Content was delivered with short didactic lectures, videos, and group activities. Twenty nine COs with prior education in crisis intervention attended one session and were separated from 21 COs without prior education who attended a different session. More female and African American COs attended the program than is representative of the general CO population. Results from pre-post questionnaires indicated that COs' knowledge of trauma and trauma-related corrections increased after the program. There was no difference in the knowledge gained by those with or without prior crisis intervention education.
Melnikov and colleagues26 evaluated an education program designed to reduce stigmatization of inmates with mental illness on 83 COs in Israel. The 48 hours program spread over 2 weeks, included didactic lectures, case reviews, general and panel discussions, peer supervision, simulations, and observational education in psychiatric wards. Emotional aspects of the learning were reviewed during peer supervision. Results from pre-post questionnaires indicated that stigmatizing attitudes decreased, and perceived knowledge of mental illness and its management improved. There were no differences in outcomes based on level of education, job seniority, or place of birth.
One CO mental health program achieved Moore level 6,24 2 programs achieved Moore level 5,13,26 and three programs achieved Moore level 411,24,25 (Supplemental Table 1, https://links.lww.com/JCEHP/A205).
Counselling Skills-Specific ProgramsDoran and colleagues examined whether 222 Division of Juvenile Justice (DJJ) employees' motivational interviewing (MI) skills improved following a 3-day basic and a 2-day advanced MI education session.27 The content and teaching methods were not disclosed. The elapsed time between the basic and advanced sessions was 6 months, but varied among participants. DJJ employees' jobs were classified across multiple disciplines, including COs, correctional counsellors, psychologists, physicians, and case management specialists. MI skill acquisition was measured by performance on a video assessment of a simulated encounter before and after attending the advanced education session. Results indicated that employees' MI skills improved after attending the advanced education session, especially in those who were younger and had higher levels of education. MI skill acquisition also improved when less time elapsed between attending the basic and advanced sessions, with the authors recommending no more than 9 months between the two.27 Job classification, motivation to use MI, and perceived efficacy of MI were not associated with any differences in skill acquisition.
Jen Der Pan and colleagues examined whether 106 preservice Taiwanese COs' counselling skills improved after a 10-week Competency-Based Counselling and Training Program (CBCTP).17 COs were divided into two groups: 44 participated in the CBCTP and 62 received professional skills education, but not the CBCTP. Groups were organized based on COs' availability for session times and were not randomized or matched. Both groups attended 3-hour weekly sessions with additional work assigned between sessions. CBCTP teaching methods included discussions, skills demonstrations, role-plays, and feedback. Results from pre-post questionnaires indicated that COs who attended the CBCTP had a greater understanding and mastery of counselling skills than those who did not. Improvements were not significantly associated with gender, educational background, or work experience.
One counselling skills-specific program achieved level 5 on the Moore outcome framework17 and one achieved level 427 (Supplemental Table 1, https://links.lww.com/JCEHP/A205).
Suicide Prevention ProgramsSkills-Based Training on Risk Management (STORM) is a suicide prevention program developed for front-line National Health Service (NHS) staff in England and Wales intended to provide staff with skills to assess and manage suicide risk in interview situations. Each of the four modules includes didactic, videotaped role play, and small group feedback components. STORM was adapted for 183 prison staff at two adult and one juvenile male establishments in the HM Prison Service (U.K.).29 Most staff were discipline workers; others worked in departments such as health care or psychology. Staff's attitude toward suicide prevention, knowledge of suicide risk issues, and confidence in their ability to implement suicide prevention were evaluated with pre-post questionnaires (n = 161) and 6 to 8 months later (n = 69). Results indicated that staff's attitudes, knowledge, and confidence in suicide prevention improved immediately postprogram. However, their knowledge and confidence significantly decreased in follow-up, but were still significantly higher than before they had participated in STORM.
Sovronsky and Shapiro described the effects of a New York State-wide suicide prevention training program delivered to police and COs at over 300 correctional facilities in the 1980s.30 The program was delivered in an 8-hour, single-day session and included didactic lectures, discussions, an interactive video, a training manual, and a pocket reference guide. A major component of the education involved educating officers to identify mental illnesses and familiarizing them with terminology used by mental health professionals. The program's effectiveness was measured with pre-post knowledge tests, questionnaires, interviews, and observations. Results indicated that officers' confidence and knowledge of identifying and managing suicidal patients increased after education, and most officers positively rated the program. However, the authors indicated that the session was not long enough to adequately cover the material in the described modalities; some discussions on the topics may have been restricted and delivered suboptimally. Officers who failed the post-test were required to receive additional education.
