

記住我
Neurosurgery is one of the most complex and highly demanding surgical disciplines. Intensive and long training is required to acquire a solid theoretical background, deep anatomical knowledge, hand–eye coordination, manual dexterity, and complex technical skills, in addition to controlling physiologic and psychological tremors. Young neurosurgeons must be aware of the intricate three-dimensional neuroanatomy (3D), the psychomotor abilities, the fatigue related to long operative surgeries, and accurate and safe manipulation in deep and narrow operative corridors, which can affect the surgical performance and results (1–3). For all these reasons, neurosurgical laboratories with human cadaveric specimens result in a unique and irreplaceable training tool for developing and refining anatomical knowledge, dexterity, technical skills, and surgical procedures before performing them on a living patient (4–6). The use of a real human specimen gives the possibility to reproduce the actual procedure, starting from the head positioning to the step-by-step surgery facing narrow corridors, fragile neurovascular structures, and a delicate brain surface, which can give an idea of how gentle and accurate the dissection has to be during the live surgery (4, 6, 7). Nevertheless, permanent neurosurgical laboratories are not widespread all over the world due to strict requirements and permissions, ethical and legal issues, and the high costs related to equipment, materials, and specimens. On the other hand, in the last few decades, medicolegal issues in the medical field and, in particular, neurosurgical practice have increased (8, 9). For these reasons, neurosurgical training has become crucial, with increasing interest in it, to train the next generation of neurosurgeons before practicing on living patients to reduce perioperative complications (10, 11). In this scenario, in recent years, the European Union has increased its financial support to settle up new anatomical and surgical laboratories, and, in parallel, the Italian government has unlocked some restrictions on body donation (12, 13). Convinced of the irreplaceable value of a cadaver lab, in this article we describe our experience in setting up a new microsurgical neuroanatomy lab (IRCCS Neuromed, Pozzilli, Italy), focusing on the development of training activity programs and microsurgical milestones useful to train the next generation of surgeons.
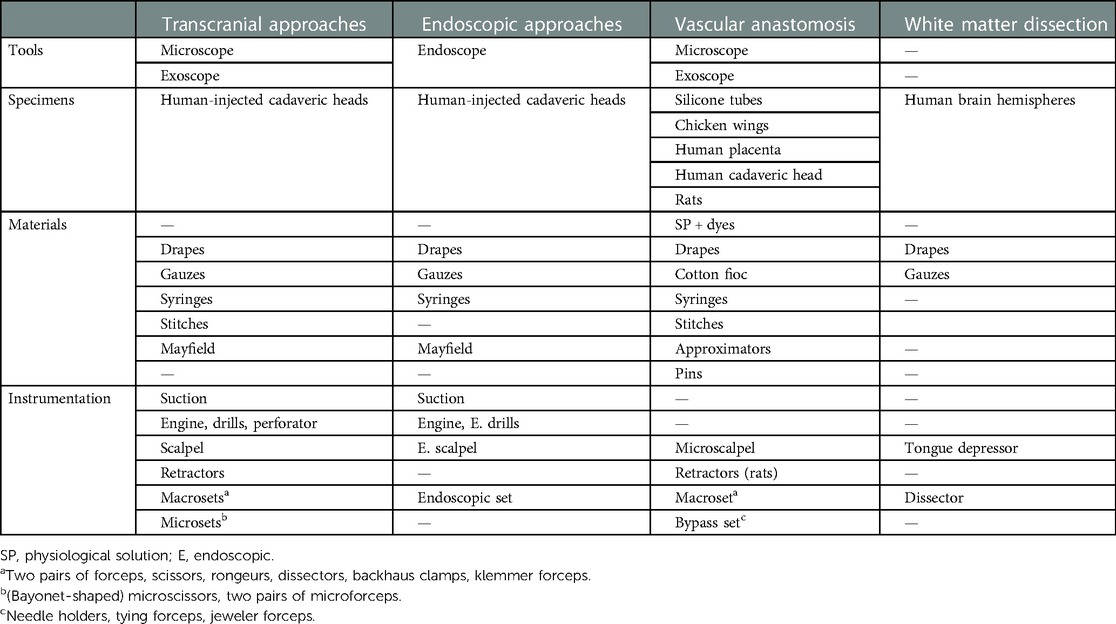
Materials and methodsWe set up a microsurgical neuroanatomy laboratory, “Laboratorio di neuroanatomia G. Cantore” (Centro di Medicina Necroscopica-Unità di Chirurgia Formativa), at Parco Tecnologico IRCCS Neuromed in Pozzilli (Italy), according to the Italian requirements (Law no. 10, 10 February 2020; G.U., 4 March 2020). The laboratory and all its activities on human and animal specimens were approved by the ethical committee of IRCCS Neuromed. Embalmed and latex-injected human cadaveric heads have been used for dissections, while the human placenta has been furnished by the Obstetrics and Gynecology Department of the Istituto Clinico Mediterraneo (ICM, Salerno, Italy) as a scientific donation after birth, and Sprague–Dawley rats were provided by the Neuromed stabularium according to the Italian law on laboratory animal welfare (D.lgs. 26/2014). The human placenta was prepared as reported elsewhere (14). A dedicated veterinarian took care of the rodents, proceeding with anesthesia, analgesia, and immobilization during the courses. All the required materials and instruments are listed in Table 1. Moreover, a permanent neuronavigation system (Treon, Medtronic) is present in the lab for measurements and anatomical verification during research activities.
Table 1. Required materials and instruments.
