
記住我

The novel coronavirus disease 2019 (COVID-19), caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), has become the most severe health crisis worldwide in recent history.1 According to the WHO COVID-19 dashboard,2 as of November 20, 2021, 223 countries and regions reported more than 255 million confirmed cases, and more than 5.1 million patients died. And currently, the cases and deaths have been increasing continuously at the rate of over 0.6 million new cases and 6,000 deaths confirmed every day.2
Fortunately, through painstaking efforts and tremendous sacrifices on prevention and control of the COVID-19 spread, China succeeded in turning the situation around.3 On March 6, 2020, the daily increase in the number of domestic cases on the Chinese mainland dropped below 100 and fell further to a single digit on March 11. On March 18, 2020, no new domestic cases were confirmed on the Chinese mainland for the first time since the beginning of the pandemic, and Wuhan lifted its 76-day outbound traffic restrictions on April 8. Since then, China's COVID-19 control has shifted its focus to preventing inbound cases and stemming domestic resurgence on an ongoing basis.
In response to the evolving COVID-19 dynamics overseas, the Chinese government adopted a series of effective measures. SARS-CoV-2 nucleic acid testing, recommended as a standard confirmation protocol for SARS-CoV-2 infection by WHO,4 plays a vital role in preventing the virus from entering China and stemming domestic case clusters. On April 10, 2020, through its joint prevention and control mechanism, the State Council informed that the PCR laboratory capacity of nucleic acid testing in medical institutions should be increased to ensure all those in need could be tested in a timely manner.5 Subsequently, on April 18, the State Council explained the relevant requirements on registration and construction of testing laboratories, training and admittance for laboratory technicians, and quality control and bio-safety in laboratories.6 Moreover, on April 30, the State Council emphasized that the capacity of nucleic acid testing in tertiary and county hospitals must be enhanced rapidly to ensure that the outpatients with fever, those highly suspected of COVID-19, and the admitted patients and their companions can be tested immediately.7
To expand population coverage of SARS-CoV-2 nucleic acid testing and to ensure that persons returning to work and workers in key organizations could receive timely and periodic testing, testing capacity in secondary hospitals was required to be also strengthened and qualified social testing institutions were encouraged to provide testing services.8 Furthermore, in June 2020, the State Council issued three bulletins, defining requirements on the quality and efficiency of SARS-CoV-2 nucleic acid testing, and urging continual technician training for nucleic acid testing to build a testing capacity reserve.9-11 From July to December, the technical handbook for SARS-CoV-2 nucleic acid testing in medical institutions,12, 13 the guidelines on mixed-sample testing,14 and the norms on 10-in-1 sampling15 were sequentially released to ensure nucleic acid testing rightful operation and good quality.
The Affiliated Hospital of Qingdao University, as a provincially regulated tertiary grade-A hospital, has conducted SARS-CoV-2 nucleic acid testing for outpatients with fever, those highly suspected of COVID-19, and admitted patients and their companions since April 30, 2020. To meet the demand for massive nucleic acid testing, our hospital constructed a specialized PCR laboratory with an area of 297 m2 and appointed 10 fixed technicians to engage in nucleic acid testing (extraction and amplification). From June 22, 2020, all workers in our hospital began to be tested for nucleic acid screening (10-in-1 sampling for testing) once every 2 weeks. Our hospital also started to provide testing services for social workers on September 30, 2020. To further prevent potential nosocomial transmission of SARS-CoV-2, since November 16, 2020, the inpatients and their companions were required several times of nucleic acid testing, separately after admission, before discharge, and during hospitalization. In addition, environmental samples in key locations in our hospital were also sent to the PCR laboratory for nucleic acid testing to monitor the disinfection effect in air and on surfaces. As a result, as of mid-November 2020, the daily number of single-tube samples for nucleic acid testing reached above 4,000.
With the increase in sample number, the ten technicians continually improved their workflow, and in early December 2020, a rapid and highly effective testing approach was established, allowing five technicians to complete 6,500 single-tube tests in one day with a high level of quality. This article describes the testing approach as a means to provide a referable workflow for other testing institutions. We also report our satisfactory quality control results and rightful reporting criterion.
