
記住我


Low back pain is the leading cause of disability with a significant social and economic impact around the world.13,18 There is strong evidence that chronic low back pain (CLBP) is associated with a complex interaction of biopsychosocial factors.2,3,7,16,27 Although many of these factors are potentially modifiable, most existing interventions are based on a biomedical model focusing on the structure or disease, and they do not target a patient-centered approach for each case of chronic low back pain.24
Cognitive functional therapy (CFT) is a physiotherapy-led intervention that has evolved from an integration of foundational behavioral psychology and neuroscience within the physiotherapist practice directed at the multidimensional nature of low back pain.22,25 The clinical journey is adapted to the individual's profile following 3 main components: (1) making sense of pain, (2) exposure with control, and (3) lifestyle changes.25 Vibe Fersum et al.30,31 found that CFT was significantly more effective than the combination of manual therapy and exercise for chronic low back pain and that the reduction in disability was maintained 3 years after the beginning of the study. This study had significant methodological shortcomings regarding the failure to carry out the intention to treat analysis, high risk of attrition bias, and random error.9,11 O'Keeffe et al.21 found that CFT was better than group-based exercise and education for disability. However, the high risk of attrition bias and performance bias precluded the confirmation of the CFT effectiveness for disability. Ussing et al.29 found that CFT was feasible and displayed clinically important effects for chronic low back pain in a secondary care setting. However, the participants were not randomised. Therefore, it is important to conduct clinical trials to compare CFT with other interventions but overcoming these methodological shortcomings. The present study investigated whether CFT is more effective than CORE-MT in pain and disability over the 8 weeks of treatment in patients with CLBP.
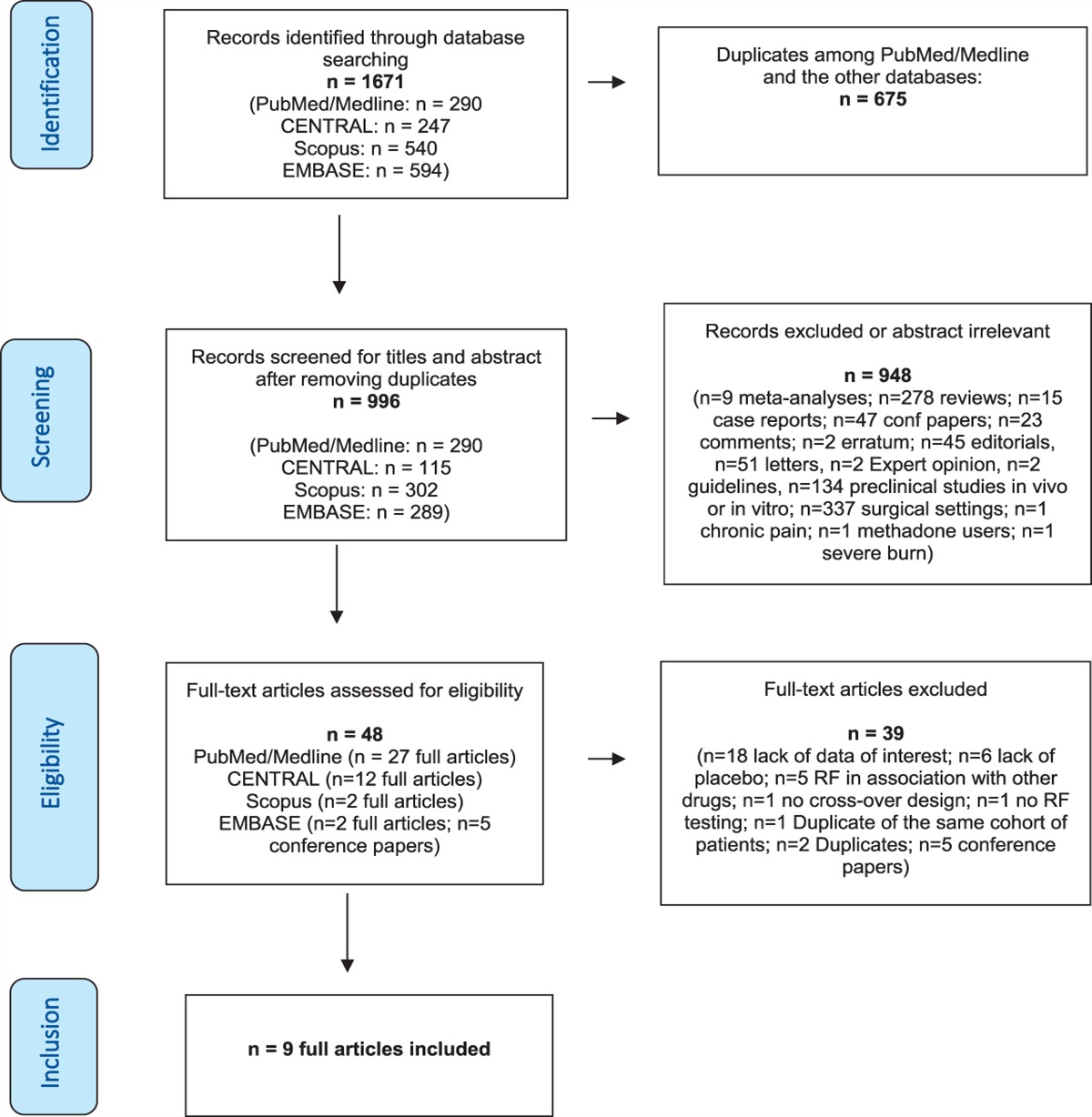
2. Methods 2.1. Study designThis is a parallel-group, randomised, controlled trial conducted in the physiotherapy department of a private orthopedic clinic in Campinas, São Paulo, Brazil (Fig. 1). Individuals with CLBP were recruited by referral of physicians and social media from September 2017 to June 2019, with 12-month follow-up ending in June 2020. A total of 4 physiotherapists, one in the CFT group and 3 in the control group, delivered the interventions in this trial. The trial was prospectively registered and was first available on ClinicalTrials.gov on September 6, 2017. The last participant's data were collected on June 28, 2020 (Registration number: NCT03273114). The full protocol manuscript is available online (https://doi.org/10.21203/rs.3.rs-1438806/v1). The trial was reported following the CONSORT statement.17
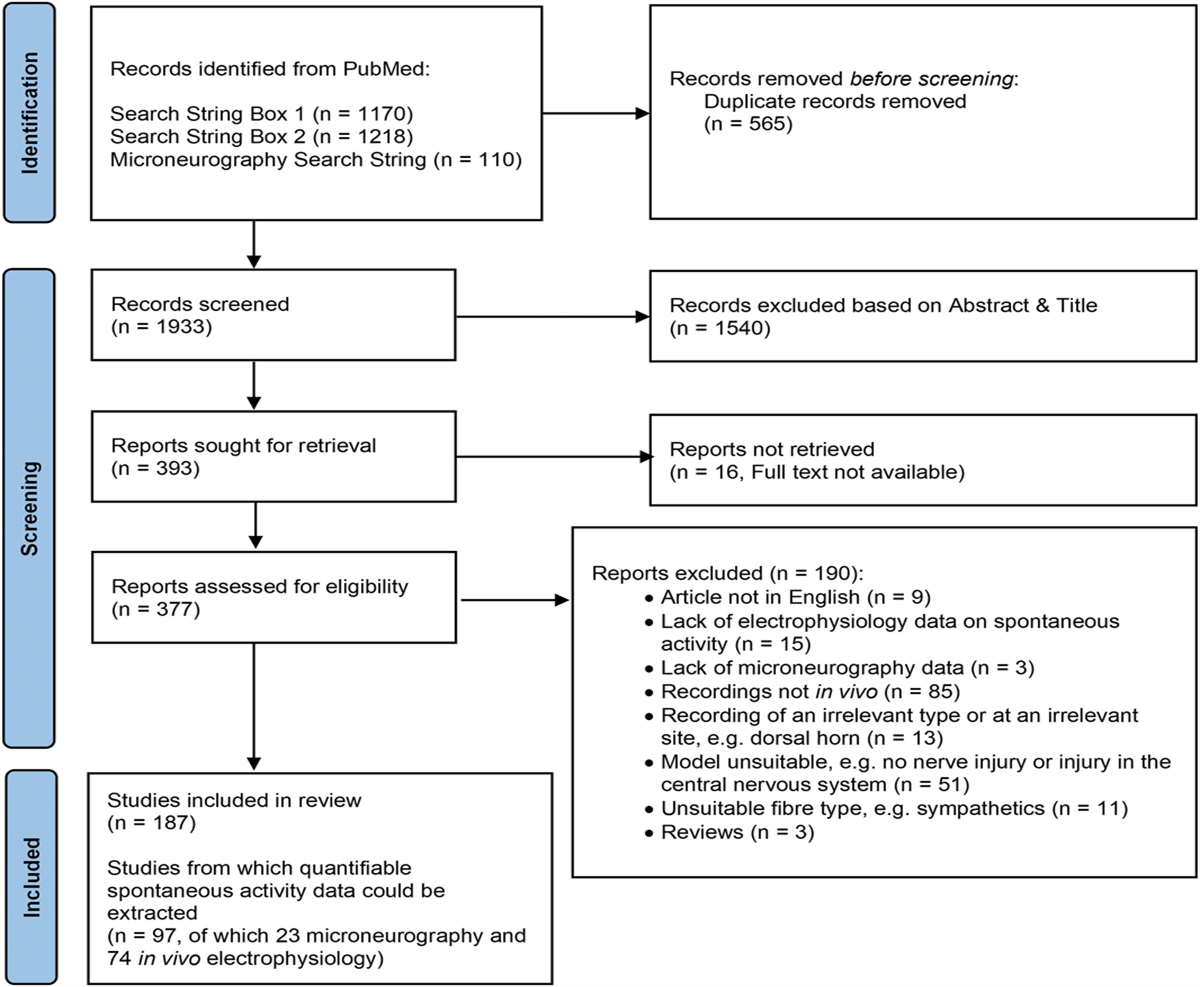
 Figure 1.:
Figure 1.: Recruitment of participants, exclusions, and randomisation of patients with chronic low back pain included in the study and follow-ups.