The training program for neurosurgical residents has been developed considering the progressive competency acquired in each year of residency, from basic techniques and procedures to complex anatomy and approaches. Four types of dissection courses have already been organized at our laboratory for neurosurgical residents and young neurosurgeons: (a) basic techniques and approaches using the microscope; (b) the 3D exoscope; (c) transcranial and endoscopic skull base approaches; and (d) microvascular anastomosis on the human placenta and rats. Furthermore, an ongoing anatomical research activity is currently being performed.
A review of the literature on anatomy and dissection guides has been done to provide a list of “suggested references” for the preparation of trainees.
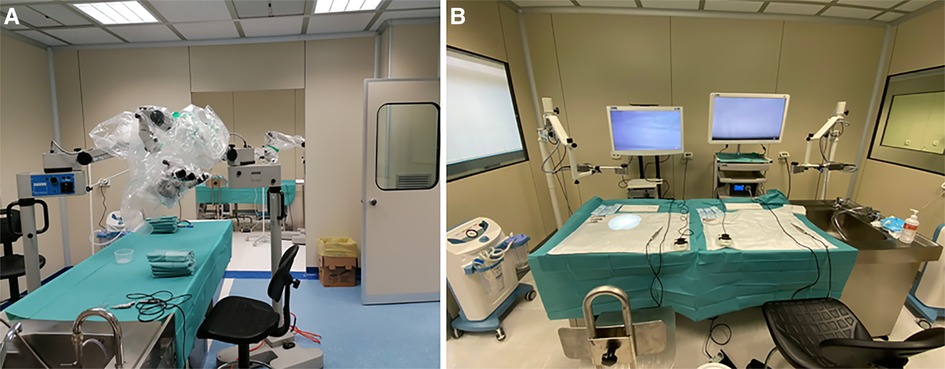
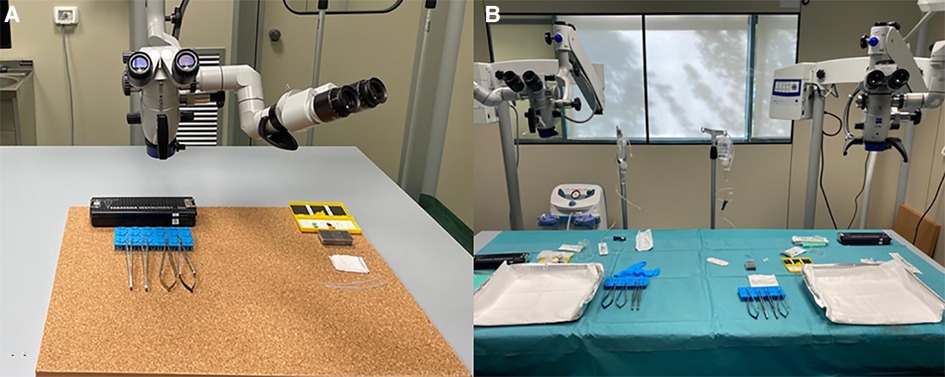
ResultsSix competency levels were designed according to the year of residency (PGY, from 1 to 5): (1) soft tissue dissections, bone drilling, and microsurgical suturing; (2) basic craniotomies and neurovascular anatomy; (3) white matter dissection; (4) skull base transcranial approaches; (5) endoscopic approaches; (6) vessel preparation on placenta and rats; and (7) microanastomosis. For each level, a checklist with milestones is provided in Table 2. Figure 1 shows the organization of our lab.
Figure 1. Workstations at “Laboratorio di neuroanatomia G. Cantore.”
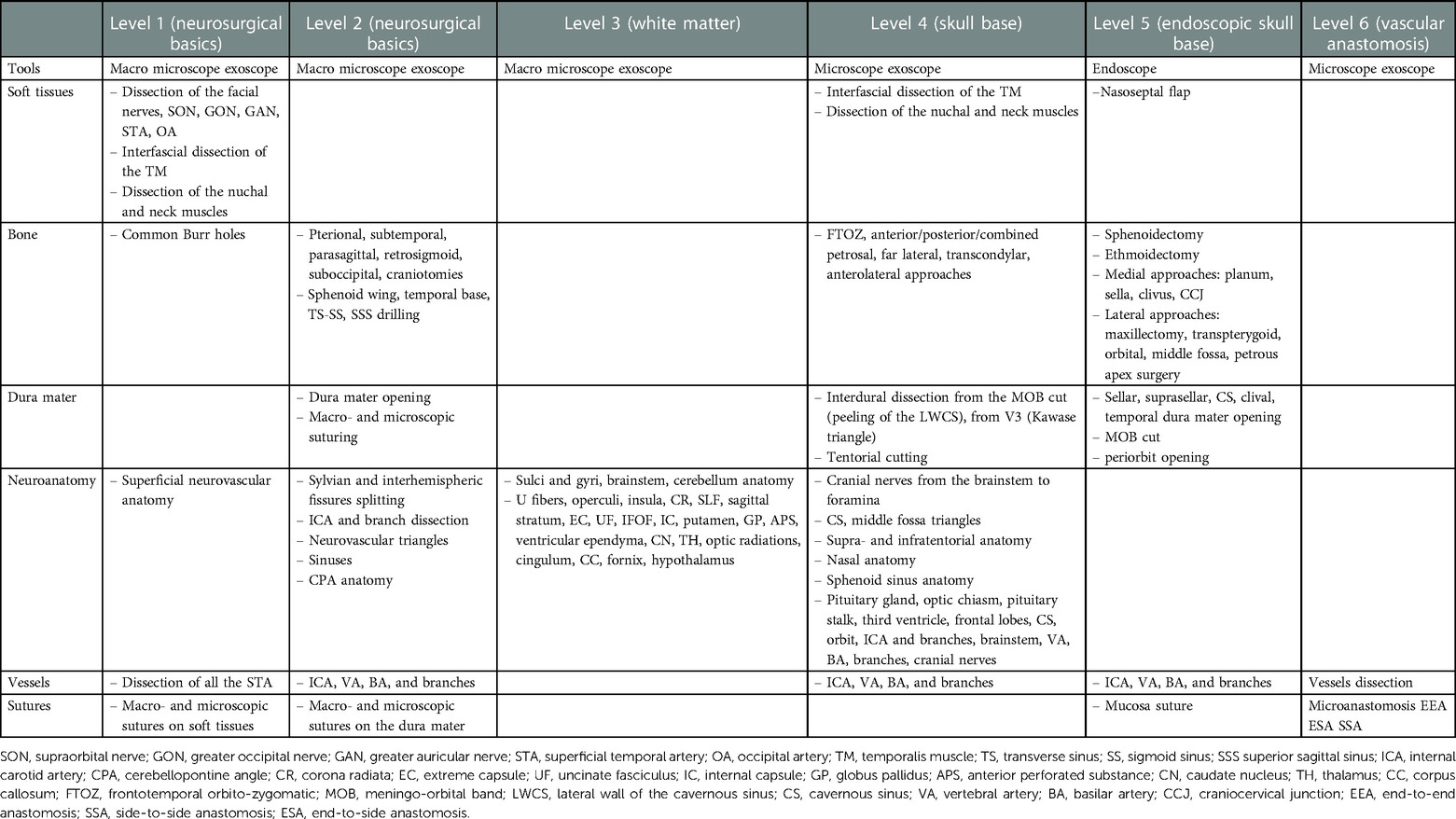
Table 2. Proposed milestone checklist for training.