2 MATERIALS AND METHODS 2.1 Sampling and receivingOutpatients with fever, those highly suspected of COVID-19, and admitted patients and their companions were separately guided to the appointed outdoor sampling sheds. The recommended nasopharyngeal swab was sampled.12, 13 The inpatients in common and isolation wards were sampled in situ; the nasopharyngeal swab was also preferred. Companions of the inpatients in common wards were also sampled in situ. According to the stipulation released by our hospital, one patient was allowed to be taken care of by only one companion (no companions for inpatients in the isolation ward). Single testing was applied to all patients, and their companions, i.e., a single sample of each patient or companion was separately tested, and the samples of social workers and environments in key locations. The 10-in-1 testing method was applied to all workers in our hospital, in which ten nasopharyngeal swabs were mixed into one test tube, and sampling was performed in their attached departments.
Disposable virus sampling tubes (inactivating type) were provided by Yongkang Medical Products Co., Ltd. (Shandong, China). Two kinds of tubes were used for single (2 mL of preserving fluid in a 5-mL tube) and 10-in-1 (6 mL of preserving fluid in a 10-mL tube) testing. Guanidine salt and nano-silver were added the preserving fluid to inactivate the virus. For outpatients with fever and those highly suspected of COVID-19, another kind of tube containing a nucleic acid releasing agent in 500 μL of preserving fluid (Jianma Gene Technology Co., Ltd., Shandong, China) was used, and the sample in this kind of tube was directly submitted to nucleic acid amplification (dispensed with nucleic acid extraction).
Our hospital contains five districts (Shinan, Shibei, Laoshan, Xihaian, and Pingdu). The PCR laboratory specifically used for SARS-CoV-2 nucleic acid testing is set in the clinical laboratory department in the Xihaian district. Samples were sampled in the 7:30–12:00 and 13:30–17:00 periods, and received by PCR laboratory in the 8:30–11:00, 12:00–15:30, and 17:00–20:30 periods (the samples of outpatients with fever and those highly suspected of COVID-19 were sampled and tested in the fever clinic in each district at any time in 24 h, not sent to the PCR laboratory). Samples were sealed and temporarily preserved in sampling sites or departments in each district and then centrally transported in batches to the PCR laboratory by the appointed medical services. The receivers scanned all samples into our laboratory information system, numbered each sample, and then passed the consecutively numbered samples, in a group of 96, to the technicians for nucleic acid testing (extraction and amplification).
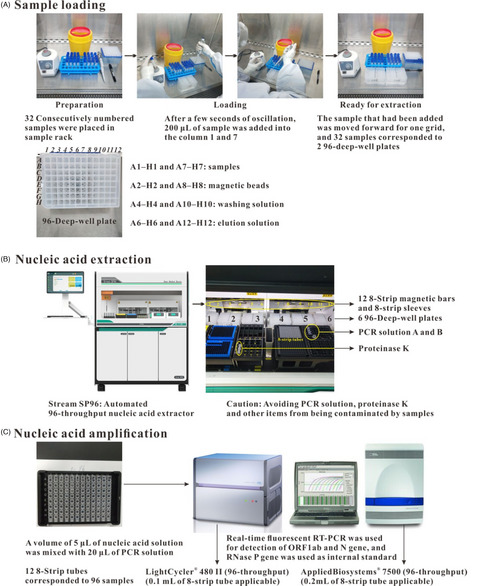
2.2 Extraction and amplificationSARS-CoV-2 nucleic acid testing in the PCR laboratory involves nucleic acid extraction and amplification (Figure 1). The nucleic acid extraction was performed in the sample pretreatment zone. In this zone, there were 3 HFsafe-1200 bio-safety cabinets (Heal Force Bio-Meditech Holdings Limited, Shanghai, China) and 7 automated 96-throughput nucleic acid extractors (Stream SP96, Daan Gene Co., Ltd. of Sun Yat-sen University, Guangdong, China). Matched nucleic acid extraction kits (DA0623, with 96-deep-well plates and 16 extractions per plate) were also used.

SARS-CoV-2 nucleic acid testing procedure in the PCR laboratory
For DA0623, each plate had 12 (1–12) columns and 8 (A–H) rows, and 200 μL of the sample was manually added into columns 1 and 7 in accordance with the sequence of A1-H1 and A7-H7, respectively, in which guanidine salt and proteinase K were used for denaturalizing and disintegrating proteins (Figure 1A). Then, six plates with 96 samples were placed sequentially on the plate board (Figure 1B). When the extractor started, the 8-strip magnetic bars nested in 8-strip sleeves transferred magnetic beads from columns 2 and 8 to columns 1 and 7 for adsorbing the dissociated nucleic acid. Then, the magnetic beads were transferred to columns 4 and 10 to wash sample matrices and then to columns 6 and 12, releasing the purified nucleic acid in RNase-free water. Finally, the magnetic beads were transferred back to the washing solution, and a high-quality nucleic acid solution was obtained, of which 5 μL was mixed with the PCR solution (20 μL, i.e., 17 μL of solution A + 3 μL of solution B) in 8-strip tubes for nucleic acid amplification (Figure 1C).