Cutler and colleagues evaluated whether a suicide awareness program for prison staff could improve staff's knowledge and attitudes of prisoner suicide and self-injury.31 53 uniformed and nonuniformed prison staff, primarily tasked with delivering programs at an institution in Suffolk, participated in the program. Each module lasted 2.5 hours; the authors did not disclose the number of modules or the time period over which they were held. Pre-post questionnaire results indicated that staff's knowledge and attitudes of prisoner suicide and self-injury improved after the program.
Two suicide prevention programs achieved level 5 on the Moore outcome framework29,30 and one program achieved level 3b31 (Supplemental Table 1, https://links.lww.com/JCEHP/A205).
DISCUSSIONIn our study, we advance the notion that COs function as pseudo-health care workers by circumstance, in need of education to bolster that aspect of their undeclared role, and thus “fix” a “problem” (here, an educational one).16 It is important to note, however, that this paradigm has inherent challenges. Critical viewpoints, such as that held by the abolitionist movement, have advanced the notion that prisons are in fact not broken, but rather ultimately social structures that punish racialized and disabled populations by (perhaps unconscious) intent.32 We accept such a lens has merit. However, prisons currently remain a primary “care provider” for psychiatric patients in North America, for better or worse, and improving the care they receive where they are is a worthy aim regardless.
The purpose of this study was to review the current state of the literature on mental health education programs for COs and identify factors contributing to their effectiveness. Despite the low quality of the articles, all the studies reviewed reported effective mental health education programs.11,17,29 Common themes related to the programs' effectiveness include applicability to all COs, information retention, program facilitators, and teaching methods.
COs' prior mental health knowledge, education background, and work experience were not associated with improvement in knowledge, skills, and attitudes after attendance.11,17,26,27 Doran and colleagues observed that COs' motivations to use MI and perceived efficacy of MI were not associated with MI performance.27 It is possible that mental health education programs can be useful for all COs, regardless of past experiences or pre-existing attitudes toward education. It may be that even those less motivated for education will improve upon program completion.
In follow-up evaluations of program efficacy, researchers noted a decline in COs' knowledge, skills, and attitudes.13,29 However, despite observing a decline when compared with immediate posteducation, COs still performed significantly better in follow-up when compared with before attending the program.29 Although COs may forget aspects of training over time, critical information may still be salient and reflected in their behavior. To combat this decline, some researchers have suggested increasing the frequency of training sessions to every 9 to 18 months, because COs show greater improvements when less time passes between sessions.27,29 Other suggestions to maintain gains include modifying sessions to incorporate more experiential learning (ie, more role-plays and group discussions) and assigning new attendees to work with veteran attendees after completion.24,29 However, future research should investigate why improvements decline over time to decrease their effects.
Course facilitators' backgrounds varied, including prison employees, physicians, and mental health consumers and their relatives.11,24,27 Facilitators with prison experience seemed particularly important, because they made the curriculum more applicable to COs' work.24 In one study including a clinical facilitator, COs requested to be taught by another CO in future iterations of the program.11 Future programs should consider incorporating facilitators with prison experience, mental health consumers, and relatives to improve effectiveness.
Program teaching methods varied and included some or all of didactic lectures, role-plays, videos, workbooks, and large group discussions.17,28,30 Based on CO feedback, researchers reported that practical skills and experiential components (ie, group feedback, role-plays) were more effective and better received than didactic content.24,29 Future programs may benefit from incorporating experiential components.
Current CO mental health education programs seem to improve COs' knowledge, attitudes, and skills related to mental health. Program strengths include their applicability toward COs, regardless of pre-existing attitudes or prior experience, facilitators with prison and mental health experiences, and incorporating experiential teaching methods. However, there is little research combatting the decline in gains after education or measurement of the impact of education on behavior or practice.
The existing CO mental health programs achieved levels 1 to 5 of Moore Expanded Framework; however, only one study achieved level 6,24 Data used to measure levels 1 to 5 of the framework consisted mostly of pre-post tests and self-report measures. Future mental health programs for CO's should aim to integrate objective measures of data, such as, observed performance to allow for a more effective evaluation of the education. In addition, future mental health programs should aim to achieve levels 6 & 7 on the Moore taxonomy with the integration of data measures that focus on patient outcomes to better understand the impact of the education on patient mental health with the integration of CPD best practices.