Level 1: soft tissue dissections, bone drilling, and microsurgical suturing (PGY 1–2)Level 1 represents the surgical basics for PGY1. The junior resident should know the different myocutaneous layers, their relationship with nerves and vessels, craniometric points, and differences between cortical and cancellous bones. At this level, the resident must become familiar with the Mayfield head holder, macroscopic instruments, dissection techniques, engine functioning, bone drilling, and macro and microscopic suture techniques.
Level 2: basic craniotomies and neurovascular anatomy (PGY 2–3)Level 2 corresponds to PGY2 and PGY3. The resident should be able to perform basic craniotomies, that is, pterional, subtemporal, parasagittal, retrosigmoid, and suboccipital approaches. They must perform Sylvian and interhemispheric fissure openings and know the target anatomy exposed during each approach. The resident must become familiar with bony drilling without injuring neurovascular structures.
Level 3: white matter dissection (PGY 3–4)Level 3 represents the anatomical knowledge of white matter for PGY3 and PGY4. Knowledge of the anatomy of the cerebral surface, white matter fibers, deep nuclei, brainstem, and cerebellum is mandatory. At this level, the resident becomes confident enough in white matter dissection to dissect the main structures.
Level 4: skull base transcranial approaches (PGY 4–5)Level 4 represents the advanced transcranial craniotomies for skull-base pathologies. This level is addressed to PGY4 and PGY5. The resident should be able to perform those approaches and recognize the extra- and intradural anatomies. Gentle interdural dissection, bony drilling in deep and narrow fields, and cutting the tent without injuring neurovascular structures are important technical skills.
Level 5: endoscopic transnasal approaches (PGY 4–5)Level 5 is addressed to PGY4 and PGY5 and corresponds to endoscopic transnasal approaches. The resident should learn the anatomy of the nasal cavity and its relationship with the maxillary, orbital, ethmoidal, sphenoidal, clival, and craniocervical junction (CCJ) compartments. Preparation of the nasoseptal flap and the transsphenoidal approach to the sella is the first step, followed by extended medial and lateral approaches. The resident must become familiar with the endoscope and one-hand dissection. Finally, an endoscopic mucosal suture should be attempted.
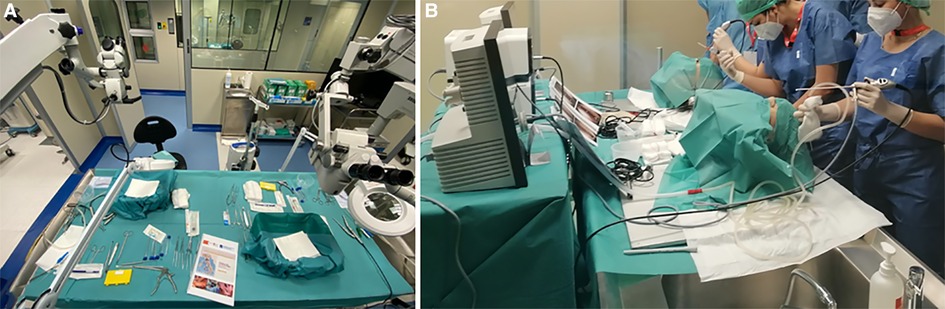
Figure 2 shows the arrangement of the stations during our microsurgical and endoscopic courses.
Figure 2. Arrangement of the stations during our (A) microsurgical and (B) endoscopic courses.