The nucleic acid amplification was performed in the amplification and analysis zone. This zone was equipped with 10 rapid 96-throughput and real-time fluorescent PCR amplification instruments (5 LightCycler® 480 II, 0.1 mL of 8-strip tube applicable, Roche Diagnostics GmbH, Mannheim, Germany; 5 AppliedBiosystems® 7500, 0.2 mL of 8-strip tube applicable, Thermo Fisher Scientific Inc., Waltham, MA, USA). The rapid nucleic acid detection kit (i.e., PCR solution, DA0992,16 Daan Gene Co., Ltd.) contains rapid catalyzing enzymes, specific primers, fluorescent probes and nucleotides in a suitable buffer, and the real-time fluorescent reverse-transcription PCR (RT-PCR) method was used. The detection targets were the open reading frame 1ab (ORF1ab) and nucleocapsid protein (N) genes of the SARS-CoV-2 genome. The amplification procedure for the ORF1ab and N gene is presented in Table 1. The RNase P gene was used as an internal standard for supervising virus sampling, sample loading, nucleic acid extraction, and amplification.
TABLE 1. Amplification procedure for target genes (ORF1ab and N genes) of SARS-CoV-2 and the RNase P gene that was used as internal standard Amplification procedure Stage Cycles Target temperature (°C) Running time (s) 1 1 50 120 2 1 95 120 3 10 95 5 60 10 (LightCycler® 480 II); 35 (AppliedBiosystems® 7500) 4 32 95 5 60 (Data acquisition) 10 (LightCycler® 480 II); 35 (AppliedBiosystems® 7500) Note Cited from the instruction of DA0992.16 2.3 Protection, disinfection, and quality controlIndividual protection was performed according to the guidelines for preventing and controlling SARS-CoV-2 infections in medical institutions17, 18 and the guidelines on bio-safety in SARS-CoV-2 laboratories.19 The sampling operators, sample receivers, and laboratory technicians who worked in the sample pretreatment zone followed senior secondary protection criteria, which includes an inner garment, surgical gown, medical protective mask and suit, disposable cap, eyes protector, latex gloves (duplex), and waterproof boot cover. The sample transporters and laboratory technicians who worked in the reagent preparation zone and nucleic acid amplification and analysis zone followed primary secondary protection criteria, including an inner garment or labor suit, surgical gown, medical protective mask, disposable cap, latex gloves, and shoe cover.
In the PCR laboratory, daily disinfection was performed according to the technical handbook for SARS-CoV-2 nucleic acid testing in medical institutions.12, 13 Briefly, at the end of daily testing, 2,000 mg/L (w/v) of chlorine disinfectant or 75% (v/v) of alcohol in water was used for disinfecting the worktable surface, laboratory ground, instruments, bio-safety cabinets, micropipettors, and the movable sample depository vehicles nearby each cabinet. If a sample spilled and polluted the operating bench, 5,500 mg/L (w/v) of chlorine disinfectant was used immediately. In addition, all medical waste derived from the PCR laboratory was transferred to a temporary storeroom and then centrally cleared out and destroyed by the appointed medical dustmen. The last technician to leave the PCR laboratory, after completing daily testing, turned on all ultraviolet lamps to disinfect the laboratory air for at least 2 h.
Internal quality control (IQC) in the PCR laboratory was performed every day when the first group of samples was treated. Two positive controls, provided by Bioyuan Biotech Co., Ltd. (Shanghai, China), coupled with three negative controls (physiological saline), were randomly placed among samples for evaluating the effectiveness of nucleic acid testing. The concentration levels of the two positive controls were approximately 500 and 1,000 copies/mL of SARS-CoV-2 nucleic acid. To prevent residual nucleic acid from polluting the PCR laboratory, the nucleic acid scavenging reagent was used for cleaning the air, worktable surface, equipment, and other items in the laboratory once a week. In addition, we also regularly participated in external quality assessment (EQA) organized by the National and Provincial Center for Clinical Laboratories, and a qualified certificate was granted to us in each EQA activity.