CPD has shown to have a positive impact on participant performance and patient outcomes,33 with the greatest impact on knowledge, less of an impact on performance, and the lowest impact on patient outcomes.34 CO mental health education programs could potentially improve inmate mental health; however CPD literature states it is difficult to measure the link between CO mental health education and the mental health of inmates and whether the improved outcomes are linked to a change in COs behavior.28
To evaluate whether CO mental health education programs have the potential to improve inmate mental health, program planners can use the Moore Expanded Outcomes framework by identifying, planning, and assessing for inmate mental health. To achieve Moore higher outcomes ‘education planning focused on the outcomes must occur so that the outcomes can be expected to happen’.35
Once the desired outcomes have been identified, COs should be engaged by planners to identify their learning needs through a needs assessment.35 A needs assessment plays an integral role in CPD planning by identifying what knowledge, skills, and attitudes the COs need to improve their performance.23 The needs assessment guides the content of the program and informs instruction to meet identified needs. Multiple educational activities that are focused on identified learning needs of COs are positively associated with behavior change.36
The program instructional design should be guided by best practices based on the learning needs identified through the needs assessment and the desired outcomes indicated through the gap analysis.35 CPD activities that use multiple educational techniques are more effective than those that use a single technique. Interactive methods are most effective at improving performance and patient health outcomes and didactic materials alone have no beneficial effect on these outcomes.
Ongoing evaluation of CO mental health education interventions is integral to ensure that it is reaching its intended outcomes. The CO mental health education programs seem to increase knowledge and meet participants' learning objectives. This can be easier to capture using summative evaluations administered at the end of an educational intervention to determine whether the objectives were achieved.23 Measurement of improved inmate mental health can be more challenging to measure, formative evaluation during an educational activity can help to determine whether the desired outcomes have been achieved.23 Future planning of CO mental health education programs should consist of formative and summative evaluation and identify at the onset of delivery, which outcome measures will be used to determine whether the intended outcomes are achieved by the CPD activity.
There are several limitations that may affect the results in the present review. Although numerous databases were searched for this review, it is possible that some correctional mental health training education may not be studied or published, which would exclude them from this review. Further, studies were limited in their outcome measurement, which were largely pre-post evaluations designed by each research team. No consistent tools were used across studies, and few studies included control groups.17,24 Few articles assessed whether the education programs translated to behavioral changes once COs returned to work.13,24,27 Only the Parker24 study measured inmate-related outcomes. It may be possible that some programs are perceived as more successful than they truly are. This may alter perceptions of how to improve CO's knowledge, attitudes, and skills related to the mental health of inmates.
CONCLUSIONThis narrative review represents the first attempt, to our knowledge, to systematically integrate the available literature on mental health education programs for COs and their impacts. With that in mind, the scant literature in this area should serve as a rallying cry to improve formal education programs for COs in this area. Future CO mental health education would be enhanced by the integration of CPD approaches into curriculum design and a more robust evaluation to measure how the education affects the overall mental health of inmates. More rigorous program development and evaluation is necessary to evaluate how these themes relate to the mental health outcomes of inmates. Longer-term follow-up is needed to understand the longitudinal impact of the education on knowledge, attitudes, and skills and the health outcomes of inmates.Lessons for Practice ■ Given the overrepresentation of mental illness among inmates, COs function as pseudo healthcare professionals, currently operating without best practices and standards for evaluation of mental health education programs. ■ Mental health education for COs is linked to improved attitudes, knowledge, and skills; however, longer-term evaluations are needed to understand the decline in improvements posteducation. ■ The design and evaluation of future CO mental health education should focus on understanding the link between mental health education and inmate mental health outcomes.