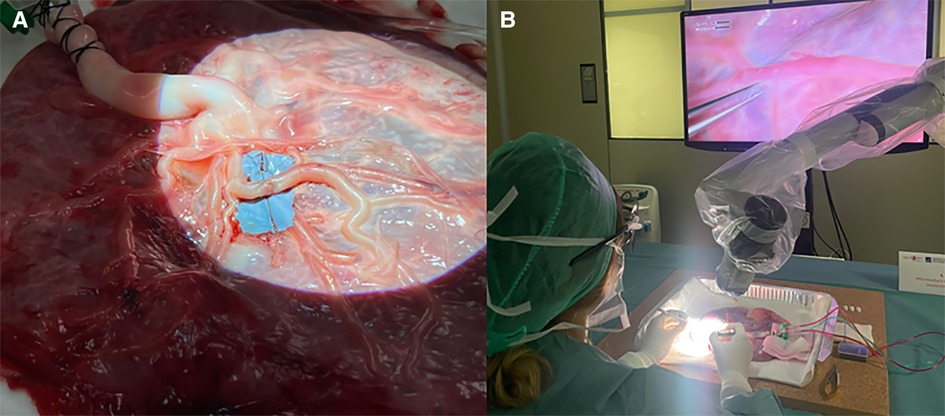
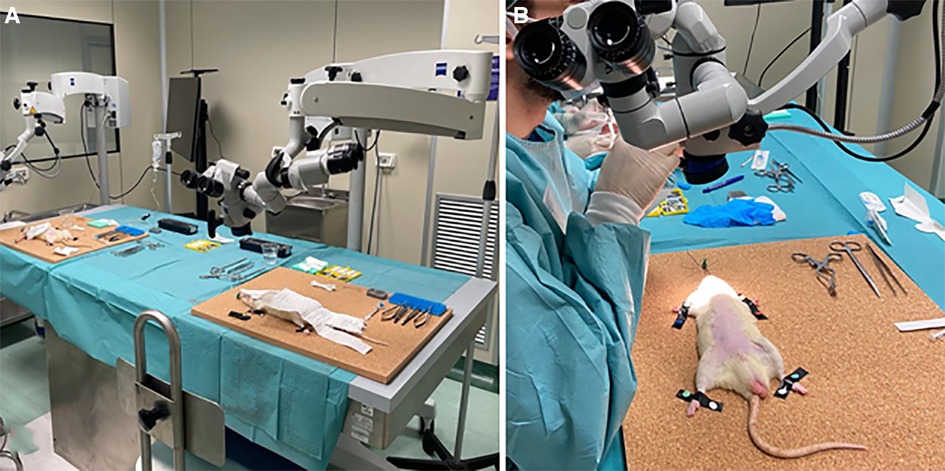
Level 6: vessel preparation and microanastomosis on inert materials, chicken wings, human placenta, human cadavers, and rats (PGY 5)Level 6 is addressed to PGY 5 and represents one of the most difficult skills to acquire in neurosurgery, namely vascular anastomosis. Starting from inert materials such as gauze and silicon tubes, the resident should train in simple knots and end-to-end, end-to-side, and side-to-side microanastomoses. Figure 3 shows the organization of the stations. Chicken wings and human placenta are used to mimic the consistency of the vessels and to train with vessel dissection. As described elsewhere (14), the human placenta is prepared and injected continuously with red and blue saline solution by cannulating the umbilical arteries and veins (Figure 4). The following step is using human cadaveric heads and in vivo rats. In particular, the human specimen allows for the replication of a real surgical procedure for bypass, dissecting vessels, and performing microanastomoses in deep fields. On the other side, the in vivo rat is the most realistic model through which it is possible to simulate bloody dissection, blood pulsation, empathy, and anxiety (Figure 5).
Figure 3. Workstation for microanastomosis on (A) inert materials and (B) wet specimens.
Figure 4. (A) Preparation of human placenta for microanastomosis with cannulation of the umbilical arteries and vein. After washing arteries and veins with clean water to remove blood clots, colored saline solution is used to continuously fill the vessels mimicking the blood. (B) Vascular dissection and microanastomosis on human placenta using a 3D exoscope.
Figure 5. (A,B) Workstation to perform dissection and microanastomosis on in vivo rats.
Finally, in Table 3, we reported a list of some useful books and articles’ references for each level of competency to guide the residents during their studies and cadaveric dissections.
Table 3. Suggested references for dissections.
DiscussionThe education and training needed to become a neurosurgeon consist of a long and demanding program that consists of acquiring a solid theoretical background and clinical and surgical experience. Residents in neurosurgery have to spend a lot of time in the operating room to become familiar with surgical anatomy and techniques and to develop practical skills (1–3). Although intraoperative surgical exposure represents the fundamental way to train surgeons, several drawbacks are encountered in every country. Differences between departments, hospitals, and nations are wide, and residents often do not have the same opportunity in their education and operation room in particular (101–107). Considering the European centers, recent surveys among neurosurgical residents report very low satisfaction rates for the theoretical and practical aspects of training in some countries (101). Moreover, novel regulations on reducing working hours for residents reduce the possibilities for practical and psychophysical training, affecting the quality of the residency and prolonging the learning curve (108, 109). These controversial aspects are also critical for the increasing medicolegal issues affecting medical practice in the last few decades (8, 9). Accordingly, the impossibility to try or repeat surgical procedures makes neurosurgical training more difficult. For all these reasons, training on human cadaveric specimens results in an essential and irreplaceable tool for residents and fully-trained neurosurgeons (10). Similarly, the evolution of simulation technology applied to surgery has assumed an important role in learning anatomy, completing procedural tasks, and improving accuracy and hand–eye coordination. In recent years, 3D inert models and virtual and augmented reality have been popularized among universities and through courses to train young residents (110, 111). Nevertheless, the use of a real human specimen gives the possibility to reproduce the real procedure starting from the head positioning to the step-by-step surgery facing narrow corridors, fragile neurovascular structures, and a delicate brain surface that can give an idea of how gentle and accurate the dissection has to be during the live surgery. Last but not least, training on human cadavers differs from inert materials or simulation tools because the trainer must also manage the emotional counterpart, empathy, and respect for the human body that can approximate real surgery.