3 RESULTS 3.1 Testing approachFrom late November 2020 to early February 2021, the daily number of single-tube samples for single testing was maintained at a high level over 4,000, and although the daily amount decreased in April, it remained around 3,500 (Figure 2A). The slight decrease in the daily sample number was attributed to a decrease in the admitted patients as outdoor temperatures rose and testing capacity in other institutions increased. In addition, when the biweekly nucleic acid screening (10-in-1 testing, Figure 2C) for workers in our hospital was conducted, the total number of single-tube samples reached 6,500 in a single day. To cope with the large daily sample number and accommodate the different numbers of received samples in the three receiving time periods (Figure 2B), the ten technicians developed a rapid and highly effective testing approach.

The daily number of single-tube samples received by the PCR laboratory from late November 2020 to late April 2021
(a) The ten technicians divided themselves into two groups, with five technicians in each group. One group of five technicians worked for 3 days, and another five technicians worked for the next 3 days (the first five technicians rested during these 3 days); this scheme was then reiterated. (b) In each group, labor divisions were equally assigned to five technicians. As shown in Table 2, four labor divisions corresponded to five labor combinations. The labor combinations were reiterated in accordance with the sequence of 1–2–3, 4–5–1, 2–3–4, 5–1–2, and 3–4–5. (c) A flexible daily profile of technician assignment and working hour arrangement was designed, as shown in Table 2, which meant that the technicians on duty increased from 3 to 5, and the 3 working hours covered the three receiving time periods. On the working days, times out of work were used for providing rest for technicians. (d) To raise working efficiency, a group of 96 samples was simultaneously loaded by two or three technicians, which was beneficial for reducing waiting time to extract nucleic acid in the 96 samples and performing extraction in the sequence of numbered samples. (e) As shown in Table 3, nucleic acid extraction was carried out in the sequence of Stream SP96 1–7. Based on the time consumption difference in SARS-CoV-2 nucleic acid amplification, the two kinds of PCR amplification instruments were used in a reasonable arrangement as shown in Table 3.
TABLE 2. SARS-CoV-2 nucleic acid testing approach with four labor divisions and five labor combinations Laboratory Technicians Labor combinations Combination 1 Combination 2 Combination 3 Combination 4 Combination 5 Technician 1 I/III II-post II-post II-pre−2 II-pre−1 Technician 2 II-pre−1 I/III II-post II-post II-pre−2 Technician 3 II-pre−2 II-pre−1 I/III II-post II-post Technician 4 II-post II-pre−2 II-pre−1 I/III II-post Technician 5 II-post II-post II-pre−2 II-pre−1 I/III Labor Divisions Working hours and labor duties Hour Duty Hour Duty Hour Duty I/III 9:00–11:30 Reagents, consumables, and protective items preparation 14:00–17:00 Nucleic acid amplification, analysis, and auditing reports 19:00–auditing over Nucleic acid amplification, analysis, and auditing reports II-pre−19:00–10:30
10:30–12:00
Sample loading and nucleic acid extraction
Nucleic acid amplification, analysis, and auditing reports
17:30–loading over Sample loading and nucleic acid extraction II-pre−2 9:00–12:00 Sample loading and nucleic acid extraction 14:00–16:30 Sample loading and nucleic acid extraction 18:30–extraction over Nucleic acid extraction II-post 12:30–15:00 Sample loading and nucleic acid extraction 17:30–loading over Sample loading II-post (Described once again) 12:30–15:00 Sample loading and nucleic acid extraction 17:30–loading over Sample loading Note I: Working in reagent preparation zone (Zone I); II: Working in sample pretreatment zone (Zone II); III: Working in nucleic acid amplification and analysis zone (Zone III). TABLE 3. Time required for each operation and the amplification arrangement Operations Sample loading Nucleic acid extraction Nucleic acid amplification Time required (min) 4.5/32 samples 48/96 samples 44 (LightCycler® 480 II); 73 (AppliedBiosystems® 7500) Extractors DA1 DA2 DA3 DA4 DA5 DA6 DA7 8-Strip tubes (mL) (for amplification) 0.1 0.1 0.1 0.1 0.2 0.2 0.2 0.2 0.2 0.1 0.1 0.1 0.1 0.1 0.2 0.2 0.1 0.1 0.1 0.1 0.1 0.2 0.2 0.1 0.1 0.1 0.1 0.1 0.2… Note DA1–7: Stream SP96 1–7; 0.1 mL: Applied to LightCycler® 480 II; 0.2 mL: Applied to AppliedBiosystems® 7500.Due to the rapid and highly effective approach, all testing results were reported in 2.5–3 h since the samples were received by the PCR laboratory, which was compliant with the requirements regarding the reporting time limit in the technical handbook for SARS-CoV-2 nucleic acid testing.12, 13 In addition, in this testing approach, technician composition and labor division were both flexible, which meant that some of the ten technicians could withdraw from the PCR laboratory if the sample amount declined abruptly (e.g., the daily sample number for single testing decreased from 3,500-plus to fewer than 2,000 in early May 2021 due to policy changes on COVID-19 prevention in our hospital) and then the labor divisions would be redefined and recombined.
