
記住我
The intestinal epithelium balances a multiplicity of roles in early life. It facilitates the digestion and absorption of nutrients and forms a barrier against potential pathogens in the intestinal lumen. These functions must be maintained during a period of rapid growth and intestinal development. When these processes are interrupted, infant health is negatively impacted. Clinically significant intestinal pathologies that arise when the barrier function of the intestine is compromised in the neonatal period include necrotizing enterocolitis (NEC), sepsis, and infectious diarrheal illness.
In this review, we discuss intestinal morphogenesis, mechanisms of epithelial cell differentiation from intestinal stem cells (ISCs), and the function of the predominant epithelial cell subtypes in the intestine. We also discuss how disruption of the intestinal epithelium is implicated in neonatal disease with a focus on NEC, the most common intestinal pathology in preterm neonates.
Formation of crypt-villus intestinal architectureMature intestinal structure develops through a highly regulated process that begins in utero. The small intestine is composed of crypts and villi lined by a continuous epithelial cell monolayer. Structural maturation of the intestine involves lengthening of villi, deepening of crypts, and localization of proliferating ISCs in the crypt base (Fig. 1). Intestinal crypts and villi develop in human fetuses from 8–24 weeks gestation with an increase in crypt depth and villus height with advancing gestational age1. Similarly, at 9 weeks gestation, proliferating cells are detected throughout the intestine, but these cells localize to their final destination of the crypt base as gestation progresses1. Development of the crypt-villus structure is influenced by a complex pattern of growth factors provided by surrounding mesenchymal cells and amniotic fluid2,3,4. Mechanical distension has also been implicated in intestinal morphogenesis. For example, flow of amniotic fluid through the intestinal lumen in utero is required for the formation of normal intestinal structure, as the development of crypts and villi is impeded in human fetuses with intestinal obstructions such as esophageal or intestinal atresia1,5. Development of the crypt-villus architecture leads to the formation of unique microenvironments that allow for the differentiation of intestinal stem cells (ISCs) into multiple epithelial subtypes, including enterocytes (also named intestinal epithelial cells, IECs), Paneth cells, goblet cells, enteroendocrine cells, tuft cells, and microfold (M) cells. These processes will be discussed in detail below.
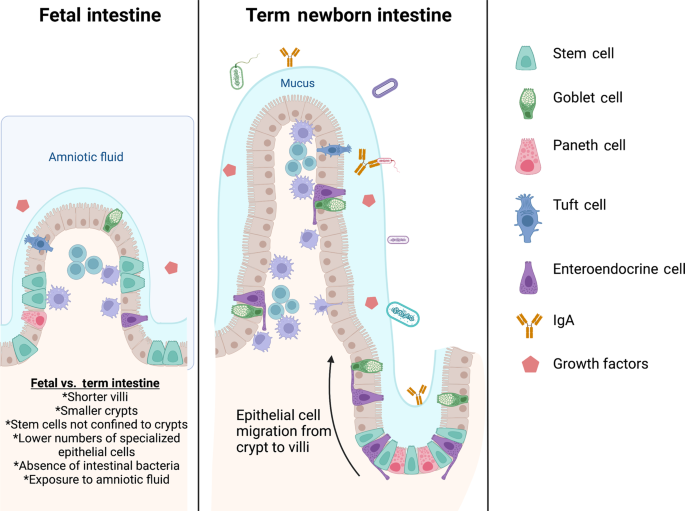
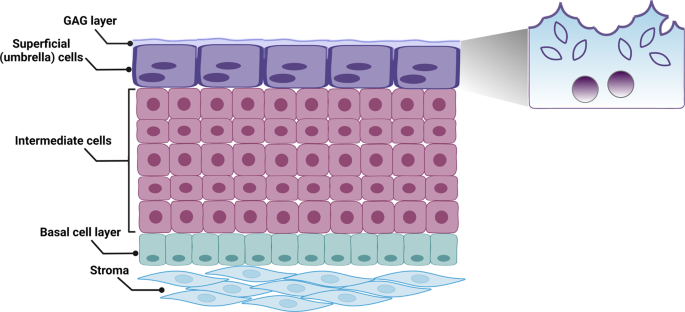
Fig. 1: Comparison of the small intestinal epithelium in the fetus and term neonate.
In utero, the intestinal epithelium is exposed to amniotic fluid, which contains growth factors essential for proper intestinal development. The crypt and villus structures mature with increasing gestational age and Lgr5+ intestinal stem cells transition from localization throughout the intestine to the intestinal crypt. Goblet cells and Paneth cells also increase in number throughout fetal development and early life, leading to increased mucus formation and antimicrobial peptide production. Both beneficial and pathogenic microorganisms can be found in the intestinal lumen as the microbiome develops after delivery. Secretory IgA provided by breast milk is a central component of the immune repertoire of the developing intestine and is crucial for establishing control of intraluminal bacteria. Figure created with Biorender.com.