Laboratory setupAfter the introduction in Italy of Law no. 10 of 10 February 2020 entitled “Rules regarding the disposition of one's body and postmortem tissues for study, training, and scientific research purposes,” our Neurosurgical Department and IRCCS Neuromed have worked together to set up a new microsurgical neuroanatomy laboratory called “Laboratorio di neuroanatomia G. Cantore” (Centro di Medicina Necroscopica—Unità di Chirurgia Formativa) at Parco Tecnologico Neuromed in Pozzilli (Italy). Finally, our laboratory has been accredited as a no-profit laboratory for body donation with other centers in Italy. This lab has been created based on our previous experiences with neurosurgical dissections in several laboratories around the world to offer educational opportunities and training activities for residents and neurosurgeons from Italy and abroad and establish research fellowships and permanent surgical research. After the initial funding for no-profit research, a policy of reuse has been applied in our no-profit lab. The necessary equipment has been found through the recovery of disused microscopes and instruments, a donation from retired surgeons, and second-hand instruments left in the lab after courses. Expired or nonsterile materials are also routinely brought into the operative room (OR) of our hospital.
For research fellows (two for each semester) and residents, a “neurosurgical booklet,” represented in Table 2 as a checklist, is furnished to give a progressive training guide. The concept is to take all the time to perform slow and gentle step-by-step dissection to preserve tissues and understand the 3D surgical anatomy and intricate relationships between structures. Meticulous work and a sound state of mind are essential to preparing the fellow for the accuracy necessary to be a neurosurgeon. Moreover, it is essential to acquire strong neuroanatomical knowledge through transcranial and endoscopic dissections to understand the anatomy from different perspectives directly on the specimen, which is the basis for performing their research.
In parallel, fellows can observe surgical procedures to treat skull base pathologies, gliomas, or epilepsy in our department, taking inspiration to learn more about a procedure directly on the specimen or to develop new anatomical research or approaches.
CoursesDuring the first year of activity, we organize six courses for neurosurgical residents and young neurosurgeons, ranging from basic to more complex: (a) basic techniques and approaches using the microscope and (b) the exoscope, (c) transcranial and endoscopic skull base approaches, and (d) microvascular anastomosis on the human placenta and rats. The costs for human specimens and organization are supported by sponsors and participation fees. Each specimen preserved in a solution of alcohol, water, and softener can be reused for different courses, lowering the final cost. Considering the aforementioned checklist (Table 2), we have organized these courses taking into account the year of residency and related neurosurgical milestones. Each course included theoretical lectures and practical lab sessions.
Basic techniques and approachesThe goal of these courses is to introduce the young resident to the basics of neurosurgery. Milestones of these courses include soft tissue dissection preserving the facial nerve and superficial temporal artery (STA), drilling techniques, basic craniotomies, sinus exposure, dura opening, interhemispheric and Sylvian fissure dissections, relevant intradural anatomy, and dura closure with a patch. During these courses, residents become familiar with instruments and techniques, can perform more common approaches such as pterional, parasagittal, and retrosigmoid approaches, and study surgical anatomy. Given the technological advancements in the neurosurgical field and the recent introduction of 3D exoscopes in surgical practice (112), we organize courses that not only use microscopes, but also hybrid microexoscopes and only exoscopes. The use of a 3D exoscope during a cadaveric course has gained widespread approval from trainees due to the limited presence of this technology in Italian hospitals.
Transcranial and endoscopic skull base approachesThese courses are addressed to senior residents and neurosurgeons and consist of lectures and practice on skull base anatomy, pathologies, surgical strategies, and both transcranial and endoscopic approaches. Great emphasis is given to extradural anatomy and corridors. Participants exercise accurate drilling techniques and gentle intradural dissection in narrow and deep corridors. A combination of transcranial and endoscopic approaches can provide a 360° view of anatomy.
Microvascular anastomosis on inert materials, placenta, and ratsThe course is aimed at senior residents and neurosurgeons who want to learn the techniques of microsuturing and train their skills. Sutures, dedicated instruments, and step-by-step techniques are illustrated during lectures. In the lab, each participant has their own station with microscopes, instruments, and sutures (from 6.0 to 10.0). Starting from inert materials, like gauze and synthetic vessels, the participant can practice different anastomotic techniques on fresh human placenta, which simulates the vessels, arachnoid, and pia mater. The placenta is cannulated and perfused first with water and then with a colored saline solution (red for arteries and blue for veins). After practicing on ex vivo specimens and trying to perform a patent and functional anastomosis, the participant could perform it on in vivo rats under sedation. It is the most realistic model through which it is possible to simulate bloody dissection, blood pulsation, empathy, and anxiety with the aim of not killing the specimen.
Depending on specific areas of training, these presented milestones could be fine-tuned and expanded by training experts.
Universities and international networksConsidering the aforementioned drawbacks, limitations, and differences among the neurosurgical training centers, in particular, in Europe and especially in our country (101, 109), that affect the learning curve of young neurosurgeons and ultimately the quality of medical assistance, the authors believe that it is time to renovate the residency systems. As previously proposed by Stienen et al., European standard guidelines for neurosurgical training could help further harmonize training among European countries and facilitate exchange (101). As regards the last decade, great work has been done by the European and Italian Neurosurgical Societies (EANS, SINCH) to contribute to the improvement of neurosurgical education through EANS training courses, the EANS spine diploma, SINCH basic courses for young residents, and hands-on courses. Nevertheless, all these opportunities remain at the discretion of the single resident and professor, are limited in time, and are affected by economical and organizational issues. The authors believe that the same compulsory theoretical program has to be suggested for all European countries during all the years of residency, in addition to being a parallel compulsory operative training plan that sustains and reinforces the surgical training in the OR with a uniform and verified number of procedures performed by the resident. Acquiring 3D anatomical knowledge, technical skills, manual dexterity, visuospatial ability, and surgical procedures should not be a choice for a neurosurgical resident, but rather a mandatory requirement to become a neurosurgeon. For this reason, the authors believe that each resident of all residency programs must have the opportunity to spend a period during each year of their residency in a cadaveric laboratory with a precise step-by-step “neurosurgical training checklist” with progressive milestones to improve the quality of operative training and guarantee equal skill acquisition all over the world.