3.2 Testing performance validationThe RNase P gene was used as an internal standard for supervising the entire operating procedure for each sample, including virus sampling, sample loading, nucleic acid extraction, and amplification. Therefore, all testing results were reported with amplification of the RNase P gene as a prerequisite. Furthermore, the daily IQC required that the two positive controls with low concentrations (approximate 500 and 1,000 copies/mL) of SARS-CoV-2 nucleic acid were visibly amplified, and the three negative controls had no amplification (Figure 3).

Amplification curves of ORF1ab and N genes using two kinds of PCR amplification instruments
The physiological-saline-diluted positive control with four concentration levels (approximately 25, 50, 100, 200 copies/mL) was used to investigate the testing procedure's analytical sensitivity from sample loading to nucleic acid amplification. The four concentrations of the ORF1ab and N genes all had distinct amplification (Figure 3), which confirmed the effectiveness and sensitivity of the used reagents and the procedure's operations, with a detection limit (<25 copies/mL) similar to or even lower than most reports on coronavirus nucleic acid testing.20, 21
Interestingly, by comparing the amplification curves (Figure 3) of the ORF1ab gene with those of the N gene at the same concentration level, we found that the selected amplified fragment by DA099216 in the N gene sequence had a higher amplification efficiency and a lower cycle threshold (Ct) value, which might be attributed to a higher AT content in this selected fragment. In addition, although the two kinds of PCR amplification instruments were both satisfactory for detecting a low concentration of the two target genes, compared with AppliedBiosystems® 7500, LightCycler® 480 II exhibited higher detection sensitivity (Figure 3), indicating its lower detection limit.
3.3 Testing result reportingIn a daily testing regimen, the positive results should meet the requirements that the two target genes both have an obvious amplification and the Ct values are both ≤30; the negative results correspond to no amplification of the two targets. If only one target gene was amplified, a timely response for resampling and retesting was initiated, and if the retesting result remained the same, a positive result could be reported; a negative report was given if amplification did not happen.
Fortunately, since our hospital started SARS-CoV-2 nucleic acid testing for patients and social workers, there have been no positive reports except for the admitted COVID-19 patients (confirmed in other testing institutions, e.g.,22) in our isolation ward. Nevertheless, a coping strategy was drawn for the positive cases initially reported in our hospital, which was continually updated referring to the protocol on COVID-19 prevention and control (updated to Edition 823). The coping strategy includes a timely network record in the national disease report system as well as an immediate transfer to the appointed medical institutions for isolation and treatment, which should be completed in 2 h.
4 DISCUSSIONSince mid-March 2020, China has entered the post-epidemic phase, and SARS-CoV-2 nucleic acid testing is being conducted continuously in the domestic population and for overseas people coming into China. Nucleic acid testing plays the key role for timely confirmation of new infections, identifying positive close contacts, and eventually preventing viral transmission. Throughout the several local outbreaks of COVID-19 on the Chinese mainland from June 2020 to May 2021 (including the reemergent epidemic in Beijing Xinfadi wholesales market caused by an imported source of infection,24 the cold-chain transmission in Dlian Ganjingzi District derived from virus-contaminated packaging of imported frozen seafood,25 and the case cluster in Guangzhou Liwan District infected by the delta variant strain (B.1.617.2)26), when the first positive case was checked out, large-scale and high-frequency nucleic acid screening was conducted immediately. Therefore, for a PCR laboratory with a fixed configuration (area and equipment), the number of technicians, the labor divisions, and the daily working profile are the critical factors for rapidly and highly effectively completing the massive nucleic acid testing.