Intestinal stem cells (ISCs)ISCs are the precursor from which all other intestinal epithelial cells differentiate1,6,7. ISCs are located at the base of intestinal crypts and identified by the expression of Leucine-rich repeat-containing G-protein coupled receptor 5 (Lgr5) once mature intestinal architecture is achieved1,6,7. Upon differentiation from ISCs, most epithelial subtypes migrate from the crypt up the intestinal villus6. The exception to this rule is Paneth cells, which migrate toward to crypt base6. A complex interplay of signaling factors from a variety of cell types, such as Paneth cells, mesenchymal cells, and CD4+ T cells is required to determine epithelial cell fate upon differentiation from ISCs8,9,10.
Although mature ISCs express Lgr5, the gene expression pattern of ISCs in the fetal intestine had not been analyzed until recently11. Single-cell RNA sequencing of human fetal intestinal tissue provided new insight into the identity of epithelial cell precursors in utero11. At 10 weeks gestation, lgr5 expression is found throughout the intestine, not specifically in intestinal crypts, and enterocytes differentiate instead from a “stem-cell like” population of progenitor cells high in vitronectin, transferrin, and gata4 expression and low in lgr5 expression11. Lgr5 expression becomes increasingly localized in the crypt at 12 weeks, and Lgr5+ progenitors increase in frequency from 8 weeks to 19+ weeks gestation11. Interestingly, Lgr5+ cells compose as much 18–22% of epithelial cells at 19+ weeks gestation, which is significantly higher than the 3–4% they represent in the adult colon11. The abundance of ISCs in the first and second trimesters is necessary to provide adequate numbers of precursors to form the epithelial lining of the rapidly developing crypt-villus architecture. Once this structure is achieved, the signaling niches required for the development of each epithelial subtype begin to form.
Extremely preterm infants are delivered during a period of intestinal development characterized by an abundance of ISCs and reduced numbers of mature specialized epithelial cells, which places them at risk for a myriad of complications related to inadequate intestinal epithelial function.
EnterocytesEnterocytes (IECs) are the most abundant epithelial cell in the intestine and serve as the primary barrier for the regulation of transport between the intestinal lumen and the circulation12. Barrier function provided by these IECs is formed by tight junctions, which are protein complexes between epithelial cells13. Tight junctions are initially observed between epithelial cells at approximately 10 weeks gestation14. After delivery, gestational age and receipt of breast milk feeds impact intestinal permeability15,16,17. For example, comparison of intestinal barrier function in neonates based on gestational age and the number of days after delivery indicates that intestinal barrier permeability is increased in preterm neonates compared to term infants (> 37 weeks gestation) during the first 2 days after delivery15. By 3–6 days, intestinal permeability decreases in both term and preterm neonates and is similar between infants across gestational ages15. Receipt of breast milk feeds is associated with reduced intestinal permeability over the first 30 days of life in preterm neonates, with the most benefit derived from a higher percentage of breast milk feeding (>75% of diet), although receiving volumes as low as 25% is likely beneficial during that time frame17. In vitro studies using human intestinal organoids found that human milk increased epithelial cell differentiation and expression of the tight junction protein occludin, which was associated with reduced permeability18. These studies highlight the importance of providing human milk feeds to neonates. In addition to improving intestinal barrier function, human milk provides numerous factors that provide protective immune functions including immunoglobulins, which will be discussed below.
Due to the restriction of movement across the intestinal epithelium imposed by the epithelial monolayer and tight junctions, specialized transporters are required for the passage of larger molecules such as immunoglobulins between the intestinal lumen, lamina propria, and systemic circulation. One such transporter, the neonatal Fc receptor (FcRn), is expressed by the intestinal epithelium and transfers immunoglobulin G (IgG) across the epithelial monolayer in a bidirectional fashion19. This process facilitates immune cell activation by transporting antigen-antibody complexes formed in the intestinal lumen to the lamina propria and dendritic cells20. The importance of FcRn-mediated IgG transport in the intestine of human infants is uncertain given the robust transplacental transfer of maternal IgG into the fetal circulation; however, FcRn-mediated transfer of maternal breast milk-derived IgG from the intestinal lumen is important in protection from enteric pathogens in mice and may be of higher importance in the preterm infant who is born prior to transplacental transfer of IgG that occurs in the 3rd trimester21,22. In addition to FcRn, intestinal epithelial cells express a polymeric immunoglobulin receptor (pIgR), which facilitates secretory IgA (sIgA) and IgM transfer across the intestinal epithelium23. sIgA is the most abundant antibody present in human breast milk and has a vital role in early host defense24. Mice lacking this receptor or who lack exposure to maternal breast milk-derived sIgA have decreased mucosal barrier integrity and an altered microbiome as adults23,25.