However, high costs, difficult human specimen acquisition, and bureaucracy issues make this goal impossible. As reported by Italian anatomists (13), although Italian law is now more permissive about body donation, the number of centers performing anatomical dissections for the benefit of medical students and residents has decreased in favor of the few universities that can afford it.
LimitationsAlthough human cadaveric specimens and fixed brain hemispheres are the most reliable models for reproducing anatomy and surgery on a living patient, technical limitations are not negligible. If embalmed specimens can be easily conserved, their soft tissue and brain stiffen, affecting the qualitative and quantitative study of the approach. On the contrary, fresh specimens overcome this issue, resulting in a greater similarity to the living one at the cost of limited conservation and use, increasing the costs. Second, the absence of the cerebrospinal fluid or the pathology of interest, such as tumors and vascular malformations, makes the cadaver defective and far from a real model.
Furthermore, the resident who spends some time in the laboratory should not forget that their experience in the OR is essential and irreplaceable for the emotional counterpart and the anxiety for responsibility related to the patient’s expectations.
Future directionsAs neurosurgeons are involved in intense cadaveric activities, we believe that more efforts should be made to create collaboration between universities and laboratories to optimize human, material and financial resources with the aim of establishing a solid and equitable operative training program. For this purpose, the provided “neurosurgery booklet” could be a starting point to be spread among universities and hands-on courses. The usefulness of this milestone approach should be discussed in the neurosurgical community and validated through questionnaires given to faculty experts and trainees. In this regard, we are formulating dedicated surveys for each level of competency to administer to participants of our cadaveric courses and research fellows in our lab. Similarly, training protocols on cadaveric specimens could be developed for spinal and peripheral neurosurgery. Although the higher costs of specimens and instrumentation could limit the possibilities, permanent laboratories for spinal and peripheral nerve surgery should be developed.
On another aspect, despite the great knowledge of neuroanatomy and surgical advances in the last few decades, descriptive neurosurgical anatomy is continually evolving through multidisciplinary description, new surgical corridors, and the improvement of minimally invasive skull base approaches (15). In this scenario, cadaver laboratories play a fundamental role in enhancing neuroanatomical knowledge and surgical outcomes. Different skull base research projects could be performed in the lab: description of anatomy with the integration of radiological examinations, development of three-dimensional models for surgical and training purposes, description of minimally invasive corridors, and comparison between surgical approaches. For this reason, a permanently equipped laboratory with research fellows is imperative.
ConclusionMicrosurgical dissection of human cadaveric specimens is the optimal way to learn and train on neuroanatomy and neurosurgical procedures before safely performing them in the operating room. The authors believe that the neurosurgical preparation has to be integrated with a compulsory operative training program as a complementary activity during all the years of residency. The goals are acquiring three-dimensional anatomical knowledge, technical skills, manual dexterity, visuospatial ability, and surgical procedures. We provided a “neurosurgery training checklist” with progressive milestones for neurosurgical residents. This step-by-step operational program may improve the quality of training and guarantee equal skill acquisition across countries. We believe that more efforts should be made to create new microsurgical laboratories, popularize the importance of body donation, and encourage collaboration between universities and laboratories.
Data availability statementThe original contributions presented in the study are included in the article/Supplementary Material; further inquiries can be directed to the corresponding author.
Ethics statementThe animal study was reviewed and approved by the Ethics Committee of IRCCS Neuromed.
Author contributionsConception and design: AF, PdR, and VE. Data: AF, PdR, NG, MDA, and VE. Drafting: AF. Critical revision of the article: PdR, NG, MDA, and VE. All authors contributed to the article and approved the submitted version.
FundingThis study was supported by the Ministero della Salute (Ricerca Corrente 2023).