2.2. ParticipantsParticipants aged 18 to 65 years, were independently mobile (with or without aids), were seeking treatment for low back pain with at least 12 weeks of duration, and were able to speak and understand Portuguese. Following Vibe Fersum et al.30 and O'Keeffe et al.21 criteria, a score greater than 14% on Oswestry Disability Index (ODI) was required for inclusion. Participants were excluded if the primary pain area was not the lumbar spine (from T12 to buttocks); if leg pain was the primary problem (eg, nerve root compression or disc prolapse with true radicular pain/radiculopathy, lateral recess or central spinal stenosis); if the patient underwent invasive pain relieving procedures such as injection-based therapy (eg, epidurals) and day case procedures (eg, rhizotomy) in the past 3 months; if they were pregnant; if they had rheumatological/inflammatory disease (eg, rheumatoid arthritis, ankylosing spondylitis, psoriatic arthritis, lupus erythematosus, Scheuermann disease) or progressive neurological disease (eg, multiple sclerosis, Parkinson's disease, motor neuron disease); if they had scoliosis (if considered the primary driver of pain); if they had unstable cardiac conditions; or if they had red flag disorders like malignancy/cancer, acute traumas like fracture (less than 6 months ago), infection, or spinal cord compression/equine tail.
A physiotherapist, who was unaware of the treatment allocation, screened the patients to confirm eligibility starting by the ODI. If the participants scored more than 14% on the ODI and consented to participate in the study, then they completed the remaining sections of the baseline questionnaire before randomisation. The first intervention session was within 1 week of randomisation. Eligible patients were informed about the study's objectives and procedures. All study assessors, both baseline and follow-up, were equally trained to apply the self-reported questionnaires.
2.3. Randomisation and blindingA computer-generated allocation sequence was used to allocate participants to receive either CFT or CORE-MT. The allocation sequence was arranged using a block randomisation model (size of 4) by an independent investigator and concealed in 148 sequentially numbered, sealed, and opaque envelopes. Immediately before the assignment to the treatment group and after the patient signed the informed consent to participate in the study, the treating clinicians opened the envelope to reveal the group allocation. It was not possible to blind the participants and the treating clinicians. The assessors were not considered blinded because participants were not blinded and outcomes were self-reported. However, to guarantee that the treatment expectation was evenly balanced between the groups and decrease measurement bias, the participants did not know the study hypothesis, and the assessors did not know the participant's intervention group. The statistician was blinded to the group allocation.
2.4. InterventionsWe have followed the template for intervention description and replication (TIDieR) checklist to describe the interventions.12 Both interventions were face to face and individualized, in a room reserved for the session of only 1 patient at a time. The treatments were 5 one-hour sessions for an 8-week intervention period, on a weekly basis for the first 2 weeks and then a session every 2 or 3 weeks. Participants were always treated by the same physical therapist who was not involved in the reassessments of participants. Prescribed exercises were filmed, written, or delivered via booklet by the physiotherapist so that participants could perform them at home regularly. The assessment of treatment fidelity was performed by in vivo observations as well as video recording during the pilot study and along the trial. Also, regular meetings to discuss these clinical cases were performed. Both groups were monitored and had adequate adherence to the treatment that was performed as planned.
2.4.1. Cognitive functional therapyCognitive functional therapy is an integrated and flexible behavioral approach developed to reduce pain and disability in people with chronic low back pain. There were 3 main components in the intervention, according to O'Sullivan et al.25 and Caneiro et al.4: Making sense of pain, exposure with control, and lifestyle change.
Making sense of pain is a reflective process that uses a patient's own story and relevant life events, combined with their experiences during behavior exposure to not only achieve a new understanding of their pain but also increase self-efficacy to reach their goals. A timeline of the pain history recalling biopsychosocial factors that may have played a role in the rise and persistence of the symptoms can help patients make sense of their chronic low back pain and disability. Listening to the patient's history is key to identify the context, area and characteristics of pain, level of disability, beliefs, physical factors, coping strategies, lifestyle factors, goals, and values. Therapeutic alliance is enhanced with elements such as empathy, mirroring, reflective issues, and reinforcement of positive behaviors. The patients develop an understanding of the contexts in which pain flare-ups occur, and therefore, positive coping strategies could be determined and discussed. Afterward, a summary of what was discussed is reviewed with the patient.
Exposure with control is a process of behavior change that allows individuals to gradually return to their valued functional activities without pain escalation and associated distress. It aims at focusing the experience of pain as a hypothesis for testing behavioral experiments using the experience of pain where possible. For instance, “lifting with a flexed spine will increase my pain.” An experience in which learned associations between threatening tasks and increased pain or harm may be corrected and new “safety” associations are formed. This strategy comes from the assumption that the discrepancy between expectancy and experience (expectancy violation) is helpful for new learning. For some individuals, the objective is to experience less pain during task performance, while for others, it may be getting involved with the feared and avoided tasks without damage. In this process, sympathetic responses and safety-seeking behaviors that happen during the performance of painful, feared, or avoided functional tasks are specifically targeted and controlled to create a mismatch between the individual's expected and actual pain responses. For instance, prior individual expectation: “I expect my pain will increase with repeated lifting. Individual experience”: “When I relax, breathe and bend my back without protecting it, my pain does not get worse—it alleviates.” Exposure with control includes promotion of body relaxation before exposure, reduction of protective behaviors, and encouragement of body awareness and control that enables the individual to experience functional activities in nonprotective ways. As an example, lifting in a relaxed manner and modifying how the individual physically performs the task without unhelpful protective responses (ie, bracing, breath holding, avoidance of spinal flexion) may result in a positive experience that promotes safety learning.