In this article, an approach for SARS-CoV-2 nucleic acid daily testing in our PCR laboratory was reported. This testing approach was developed based on the laboratory configuration (297 m2 equipped with bio-safety cabinets, nucleic acid extractors, and PCR amplification instruments) and the sample distribution in different receiving time periods (Figure 2B). The number of nucleic acid extractors and PCR amplification instruments corresponded to that of bio-safety cabinets, i.e., if the number of the latter changed, the former would change accordingly. Based on the time required for sample loading, nucleic acid extraction, and amplification (Table 3), a reasonable equipment matching was three cabinets for seven extractors and ten PCR instruments. The five technicians could complete nucleic acid daily testing with a high level of quality, with three of them loading sample and the other two operating extractors and PCR instruments (Figure 1). Due to nearly half of the daily samples being sent to the PCR laboratory in the 17:00–20:30 period (Figure 2B), only in this time period, all the five technicians worked in the laboratory. In the other two time periods, only three or four technicians were assigned (Table 2). Finally, to provide enough resting time for the five technicians after laborious work, another group of five technicians took over testing work, and the first five technicians rested for several days. After soliciting individual opinions, an interval of 3 days was thought to be beneficial to refresh the workers’ energy. Although the laboratory configurations in other testing institutions are different from each other, the testing approach presented in this article can provide a referable workflow and be adapted for a suitable number of technicians and a reasonable daily working profile.
Depending on the developed testing approach, a short turnaround time of 2.5–3 h was achieved since samples were received by the PCR laboratory, which was much lower than the official requirement (6–24 h).12, 13 The satisfactory results of daily quality control and high sensitivity of the detection method (Figure 3) proved that the testing approach was reliable and effective. Furthermore, the testing results were reported referring to the latest national reporting criterion,23 which ensured that the testing reporting was lawful and rightful, embodying the responsibility of medical workers for the tested population. In addition, individual protection and daily disinfection were performed according to the national operation standard,17-19 which protected the personal safety of the technicians and prevented residual nucleic acid from polluting the laboratory. In summary, these strategies ensured that our testing approach ran confidently and successfully, and contributed a positive feedforward to national COVID-19 prevention and control.
Up to now, there has been an article to report their workflow in the PCR laboratory for large-scale population screening for SARS-CoV-2 infection.27 In the article, the authors described their laboratory configuration and technicians’ labor divisions (Table 4). (a) Coinciding with our opinions, they also identified that the number of the bio-safety cabinets in sample pretreatment zone determined the numbers of the nucleic acid extractors, the PCR amplification instruments, and the laboratory technicians assigned. Based on numerous practices, we recommended that a reasonable ratio should be confined within a range of 1: 2–3: 3–4: 2, so we considered that an excessive assignment of PCR amplification instruments and laboratory technicians appeared in the reference. (b) Similar to our labor divisions, they also defined labor duties for all technicians working in the PCR laboratory, which included reagent preparation, sample loading and distribution, and nucleic acid extraction and amplification. Due to our more definite labor divisions and combinations as well as much more resting time provided for technicians (Tables 2 and 4), a much higher testing capacity (1,300 tubes/technician/15 h vs. 745 tubes/technician/24 h, Table 4) could be achieved in our approach. (c) Therefore, these lines of evidence demonstrated that our testing approach was rapid and highly effective for large-scale population screening. Expectantly, referring to the two reported testing approaches, the State Council could further optimize the guidelines on conducting large-scale testing of SARS-CoV-2 nucleic acid in population.28, 29
TABLE 4. Comparisons of the two approaches for SARS-CoV-2 nucleic acid testing provided by our article and the Reference Testing approach Our article Reference 27 Laboratory configuration Area 297 m2 -a Bio-safety cabinets 3 7 Nucleic acid extractors 7 15 PCR amplification instruments 10 30 Laboratory technicians Total 10 (5 technicians/group) 54 (18 technicians/group) Zone I 1b 1 Zone II 4 13 Zone III 1b 2 Mobile 0 2 Working profile Daily testing of large-amount samples Short-term and large-scale population screening Working hours/Technicians assigned Morning shift 9:00–12:00/3 (in the same group) 6:00–15:00/18 (the first group) Afternoon shift
留言 (0)