Conflict of interestThe authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's noteAll claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References1. Yaşargil MG. A legacy of microneurosurgery: memoirs, lessons, and axioms. Neurosurgery. (1999) 45(5):1025–92. doi: 10.1097/00006123-199911000-00014
CrossRef Full Text | Google Scholar
3. Belykh E, Onaka NR, Abramov IT, Yağmurlu K, Byvaltsev VA, Spetzler RF, et al. Systematic review of factors influencing surgical performance: practical recommendations for microsurgical procedures in neurosurgery. World Neurosurg. (2018) 112:e182–207. doi: 10.1016/j.wneu.2018.01.005
PubMed Abstract | CrossRef Full Text | Google Scholar
4. Aboud E, Al-Mefty O, Yaşargil MG. New laboratory model for neurosurgical training that simulates live surgery. J Neurosurg. (2002) 97(6):1367–72. doi: 10.3171/jns.2002.97.6.1367
PubMed Abstract | CrossRef Full Text | Google Scholar
5. Moon K, Filis AK, Cohen AR. The birth and evolution of neuroscience through cadaveric dissection. Neurosurgery. (2010) 67(3):710–99. doi: 10.1227/01.NEU.0000383135.92953.A3
CrossRef Full Text | Google Scholar
6. Matsushima T, Matsushima K, Kobayashi S, Lister JR, Morcos JJ. The microneurosurgical anatomy legacy of Albert L. Rhoton Jr. MD: an analysis of transition and evolution over 50 years. J Neurosurg. (2018) 129(5):1331–41. doi: 10.3171/2017.7.JNS17517
PubMed Abstract | CrossRef Full Text | Google Scholar
7. Hernesniemi J, Niemelä M, Karatas A, Kivipelto L, Ishii K, Rinne J, et al. Some collected principles of microneurosurgery: simple and fast, while preserving normal anatomy: a review. Surg Neurol. (2005) 64(3):195–200. doi: 10.1016/j.surneu.2005.04.031
PubMed Abstract | CrossRef Full Text | Google Scholar
8. Steele L, Mukherjee S, Stratton-Powell A, Anderson I, Timothy J. Extent of medicolegal burden in neurosurgery: an analysis of the national health service litigation authority database. Br J Neurosurg. (2015) 29(5):622–9. doi: 10.3109/02688697.2015.1054362
PubMed Abstract | CrossRef Full Text | Google Scholar
9. Lefever D, Esfahani DR, Kandregula S, Trosclair K, Demand A, Vega A, et al. The medical legal environment in neurosurgery: an informative overview of the stages of litigation and distinct challenges. World Neurosurg. (2021) 151:370–4. doi: 10.1016/j.wneu.2021.03.039
PubMed Abstract | CrossRef Full Text | Google Scholar
10. Bernardo A. Establishment of next-generation neurosurgery research and training laboratory with integrated human performance monitoring. World Neurosurg. (2017) 106:991–1000. doi: 10.1016/j.wneu.2017.06.160
PubMed Abstract | CrossRef Full Text | Google Scholar
11. Hoz SS, Al-Sharshahi ZF, Esene IN, Al-Awadi OM, Salih HR, Alrawi MA, et al. More laboratory simulations—fewer brain complications: prospects from the first neurosurgery laboratory in Iraq. World Neurosurg. (2022) 157:30–4. doi: 10.1016/j.wneu.2021.09.087
PubMed Abstract | CrossRef Full Text | Google Scholar
12. McHanwel S, Brenner E, Chirculescu ARM, Drukker J, van Mameren H, Mazzotti G, et al. The legal and ethical framework governing body donation in Europe: a review of current practice and recommendations for good practice. Eur J Anat. (2008) 12(1):1–24.
13. De Caro R, Boscolo-Berto R, Artico M, Bertelli E, Cannas M, Cappello F, et al. The Italian law on body donation: a position paper of the Italian college of anatomists. Ann Anat. (2021) 238:151761. doi: 10.1016/j.aanat.2021.151761
PubMed Abstract | CrossRef Full Text | Google Scholar
14. Del Maestro M, Rampini AD, Mauramati S, Giotta Lucifero A, Bertino G, Occhini A, et al. Dye-perfused human placenta for vascular microneurosurgery training: preparation protocol and validation testing. World Neurosurg. (2021) 146:e854–64. doi: 10.1016/j.wneu.2020.11.034
PubMed Abstract | CrossRef Full Text | Google Scholar
17. Rhoton AL Jr. The orbit. Neurosurgery. (2002) 51(4 Suppl):303–34. PMID: 12234452. doi: 10.1227/01.NEU.0000028329.38986.47
CrossRef Full Text | Google Scholar
18. Rhoton AL. Jugular foramen: The posterior cranial fossa: Microsurgical anatomy and surgical approaches. Neurosurgery. (2007) 47 (Suppl. 3), S267–85. doi: 10.1227/01.NEU.0000296227.70319.6E
CrossRef Full Text | Google Scholar
20. Rhoton J. The posterior cranial fossa: microsurgical anatomy and surgical approaches. Neurosurgery. (2000) 47(3 Suppl):5–6. doi: 10.1097/00006123-200009001-00005
CrossRef Full Text | Google Scholar
30. Rhoton AL. The cavernous sinus, the cavernous venous plexus, and the carotid collar. Neurosurgery. (2002) 51:375–410. doi: 10.1227/01.NEU.0000028833.01529.E7
CrossRef Full Text | Google Scholar
32. Ammirati M, Bernardo A. Anatomical study of the superior orbital fissure as seen during a pterional approach. J Neurosurg. (2007) 106(1):151–6. doi: 10.3171/jns.2007.106.1.151
PubMed Abstract | CrossRef Full Text | Google Scholar
33. Chaddad-Neto F, Filho JMC, Dória-Netto HL, Faria MH, Ribas GC, Oliveira E. The pterional craniotomy: tips and tricks. Arq Neuropsiquiatr. (2012) 70(9):727–32. doi: 10.1590/S0004-282X2012000900015
PubMed Abstract | CrossRef Full Text | Google Scholar
34. Coscarella E, Vishteh AG, Spetzler RF, Seoane E, Zabramski JM. Subfascial and submuscular methods of temporal muscle dissection and their relationship to the frontal branch of the facial nerve. Technical note. J Neurosurg. (2000) 92(5):877–80. doi: 10.3171/jns.2000.92.5.0877