Lifestyle change is to help patients adopt a healthy lifestyle. Strategies for changing unfavorable lifestyle behaviors are discussed as part of making sense of pain. Physical activity is based on a person's preferences linked to individual goals considering costs, accessibility issues, and social engagement to stimulate enduring behavior change. Sleep deficits associated with by poor sleep hygiene are addressed establishing a daily routine and reducing the use of electronic in bed. Disturbances due to pain, worry, and stress may be managed with techniques of relaxation (ie, guided meditation) and engaging in regular physical activity. Specific training of rolling and posturing in bed in a relaxed way is explored when movement and postures in bed are an issue.
Participants randomised in the CFT group were treated by a newly graduated physiotherapist with 1 year of clinical experience in CFT. She attended 3 CFT workshops with 3 tutors of the method and completed 106 hours of training, including workshops, patient examinations, and a pilot study with the supervision of a physiotherapist with more than 4 years of clinical experience in CFT.
2.4.2. Core training exercise and manual therapyThe participants assigned to the comparison group were treated with a strengthening program to maximize static core muscle endurance and dynamic core stability, based on McGill core exercises.20The approach consisted of trunk, abdominal, and pelvic strengthening in different functional positions and was progressive in relation to difficulty and intensity. Before core endurance exercises, flexion-extension motion was performed by slowly cycling through full spine flexion to full extension in 4-point kneeling (cat–camel exercise) and the basic abdominal brace was taught in a relaxed neutral spine position. Core endurance exercises included bridge exercises (bridge, prone bridge, and side bridge), 4-point kneeling exercises (ie, bird–dog), and supine exercises (ie, dead bug, curl-up). Core muscles were maintained active to control the lumbar spine and pelvic girdle during multiplanar arm and leg movements (ie, lunges, hip abduction). A list including the detailed description of the main exercises is provided in the supplementary material (available at https://links.lww.com/PAIN/B612). The prescription of the exercises was individualized, and the exercises were performed with resistance (elastic bands, dumbbell, or ankle weights) and on unstable surfaces according to the progress of each patient. The physiotherapists of this group provided instruction, demonstration, and individual feedback for the exercises during the sessions. Patients were instructed and encouraged to perform a 30-minute exercise session at home including 2 to 3 sets of 6 to 12 repetitions holding the isometric contraction for 3 to 10 seconds of each prescribed exercise 3 times a week. The manual therapy interventions were joint mobilization or manipulation (thrust)15 and mobilization with movement techniques14 to the spine or pelvis. These interventions were used pragmatically whenever the therapist judged necessary, with the aim of restoring optimal motion, reducing pain, and facilitating core exercises progression. Participants in the CORE-MT group were treated by 3 physiotherapists with at least 5 years of clinical experience in manual therapy and core training exercises with no prior training in CFT.
2.5. OutcomesThe primary outcomes were pain intensity (on a numerical pain-rating scale from 0 to 10, with 0 indicating no pain and 10 the worst possible pain) and disability associated with low back pain measured on the Oswestry Disability Index (scores ranged from 0 to 100) 8 weeks after first intervention session (postintervention).6,32 Secondary outcomes were pain intensity and disability assessed 6 and 12 months after the first intervention session. Additional secondary outcomes were global perceived effect measured on Global Perceived Effect Scale (current symptoms as compared with baseline, on a scale from −5 [vastly worse] to 0 [unchanged], to +5 [completely recovered]), and patient satisfaction measured on the patient satisfaction questionnaire (1 = satisfied, 2 = just a little satisfied, 3 = neither satisfied nor dissatisfied, 4 = just a little dissatisfied, 5 = dissatisfied) at 8 weeks and 6 and 12 months after intervention.10,33
Other data that were collected included baseline sociodemographic information, symptoms duration, number of pain areas, family history of low back pain, MRI scans performed, back surgery, paid work, and chronicity risk (Örebro Musculoskeletal Pain Questionnaire [OMPQ] and and StarT back screening tool [SBST]).8,26
Outcomes were assessed at 8 weeks (primary end points), 6 months, and 12 months by means of telephone contact by 2 blinded assessors (1 physiotherapist and 1 physical educator) trained by the principal researcher during a pilot study. They did not treat any of the participants nor were aware of their group allocation or received any information regarding the treatment arm of the participants. Also, both assessors did not have access to the place where the treatment was administered or the waiting room.
2.6. Sample size calculationWe determined that a minimum sample size of 148 participants (74 per group) would be required to provide the trial with 80% power to detect a between-group difference of 1.0 point for pain intensity and 5 points for disability (ODI) at 8 weeks. We performed the sample size calculation with lower values than what is considered clinical important changes to generate a larger statistical precision.23 Assumptions for the pain intensity and disability included a 2-sided alpha level of 0.05 and a mean standard deviation of 2.0 for pain and 10% for disability. The estimated sample size also allowed a limit of 15% loss of follow-up.
