This retrospective study included patients managed in the 23-bed adult intensive care unit of the Marie Lannelongue Cardiothoracic Surgery Hospital (Groupe Hospitalier Paris Saint Joseph, Le Plessis-Robinson, France). A national review board CERAR approved the study (IRB0001025). All patients received an information and no-objection statements in accordance with the French law on retrospective studies.
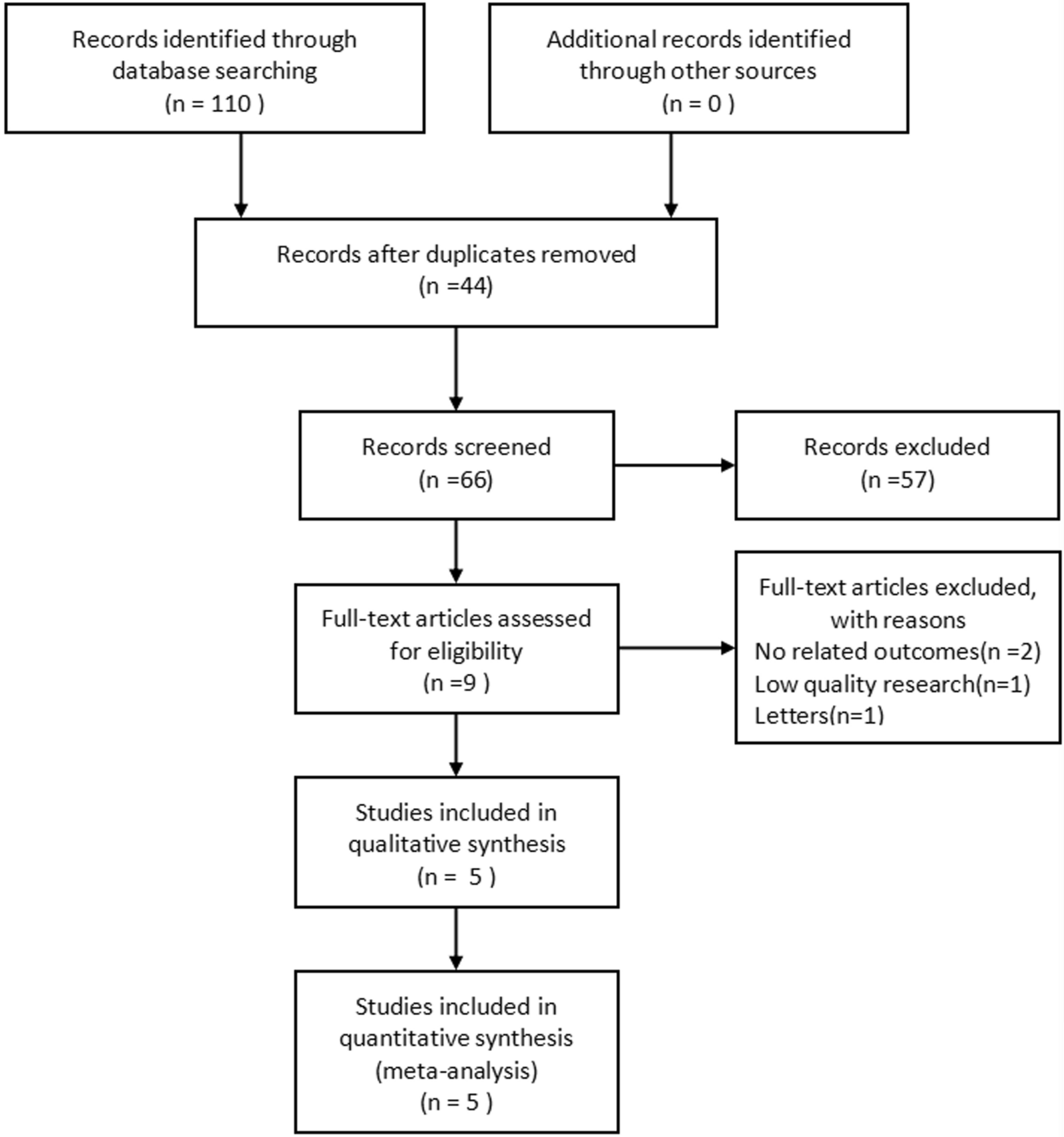
Records of consecutive adults managed with ECMO between January 2017 and August 2020 were screened to identify patients who required circuit changes due to bleeding or thrombosis with oxygenation failure. Each circuit change was handled as a separate event.
Definitions
Bleeding group was defined as either bleeding persistent for more than two days or bleeding uncontrolled despite hemostatic procedures (arterio-embolization, surgical revision, packing, local hemostatic procedure during endoscopy). Bleeding localization was epistaxis or oral bleeding, cannula- or catheter-related bleeding, hemoptysis, and deep bleeding.
Thrombosis group included sudden thrombosis of head pump or circuit, clots on the membrane visible to the naked eye combined with hypoxemia defined as desaturation < 90% or right radial PaO2 < 80 mmHg with ECMO FiO2 ≥ 80%. When oxygenator did not allow direct visualization of clots on the membrane, thrombosis was defined as membrane dysfunction with a post-oxygenator blood gas sample showing an ECMO PaO2/FiO2 < 200 mmHg [5].
ECMO monitoring
For VV- and VA-ECMO, unfractionated heparin (UFH) was administered to maintain antiXa between 0.2 and 0.4 IU/mL, with dosage adjustments after each antiXa assay performed at least every 12 h. In compliance with ELSO recommendations, in patients with bleeding, UFH was interrupted for up to 12 h or as long as needed to control the bleeding [3]. Once the bleeding was controlled, effective anticoagulation was reintroduced in patients with formal indications (e.g., pulmonary embolism, loss of arterial pulsatility, mechanical valve).
Laboratory tests performed at least twice daily included hemoglobin, platelet count, antiXa, fibrinogen, pH, PaCO2, and PaO2.
Protocolized transfusions of red blood cells (RBC), platelets, fresh frozen plasma (FFP), and fibrinogen were given to maintain hemoglobin > 7 g/dL, platelets > 30 000/mm3, fibrinogen > 1.5 g/dL, and prothrombin time > 50% [6].
Data collection
For this study, we collected data over the seven days before and after the circuit change (from D-7 to D + 7). D-1 and D + 1 corresponded to the 24 h before and after the change. The data included the blood tests listed above, transfusion data (administered amounts of RBC units, FFP units, platelets, and fibrinogen), and technical data (ECMO and ventilator FiO2, ECMO flow rate). Clinical bleeding and hemostatic procedures were collected over the five days before and after the change (from D-5 to D + 5); this shorter collection period limited the risk of missing data.
Statistical analysis
Data were analyzed using StatView 5.0 software (SAS Institute, Cary, NC). Data distribution was assessed by the Kolmogorov–Smirnov test. Normal data were described as mean ± SD and non-normal data as median [interquartile range]. Continuous variables were compared using Student's t test; for repeated measures, we performed ANOVA followed by the Scheffe test. P values < 0.05 were considered significant.







留言 (0)