PubMed Abstract | CrossRef Full Text | Google Scholar
35. Oikawa S, Mizuno M, Muraoka S, Kobayashi S. Retrograde dissection of the temporalis muscle preventing muscle atrophy for pterional craniotomy: technical note. J Neurosurg. (1996) 84(2):297–9. doi: 10.3171/jns.1996.84.2.0297
PubMed Abstract | CrossRef Full Text | Google Scholar
37. Poblete T, Jiang X, Komune N, Matsushima K, Rhoton AL. Preservation of the nerves to the frontalis muscle during pterional craniotomy. J Neurosurg. (2015) 122(6):1274–82. doi: 10.3171/2014.10.JNS142061
PubMed Abstract | CrossRef Full Text | Google Scholar
38. Campero A, Villalonga JF, Elizalde RL, Ajler P. The nuchal lines as anatomic landmarks to dissect the muscles in the far lateral approach. World Neurosurg. (2018) 113:188–94. doi: 10.1016/j.wneu.2018.02.090
PubMed Abstract | CrossRef Full Text | Google Scholar
39. Rhoton J. The far-lateral approach and its transcondylar, supracondylar, and paracondylar extensions. Neurosurgery. (2000) 47(3 Suppl). doi: 10.1097/00006123-200009001-00020
CrossRef Full Text | Google Scholar
40. Ribas GC, Rhoton AL, Cruz OR, Peace D. Suboccipital burr holes and craniectomies. Neurosurg Focus. (2005) 19(2):1–12. doi: 10.3171/foc.2005.19.2.2
CrossRef Full Text | Google Scholar
41. Rhoton AL. The cerebellopontine angle and posterior fossa cranial nerves by the retrosigmoid approach. Neurosurgery. (2000) 47(Suppl 3):S93–129. doi: 10.1097/00006123-200009001-00013
PubMed Abstract | CrossRef Full Text | Google Scholar
42. Ugur HC, Dogan I, Kahilogullari G, Al-Beyati ESM, Ozdemir M, Kayaci S, et al. New practical landmarks to determine sigmoid sinus free zones for suboccipital approaches: an anatomical study. J Craniofac Surg. (2013) 24(5):1815–8. doi: 10.1097/SCS.0b013e3182997ff8
PubMed Abstract | CrossRef Full Text | Google Scholar
43. Savardekar A, Nagata T, Kiatsoontorn K, Terakawa Y, Ishibashi K, Goto T, et al. Preservation of labyrinthine structures while drilling the posterior wall of the internal auditory canal in surgery of vestibular schwannomas via the retrosigmoid suboccipital approach. World Neurosurg. (2014) 82(3):474–9. doi: 10.1016/j.wneu.2014.02.029
PubMed Abstract | CrossRef Full Text | Google Scholar
45. Sampath P, Rini D, Long DM. Microanatomical variations in the cerebellopontine angle associated with vestibular schwannomas (acoustic neuromas): a retrospective study of 1006 consecutive cases. J Neurosurg. (2000) 92(1):70–8. doi: 10.3171/jns.2000.92.1.0070
PubMed Abstract | CrossRef Full Text | Google Scholar
46. Giammattei L, Starnoni D, Benes V, Froelich S, Cossu G, Borsotti F, et al. Extreme lateral supracerebellar infratentorial approach: surgical anatomy and review of the literature. World Neurosurg. (2021) 147:89–104. doi: 10.1016/j.wneu.2020.12.042
PubMed Abstract | CrossRef Full Text | Google Scholar
47. Campero A, Tróccoli G, Martins C, Fernandez-Miranda JC, Yasuda A, Rhoton ALJ. Microsurgical approaches to the medial temporal region: an anatomical study. Neurosurgery. (2006) 59(4 Suppl 2), discussion ONS307-8:ONS279-307, doi: 10.1227/01.NEU.0000223509.21474.2E.17041498
PubMed Abstract | CrossRef Full Text | Google Scholar
48. Voets NL, Bartsch A, Plaha P. Brain white matter fibre tracts: a review of functional neuro-oncological relevance. J Neurol Neurosurg Psychiatry. (2017) 88(12):1017–25. doi: 10.1136/jnnp-2017-316170
PubMed Abstract | CrossRef Full Text | Google Scholar
49. Tanriover N, Rhoton AL, Kawashima M, Ulm AJ, Yasuda A. Microsurgical anatomy of the insula and the Sylvian fissure. J Neurosurg. (2004) 100(5):891–922. doi: 10.3171/jns.2004.100.5.0891
PubMed Abstract | CrossRef Full Text | Google Scholar
50. Türe U, Yaşargil MG, Friedman AH, Al-Mefty O. Fiber dissection technique: lateral aspect of the brain. Neurosurgery. (2000) 47(2):417–26; discussion 426-7. doi: 10.1097/00006123-200008000-00028. PMID: 10942015.
CrossRef Full Text | Google Scholar
51. Costa M, Braga VL, Yağmurlu K, Centeno RS, Cavalheiro S, Chaddad-Neto F. A technical guide for fiber tract dissection of the internal capsule. Turk Neurosurg. (2018) 28(6):934–9. doi: 10.5137/1019-5149.JTN.20884-17.1
PubMed Abstract | CrossRef Full Text | Google Scholar
52. Sincoff EH, Tan Y, Abdulrauf SI. White matter fiber dissection of the optic radiations of the temporal lobe and implications for surgical approaches to the temporal horn. J Neurosurg. (2004) 101(5):739–46. doi: 10.3171/jns.2004.101.5.0739
PubMed Abstract | CrossRef Full Text | Google Scholar
53. Serra C, Türe U, Krayenbühl N, Şengül G, Yaşargil DCH, Yaşargil MG. Topographic classification of the thalamus surfaces related to microneurosurgery: a white matter fiber microdissection study. World Neurosurg. (2017) 97:438–52. doi: 10.1016/j.wneu.2016.09.101
PubMed Abstract | CrossRef Full Text | Google Scholar
54. Martino J, Brogna C, Robles SG, Vergani F, Duffau H. Anatomic dissection of the inferior fronto-occipital fasciculus revisited in the lights of brain stimulation data. Cortex. (2010) 46(5):691–9. doi: 10.1016/j.cortex.2009.07.015
PubMed Abstract | CrossRef Full Text | Google Scholar
55. Kadri PAS, de Oliveira JG, Krayenbühl N, Türe U, de Oliveira EPL, Al-Mefty O, et al. Surgical approaches to the temporal horn: an anatomic analysis of white matter tract
留言 (0)