2.7. Statistical analysesAnalyses were performed by a statistician who received the encoded data and were based on intention-to-treat principles. Missing data were assumed to be missing completely at random. Multiple imputation was used to account for these missing data.28 Missing values in outcome variables were estimated using multiple imputation by chained equations after 50 replicated imputed data sets. Variables included in the multiple imputation process included (1) group factor, (2) time factor, and (3) the respective outcome variable. Descriptive statistics was used to describe the characteristics of the participants in both treatment groups. Two-sided P values of less than 0.05 were considered to indicate statistical evidence of significance. The outcomes pain intensity, disability, and global perceived effect were analyzed using repeated-measure linear mixed models (participants and time as random factors) that included all the scores that were reported after randomisation with the baseline scores as covariates. Adjusted mean differences were tested at week 8, 6 months, and 12 months. Multiple comparisons were performed using the Tukey test with P values adjusted using the Holm procedure. The variable patient satisfaction was compared by ridit analysis of the ordered categorical data. Effect sizes for primary and secondary outcomes (except patient satisfaction) were calculated as Cohen d from estimated marginal means and standard error estimates from the primary adjusted analysis. Effect sizes were interpreted according to Cohen criteria (small ≤ 0.2; moderate = 0.5; large ≥ 0.8).5 All analyses were performed using the RStudio version 0.99.486 and packages “nlme,” “emmeans,” “mice,” “miceadds,” “mitml,” “multicomp,” “stddiff,” and “ridittools” (supplementary material, available at https://links.lww.com/PAIN/B612).
3. Results 3.1. Recruitment and baseline dataA total of 148 participants from an orthopedic clinic underwent randomisation; 74 participants were randomly assigned to the CFT group and 74 to the CORE-MT group (Fig. 1). Altogether, 97.3% (n = 72) of participants in each intervention group completed the 8 weeks of the trial; 97.3% (n = 72) of participants in the CFT group and 94.6% (n = 70) of participants in the CORE-MT group completed the 6 months of the trial; 95.9% (n = 71) of participants in the CFT group and 89.2% (n = 66) completed the 1 year of the trial.
The characteristics of the participants at baseline are presented in Table 1. Participants were mainly middle aged, predominantly female, and had paid work. The median of low back pain duration was 60 months, and the median of the number of pain sites was 5. The majority of participants scored a high risk of chronicity on OMPQ (62.84%), which was the same for both groups, as well as family history of low back pain (75.86%) and MRI scan performed for low back pain (82.76%). The mean number of treatments (SD) was similar in both groups (CFT: 4.24 [1.17] vs CORE-MT: 4.23 [1.22]).
Table 1 - Characteristics of the patients at baseline. Characteristic CFT group CORE-MT group Female sex—n (%) 44 (59.46) 47 (63.51) Age—y; mean (±SD) 46.39 ± 10.62 40.43 ± 11.55 Height—m 1.69 ± 10.34 1.69 ± 9.75 Weight—kg 77.49 ± 12.02 78.06 ± 16.45 Paid work—n (%) 62 (83.78) 56 (75.68) Disability (ODI) 30.66 ± 10.82 26.98 ± 9.44 Pain intensity (NPS) 5.78 ± 1.71 5.58 ± 1.84 Duration of LBP—months (median, IQR) 72 (120) 48 (72) Low back surgery—n (%) 6 (8.22) 4 (5.56) No of pain sites—(median, IQR) 5 (6.25) 5 (5) Family history of LBP—n (%) 54 (73.97) 56 (77.77) MRI scan performed—n (%) 60 (82.19) 60 (83.33) Risk of chronicity, Örebro (0-100) 53.70 ± 11.21 53.36 ± 12.18 Risk of chronicity, StarTback—n (%) Low risk 17 (22.97) 21 (28.38) Medium risk 34 (45.95) 35 (47.29) High risk 23 (31.08) 18 (24.32)Data of the variables family history, MRI scan performed and low back surgery of one participant in the CFT group and of 2 participants in the control group were missing.
CFT, cognitive functional therapy; CORE-MT, core training exercise and manual therapy; LBP, low back pain; NPS, numerical pain rating scale; ODI, Oswestry Disability Index.
In the analysis of primary outcomes, CFT was more effective than CORE-MT in disability at 8 weeks (MD = −4.75; 95% CI −8.38 to −1.11; P = 0.011; effect size = 0.55). This study found no difference between groups in pain intensity (MD = −0.04; 95% CI −0.79 to 0.71; P = 0.916) (Table 2 and Fig. 2).
Table 2 - Unadjusted mean (SD) for each numeric outcome, including primary outcomes (pain intensity and disability at 8 weeks) and secondary outcomes (pain intensity and disability at 6 and 12 months, and global recovery), by treatment group and adjusted between-group mean differences for each follow-up time point. Baseline 8 wk 6 mo 12 mo CFT (n = 74) CORE-MT (n = 74) CFT (n = 72) CORE-MT (n = 72) Adjusted between-group mean difference (95% CI) Effect size as SMD* CFT (n = 72) CORE-MT (n = 70) Adjusted between-group mean difference (95% CI) Effect size as SMD* CFT (n = 71) CORE-MT (n = 66) Adjusted between-group mean difference (95% CI) Effect size as SMD* Pain intensity (0-10) 5.78 (1.70) 5.58 (1.84) 3.57 (2.46) 3.51 (2.31) −0.04 (−0.79 to 0.71) 0.07 3.82 (2.56) 4.16 (2.53) −0.25 (−1.12 to 0.62) 0.14 3.92 (2.44) 3.52 (2.35) 0.29 (−0.54 to 1.11) 0.19 Disability (0-100) 30.66 (10.82) 26.98(9.44) 17.48 (13.43) 20.25 (11.43) −4.75 (−8.38 to −1.11)† 0.55 17.35 (12.41) 18.90 (10.37) −2.98 (−6.45 to 0.48) 0.43 18.21 (13.28) 17.67 (12.40) −1.43 (−5.45 to 2.58) 0.22 Global recovery (−5 to +5) — — 2.76 (1.80) 2.42 (1.70) 0.34 (−0.33 to 1.01) 0.19 2.17 (2.32) 2.13 (2.28) 0.06 (−0.63 to 0.74) 0.02 2.07 (2.24) 2.35 (1.96) −0.25 (−0.94 to 0.44) 0.13*Standardized mean difference (SMD) calculated from marginal estimates (Cohen d).