REFERENCES 1. Lamb HR, Weinberger LE. Persons with severe mental illness in jails. Psychistr Serv. 1998;49:483–492. 2. Simpson AF, McMaster JJ, Cohen SN. Challenges for Canada in meeting the needs of persons with serious mental illness in prison. J Am Acad Psychiatry Law. 2013;41:501–509. 3. Brink JH, Doherty D, Boer A. Mental disorder in federal offenders: a Canadian prevalence study. Int J Law Psychiatry. 2001;24:339–356. 4. Fazel S, Seewald K. Severe mental illness in 33,588 prisoners worldwide: systematic review and meta-regression analysis. Br J Psychiatry. 2012;200:364–373. 5. Fazel S, Grann M, Kling B, Hawton K. Prison suicide in 12 countries: an ecological study of 861 suicides during 2003-2007. Soc Psychiatry Psychiatr Epidemiol. 2011;46:191–195. 6. Kouyoumdjian F, Schulder A, Matheson FI, et al. Health status of prisoners in Canada: narrative review. Can Fam Physician. 2016;62:215–222. 7. Metzner J, Trestman R, Appelbaum K, Lewis CF: Gender-specific treatment. In: Metzner J, Trestman R, Appelbaum K, eds. Oxford Textbook of Correctional Psychiatry. Oxford, UK: Oxford University Press; 2015:294–298. 8. Raphael S, Stoll MA. Assessing the contribution of the deinstitutionalization of the mentally ill to growth in the US incarceration rate. J Legal Stud. 2013;42:187–222. 9. Nichols R “The colonialism of incarceration.” Legal Violence and the Limits of the Law. Oxfordshire, England: Routledge, 2017,49–67. 10. Torrey EF, Zdanowicz MT, Kennard AD, et al. The Treatment of Persons with Mental Illness in Prisons and Jails: A State Survey. Virginia, USA. Treatment Advocacy Center. 1. 11. DeHart D, Iachini A. Mental health and trauma among incarcerated persons: development of a training curriculum for Correctional Officers. Am J Crime Justice. 2019;44:457–473. 12. Appelbaum KL, Hickey JM, Packer I. The role of correctional officers in multidisciplinary mental health care in prisons. Psychiatr Serv. 2001;52:1343–1347. 13. Davidson ML. A criminal justice system–wide response to mental illness: evaluating the effectiveness of the Memphis Crisis Intervention Team training curriculum among law enforcement and Correctional Officers. Crime Justice Policy Rev. 2016;27:46–75. 15. Steiner B, Butler HD, Ellison JM. Causes and correlates of prison inmate misconduct: a systematic review of the evidence. J Crime Justice. 2014;42:462–470. 16. Kitto S “What is an Educational Problem?” Revisited. J Contin Educ Health Prof. 2019;39:223–224. 17. Jen Der Pan P, Chang SH, Jiang KJR. Effects of a competency-based counseling training program for correctional officers. Int J Offender Ther Comp Criminol. 2008;52:722–735. 18. Danilovich N, Kitto S, Price DW, Campbell C, Hodgson A, Hendry P. Implementing competency-based medical education in family medicine: a narrative review of current trends in assessment. Fam Med. 2021;53(). 19. Tricco AC, Lillie E, Zarin W, et al. PRISMA extension for scoping reviews (PRISMA-ScR): checklist and explanation. Ann Intern Med. 2018;169:467–473. 21. Kitto S, Chesters J, Grbich C. Quality in qualitative research. Criteria for authors and assessors in the submission and assessment of qualitative research articles for the Medical Journal of Australia. Med J Aust. 2008;188:243–246. 22. Hsieh HF, Shannon SE. Three approaches to qualitative content analysis. Qual Health Res. 2005;15:1277–1288. 23. Moore DE, Green JS, Gallis HA. Achieving desired results and improved outcomes: integrating planning and assessment throughout learning activities. J Contin Educ Health Prof. 2009;29:1–15. 24. Parker GF. Impact of a mental health training course for correctional officers on a special housing unit. Psychiatr Serv. 2009; 60:640–645. 25. Maltman L, Hamilton L. Preliminary evaluation of personality disorder awareness workshops for prison staff. J Forensic Psychol Pract. 2011;13:244–256. 26. Melnikov S, Elyan-Antar T, Schor R, et al. Nurses teaching prison officers: a workshop to reduce the stigmatization of prison inmates with mental illness. Perspect Psychiatr Care. 2017; 53:251–258. 27. Doran N, Hohman M, Koutsenok I. Linking basic and advanced motivational interviewing training outcomes for juvenile correctional staff in California. J Psychoact Drugs. 2011; 43:19–26. 28. Mazmanian PE, Davis DA, Galbraith R. Continuing medical education effect on clinical outcomes. Chest. 2009;135:5S–7S. 29. Hayes AJ, Shaw JJ, Lever-Green G, et al. Improvements to suicide prevention training for prison staff in England and Wales. Suicide Life-threatening Behav. 2008;38:708–713. 30. Sovronsky HR, Shapiro I. The New York State model suicide prevention training program for local corrections officers. Psychiatr Q. 1989;60:139–149. 31. Cutler J, Bailey J, Dexter P. Suicide awareness training for prison staff: an evaluation. Legal Criminol Psychol. 1997; 28:65–69. 32. Ware S, Ruzsa J, Dias G It can't Be fixed because it's not broken: racism and disability in the prison industrial complex. Ben-Moshe L, Chapman C, Carey AC, (eds). Disability Incarcerated. Palgrave Macmillan, AMA Books, New York. 2014. 163–184. 33. Robertson MK, Umble KE, Cervero RM Impact studies in continuing health professions: Update J Contin Educ Health Prof. 2003;23:146–156. 34. Mansouri M, Lockyer J. A meta-analysis of continuing medical education effectiveness. J Contin Educ Health Prof. 2007;27:6–15. 35. Moore DE. Needs assessment in the new health care environment: combining discrepancy analysis and outcomes to create more effective CME. J Contin Educ Health Prof. 1998;18:133–141. 36. Davis DA, Thomson MA, Oxman AD, Haynes RB. Changing physician performance: a systematic review of continuing medical education strategies. JAMA. 1995;274: 700–705.
留言 (0)