The healthy developing intestinal epithelium, although immature, forms a functional barrier. There are also mechanisms in place for the transport of immune mediators and nutritional factors between the lamina propria and intestinal lumen. Achieving a balance between these opposing roles is critical for intestinal homeostasis, and one of the first challenges faced by the intestinal epithelial is provided by the developing microbiome.
Microbiome in IEC developmentThe intestinal microbiome develops rapidly upon delivery, and these bacteria can directly impact the development of the intestinal epithelial monolayer. Bacteria abundant in the intestine of breastfeeding term neonates, such as Bifidobacterium spp., metabolize human milk oligosaccharides in breast milk and produce biologically active compounds such as short chain fatty acids (SCFAs)26,27. SCFAs can act directly on intestinal epithelial cells and immune cells28. When infants are born prematurely, their microbiome is instead predominated by potentially pathogenic bacteria such as Staphylococcus, Klebsiella, Escherichia, or Enterococcus spp29. The presence of these microbes in stool samples has been associated with the development of bacteremia and sepsis in preterm neonates30. Given the negative impacts of microbial dysbiosis on neonatal health, there are ongoing discussions regarding whether routine administration of probiotics to infants in the NICU should occur in an effort to modify the microbiome31.
Preterm and critically ill neonates are frequently exposed to antibiotics in the NICU due to their lability and risk of death from infection32. These antibiotics directly impact the composition of the intestinal microbiome29,30. In addition, mechanistic studies in mice have demonstrated how antibiotic administration impacts intestinal development. For example, treatment of neonatal mice with the commonly used antibiotics ampicillin and gentamicin for 10 days resulted in significantly shorter villus length and crypt depth relative to untreated controls, as well as increased intestinal permeability and inflammation33. These findings were associated with decreased intestinal epithelial cell proliferation within the crypts as well as lower numbers of goblet and Paneth cells33. In another study examining the impact of the microbiome on intestinal development, germ-free mice were colonized with the microbiome of preterm human infants born at 27 weeks gestation who had weight gain of either < 10 g/kg/day (inadequate growth) or >10 g/kg/day (normal growth). The microbiome from infants with normal growth resulted in the development of a significantly longer small intestine as well as longer villi and deeper crypts in recipient mice34. This improved intestinal growth was associated with increased numbers of proliferating stem cells and transit amplifying cells as well as goblet cells, and Paneth cells34. Mice that received the microbiome from infants with poor weight gain were found to have increased intestinal and systemic proinflammatory gene expression34. Improving growth and reducing inflammation are two additional reasons to strive towards promoting a healthy microbiome in neonates by providing human milk feeds and avoiding unnecessary antibiotic administration.
Activation of intestinal epithelial cellsBacteria in the intestinal lumen can induce inflammation by stimulating innate immune receptors such as Toll-like receptors (TLRs), which are located on intestinal epithelial cells and immune cells. TLRs are a class of innate immune receptors that recognize components of bacteria and viruses35,36. Stimulation of TLRs activates an inflammatory cascade that can lead to the elimination of an invading pathogen and/or tissue damage35,36. Studies utilizing reporter mice that express fluorescent proteins in conjunction with TLRs found similar levels of TLR2, 4, 7, and 9 in both neonatal and adult small intestines and colons37. Studies in fetal mice detected higher expression of TLR4, the receptor for bacterial lipopolysaccharide (LPS), and lower levels of TLR9, a receptor for bacterial DNA, in the intestine of mice in utero relative to the expression at the time of delivery38. This expression pattern has been linked to the pathogenesis of NEC, which will be discussed below in more detail38. TLR5, which recognizes bacterial flagellin, is expressed throughout the intestinal epithelium in neonatal mice37. This level of expression decreases until weaning/adulthood, when TLR5 is primarily localized to Paneth cells37. Increased TLR5 signaling in neonatal mice has been associated with the early establishment of the microbiome and controlling flagellated intestinal bacteria39. Expression of TLR3, the receptor for double stranded RNA, is also developmentally regulated in mice. PCR analysis of gene expression on intestinal epithelial cells found that TLR3 expression gradually increased from P7 to P2837. Studies in mice indicate that increased susceptibility of neonates to infection with Rotavirus, a cause of severe diarrhea in infants, may be in part due to the reduced TLR3 expression on IECs of neonatal mice40. Although more mechanistic studies are needed, it is clear that changes in TLR expression over the course of intestinal development are a critical mechanism underlying age-based differences in susceptibility to inflammatory and infectious GI diseases.