†P < 0.05.
CFT, cognitive functional therapy; CORE-MT, core training exercise and manual therapy.
 Figure 2.:
Figure 2.: Mean pain intensity (left) and disability (right) for CFT and CORE-MT groups. CFT, cognitive functional therapy; CORE-MT, core training exercise and manual therapy.
3.3. Secondary outcomesIn the analysis of numeric secondary outcomes (Table 2), this study found no difference between groups in pain intensity at 6 months (MD = −0.25; 95% CI −1.12 to 0.62, P = 0.576) or in disability at 6 months (MD = −2.98; 95% CI −6.45 to 0.48, P = 0.091) (Fig. 2). There was no difference between groups in pain intensity (MD = 0.29: 95% CI −0.54 to 1.11, P = 0.494) or disability (MD = −1.43: 95% CI −5.45 to 2.58, P = 0.484) at 12 months (Fig. 2). No difference was found between groups in global perceived effect at 8 weeks (MD = 0.34; 95% CI −0.33 to 1.01, P = 0.32), at 6 months (MD = 0.06; 95% CI −0.63 to 0.74, P = 0.873), or 12 at months (MD = −0.25; 95% CI −0.94 to 0.44, P = 0.481). Also, no difference was found between group in patient satisfaction (Table 3). No serious adverse events related to the interventions were reported.
Table 3 - Secondary outcome patient satisfaction. Patient satisfaction, n (%) CFT group CORE-MT group 1 2 3 4 5 1 2 3 4 5 At 2 mo 63 (87.50%) 6 (8.33%) 1 (1.39%) 1 (1.39%) 1 (1.39%) 58 (81.69%) 8 (11.27%) 4 (5.63%) 1 (1.41%) 0 (0.00%) z = 0.597, P = 0.550 At 6 mo 53 (73.61%) 10 (13.89%) 6 (8.33%) 3 (4.17%) 0 (0.00%) 47 (67.14%) 12 (17.14%) 7 (10.00%) 3 (4.29%) 1 (1.43%) z = 0.683, P = 0.494 At 1 y 53 (74.65%) 10 (14.08%) 8 (11.27%) 0 (0.00%) 0 (0.00%) 45 (68.18%) 7 (10.61%) 11 (16.67%) 1 (1.52%) 2 (3.03%) z = 0.889, P = 0.374Patient satisfaction: (1-5), 1 = completely satisfied, 2 = a little bit satisfied, 3 = neither satisfied or dissatisfied, 4 = a little bit dissatisfied, 5 = completely dissatisfied.
CFT, cognitive functional therapy; CORE-MT, core training exercise and manual therapy.
This randomised clinical trial showed that CFT reduced disability, but the difference was not clinically important compared with CORE-MT post-intervention (short term) in patients with CLBP. There was no difference in pain intensity between interventions, and the treatment effect was not maintained in the mid-term and long-term follow-ups.
4.2. Comparison with other trialsO'Keeffe et al.21 found a reduction in disability at 6 months and at 1-year follow-ups when CFT was compared with a group exercise and education but with a loss of follow-up of 30% of participants. It is difficult to compare O'Keeffe et al. trial findings to our findings because the authors did not present the results postintervention. However, the high risk of attrition bias of O'Keeffe et al. trial may explain why our trial failed to replicate the reduction in disability at 6 months and 1-year follow-ups. The same therapist applying both interventions combined with the longer period of the CFT group treatment may have generated performance bias and inflate the effect size.
Vibe Fersum et al.30 also found a reduction in disability (MD = −9.7; 95% CI −12.7 to −6.7) with an effect size greater than in our trial, but contrary to our trial and the O'Keeffe et al. trial, they showed a reduction in pain intensity (MD = −2.1; 95% CI −2.7 to −1.4). The greater effect size and the reduction in pain intensity may be because the study of Vibe Fersum et al. was vulnerable not only because of the high risk of bias but also because of the high risk of random error due to the small sample size (n = 94). There was a substantial violation of intention-to-treat principles with the exclusion of 27 of 121 participants before the 3-month follow-up.
Contrary to the O'Keeffe et al. and Vibe Fersum et al. trials, in our trial, the reduction in disability was not maintained at 6 and 12 months. In addition to the high risk of attrition bias as opposed to the low risk in our trial, there are other factors that may explain the difference in the results between studies. Besides, the newly graduated physiotherapist in the CFT group in our trial; the mean of treatments was 4.2 over 8 weeks, vs 7.7 over 12 weeks in the Vibe Fersum trial, and 5.0 over 13.7 weeks in the O'Keeffe trial. The higher number of treatments and weeks patients were receiving care could have prolonged the effect of treatment. Our results suggest that a booster session at 6 months may be necessary to prolong the treatment effect.11
Other biopsychosocial approaches that are in line with CFT presented promising results in recent clinical trials.1,19 Ashar et al.1 compared pain reprocessing therapy (PRT) with an open-label placebo and usual care for chronic low back pain and found large reduction in pain intensity that continued at 1-year follow-up. The aim of this approach was to promote patients' reconceptualization of primary (nociplastic) chronic pain as a brain-generated false alarm using cognitive, somatic, and exposure-based techniques. Malfiet et al.19 showed that pain neuroscience education combined with cognition-targeted motor control training reduced pain intensity and disability with medium to large effect sizes compared with traditional back and neck education and general exercises for chronic spinal pain. Similarly, to the second component of CFT, cognition-targeted motor training was based on movements participants feared and avoided that were introduced using a graded approach with the progression toward physically, cognitively, and psychosocially demanding situations.
4.3. Clinical implicationsCognitive functional therapy reduced disability compared with core exercise and manual therapy for patients with chronic low back pain postintervention. However, this effect was not clinically important and was not maintained at mid- and long-term follow-up.
4.4. Strengths and limitations of the studyThe present trial has several strengths and limitations. Our research group is independent of the group that developed CFT. Our trial was the first trial on CFT conducted outside Europe and in an upper-middle-income country. The study followed the prespecified protocol without substantial violations. The 3 physiotherapists of the comparison group were used to treating patients using core exercises and manual therapy and did not attend any CFT workshop. The primary outcomes were the ones prespecified in the registered protocol and our trial achieved a very low loss of follow-up of participants in the time point of the primary outcomes (2.7% vs 37% in the O'Keeffe et al.21 trial and 22.5% in the Vibe Fersum et al.30 trial) as well as at 6 months (4% vs 28% in the O'Keeffe et al. trial and 22.5% in the Vibe Fersum et al. trial) and at 12-month follow-ups (7.5% vs 31% in the O'Keeffe et al. trial and 22.5% in the Vibe Fersum et al. trial). Opposed to the Vibe Fersum et al. trial, our trial did not violate intention-to-treat principles.
There are some limitations. There was a slight random imbalance in the distribution of some variables in the characteristics of the sample (eg, disability). This was not a statistical issue because the primary outcome disability postintervention was adjusted by the baseline value of the same variable for the linear mixed model. However, it seems that the block randomisation (size of 4) of 148 participants in 2 groups of 74 is still small to ensure balance of baseline characteristics and eliminates selection bias. It was not possible to blind assessors because the outcomes were self-reported and the participants were not blinded. The study was conducted in one clinic in Brazil, which may limit generalizability.
5. ConclusionTreatment with CFT reduced disability, but the difference was not clinically important compared with CORE-MT postintervention (short term) in patients with CLBP. There was no difference in pain intensity between interventions, and the treatment effect was not maintained in the mid-term and long-term follow-ups.
Conflict of interest statementThe authors have no conflict of interest to declare.
Appendix A. Supplemental digital contentSupplemental digital content associated with this article can be found online at https://links.lww.com/PAIN/B612.
AcknowledgementsThe Coordenação de Aperfeiçoamento de Pessoal de Nível Superior—Brasil (CAPES)—(Finance code 001) scholarship were received in support of this work. The funding source played no role in the study design, collection, analysis, and interpretation of the data, nor in the writing of the manuscript and in the decision to submit the manuscript for publication.
This study was presented and published as a conference abstract at the 2021 Back and Neck Pain Forum.
Authors contributions: All authors contributed to the concept and design of the study. J. Castro was the therapist of CFT group and was involved in setting the writing article assisted by N. Meziat-Filho, L. Correia, F.J.J. Reis, and L.C. Nogueira. N. Meziat-Filho also contributed in data interpretation and statistical analysis strategy. M.J. Pellegrini was one of the assessors. B.S. Donato, B. Arruda, and F. Agulhari were the therapists of the CORE-MT group. Statistical analysis was performed by A.S. Ferreira. F.T.C. Belache, C.P. Sousa, and J. Fernandez contributed to the critical revision of the article. All authors read and approved the final version of the article.
This study was approved by the Research Ethics Committee of Centro Universitário Augusto Motta Ethics Committee (approval number: 2219742). All patients signed the informed consent form prior to participation.