The innate immune defense mechanisms of the small intestine extend beyond TLR signaling in the intestinal epithelium. Two important epithelial cell subtypes involved in innate immunity include Paneth cells and goblet cells. These cells will be discussed in detail below.
Paneth cellsPaneth cells produce antimicrobial peptides (AMPs), a diverse family of molecules that serve as an initial line of defense against potentially harmful pathogens in the gut41,42. Murine experiments indicate that Paneth cells also impact Lgr5+ ISC development via growth factor production43.
Paneth cell numbers increase in the human intestine with advancing gestational age (Fig. 1)44,45. In human intestinal biopsy samples, Paneth cells are observed in very low numbers at 17–23 weeks gestation but increase dramatically at term44. Similarly, in the murine small intestine, Paneth cell numbers increase linearly from P1 to P28, with low numbers found in the first 7 days after birth44,46. Paneth cell-produced AMPs also have a gestational age-dependent expression pattern44,45,47. For example, the expression of the AMPs regenerating islet-derived protein 3, lysozyme-1, and alpha defensin increase with increasing Paneth cell numbers in mice and humans44. When infants are delivered preterm, their Paneth cell and AMP levels are reduced compared to term infants, which likely increases their risk for sepsis resulting from bacterial translocation from the gut. In contrast to the other AMPs, the expression pattern of the antimicrobial peptide cathelin-related antimicrobial peptide (CRAMP) is highest shortly after birth and subsequently decreases with age. IEC expression of CRAMP is detectable in the intestine of neonatal mice until P14 and then becomes undetectable at P21 and P2847. This may be clinically significantly as neonatal CRAMP knockout mice exhibit decreased control of oral Listeria monocytogenes infection47. In addition, CRAMP has dose-dependent antimicrobial activity against a variety of commensal bacteria as well as potential neonatal pathogens47. These findings have led to the hypothesis that CRAMP may have an important role in the initial establishment of the neonatal intestinal microbiome47.
Goblet cellsGoblet cells produce mucus, secrete AMPs, and deliver antigens to intestinal immune cells via goblet cell-associated antigen passages (GAPs)48. In utero, goblet cell numbers are minimal at 8–10 weeks gestation but increase between 12 weeks to 19+ weeks11. Mucin 2 (muc2) expressing goblet cell numbers remain stable between 17 weeks and term gestation44. A similar pattern is observed in the murine intestine from P1 to P2844. Disruption of goblet cell function and mucus production can lead to reduced protection of IECs from intraluminal gut bacteria, which can subsequently lead to increased inflammation33. The mucus produced by goblet cells is an important component of the intestine’s innate immune defenses and barrier function. In contrast, GAPs have been associated with the development of late onset sepsis from Escherichia coli in a neonatal model49. Epidermal growth factor (EGF) from breast milk led to reduced GAP formation and decreased E. coli translocation from the intestine49. GAPs are important in providing antigens to antigen-presenting cells, which leads to immune activation. In neonates, there is a delicate balance between providing immune education and preventing dissemination of potentially harmful bacteria. Bacterial species that evade mucosal defense mechanisms, such as the invasive E. coli described above, are a particularly important threat to neonatal health. Another intestinal cell type involved in providing antigens from the intestinal lumen to underlying immune cells is Microfold (M) cells.
M cellsM cells are a specialized type of epithelial cells found in close association with gut-associated lymphoid tissue50. These cells serve as a route of transfer of microbial products from the intestinal lumen to antigen-presenting cells, which then modulate the immune response50. In mice, M cell numbers are minimal in the first few days after birth, with increasing numbers noted after P851. In human fetal tissue, M cells have been identified as early as 17 weeks in the small intestine52.
Functionally, sIgA production in the intestine requires appropriate M cell development due to the role of M cells in intestinal microbial antigen delivery to underlying immune cells53. For example, recently weaned mice with an M cell maturation defect were found to have reduced concentrations of reduced of commensal bacteria-specific IgA and IgA bound bacteria in their stool53,54. The importance of M cells in sIgA production prior to weaning is likely minimized due to the abundance of sIgA provided by human milk55. This is supported by findings of significantly lower levels of intestinal bacteria bound by sIgA in the feces of formula fed preterm human infants relative to those receiving maternal milk56. Thus, sIgA provided by maternal milk likely predominates above M cell mediated mechanisms in early life.
Enteroendocrine cellsEnteroendocrine cells are primarily known to produce hormones in the gut in response to nutritional signals, which subsequently aid in digestion and metabolism57. Quantification of enteroendocrine cells by staining tissue sections for α-chromogranin over the course of fetal development found similar percentages in the small intestine from 17 weeks gestation to term44. Mice have a similar developmental pattern with a constant number between P1 and P2844. Analysis of serum levels of gut hormones found that the impact of gestational age at delivery and the number of days since birth on hormone levels is variable
留言 (0)