References [1]. Ashar YK, Gordon A, Schubiner H, Uipi C, Knight K, Anderson Z, Carlisle J, Polisky L, Geuter S, Flood TF, Kragel PA, Dimidjian S, Lumley MA, Wager TD. Effect of pain reprocessing therapy vs placebo and usual care for patients with chronic back pain: a randomized clinical trial. JAMA Psychiatry 2022;79:13–23. [2]. Briggs AM, Jordan JE, O'Sullivan PB, Buchbinder R, Burnett AF, Osborne RH, Straker LM. Individuals with chronic low back pain have greater difficulty in engaging in positive lifestyle behaviours than those without back pain: an assessment of health literacy. BMC Musculoskelet Disord 2011;12:161. [3]. Campbell P, Bishop A, Dunn KM, Main CJ, Thomas E, Foster NE. Conceptual overlap of psychological constructs in low back pain. PAIN 2013;154:1783–91. [4]. Caneiro JP, Smith A, Bunzli S, Linton S, Moseley GL, O'Sullivan P. From fear to safety: a roadmap to recovery from musculoskeletal pain. Phys Ther 2022;102:pzab271. [5]. Cohen J. Statistical Power Analysis for the Behavioral Sciences. 2nd ed. Hillsdale, NJ: Lawrence Erlbaum Associates, Publishers, 1988. [6]. Costa LOP, Maher CG, Latimer J, Ferreira PH, Ferreira ML, Pozzi GC, Freitas LMA. Clinimetric testing of three self-report outcome measures for low back pain patients in Brazil: which one is the best? Spine 2008;33:2459–63. [7]. Dankaerts W, O'Sullivan P, Burnett A, Straker L, Davey P, Gupta R. Discriminating healthy controls and two clinical subgroups of nonspecific chronic low back pain patients using trunk muscle activation and lumbosacral kinematics of postures and movements: a statistical classification model. Spine (Phila Pa 1976) 2009;34:1610–8. [8]. Fagundes FRC, Costa LOP, Fuhro FF, Manzoni ACT, de Oliveira NTB, Cabral CMN. Örebro Questionnaire: short and long forms of the Brazilian-Portuguese version. Qual Life Res 2015;24:2777–88. [9]. Fernandez J, Ferreira ADS, Castro J, Correia LCL, Meziat-Filho N. Comment on the paper “Cognitive functional therapy in patients with non specific chronic low back pain,” by Vibe Fersum et al. Eur J Pain 2019;23:1574–5. [10]. Fischer D, Stewart AL, Bloch DA, Lorig K, Laurent D, Holman H. Capturing the patient's view of change as a clinical outcome measure. JAMA 1999;282:1157–62. [11]. George SZ. Commentary on “cognitive functional therapy in patients with non-specific chronic low back pain”. Eur J Pain 2019;23:1401–2. [12]. Hoffmann TC, Glasziou PP, Boutron I, Milne R, Perera R, Moher D, Altman DG, Barbour V, Macdonald H, Johnston M, Lamb SE, Dixon-Woods M, McCulloch P, Wyatt JC, Chan AW, Michie S. Better reporting of interventions: template for intervention description and replication (TIDieR) checklist and guide. BMJ 2014;348:g1687. [13]. Hoy D, March L, Brooks P, Blyth F, Woolf A, Bain C, Williams G, Smith E, Vos T, Barendregt J, Murray C, Burstein R, Buchbinder R. The global burden of low back pain: estimates from the Global Burden of Disease 2010 study. Ann Rheum Dis 2014;73:968–74. [14]. Hussien HM, Abdel-Raoof NA, Kattabei OM, Ahmed HH. Effect of mulligan concept lumbar SNAG on chronic nonspecific low back pain. J Chiropr Med 2017;16:94–102. [15]. Kirkaldy-Willis WH, Cassidy JD. Spinal manipulation in the treatment of low-back pain. Can Fam Physician 1985;31:535. [16]. Lee H, Hübscher M, Moseley GL, Kamper SJ, Traeger AC, Mansell G, McAuley JH. How does pain lead to disability? A systematic review and meta-analysis of mediation studies in people with back and neck pain. PAIN 2015;156:988–97. [17]. Lepage L, Altman DG, Schulz KF, Moher D, Egger M, Davidoff F, Elbourne D, Gøtzsche PC, Lang T. The revised CONSORT statement for reporting randomized trials: explanation and elaboration. Ann Intern Med 2001;134:663–94. [18]. Maher C, Underwood M, Buchbinder R. Non-specific low back pain. Lancet 2017;389:736–47. [19]. Malfliet A, Kregel J, Coppieters I, de Pauw R, Meeus M, Roussel N, Cagnie B, Danneels L, Nijs J. Effect of pain neuroscience education combined with cognition-targeted motor control training on chronic spinal pain: a randomized clinical trial. JAMA Neurol 2018;75:808–17. [20]. McGill SM. Low back stability: from formal description to issues for performance and rehabilitation. Exerc Sport Sci Rev 2001;29:26–31. [21]. O'Keeffe M, O'Sullivan P, Purtill H, Bargary N, O'Sullivan K. Cognitive functional therapy compared with a group-based exercise and education intervention for chronic low back pain: a multicentre randomised controlled trial (RCT). Br J Sports Med 2020;54:782–9. [22]. O'Keeffe M, Purtill H, Kennedy N, O'Sullivan P, Dankaerts W, Tighe A, Allworthy L, Dolan L, Bargary N, O'Sullivan K. Individualised cognitive functional therapy compared with a combined exercise and pain education class for patients with non-specific chronic low back pain: study protocol for a multicentre randomised controlled trial. BMJ Open 2015;5:e007156. [23]. Ostelo RW, Deyo RA, Stratford P, Waddell G, Croft P, von Korff M, Bouter LM, de Vet HC. Interpreting change scores for pain and functional status in low back pain: towards international consensus regarding minimal important change. Spine (Phila Pa 1976) 2008;33:90–4. [24]. O'Sullivan P. It's time for change with the management of non-specific chronic low back pain. Br J Sports Med 2012;46:224–7. [25]. O'Sullivan PB, Caneiro JP, O'Keeffe M, Smith A, Dankaerts W, Fersum K, O'Sullivan K. Cognitive functional therapy: an inte
留言 (0)