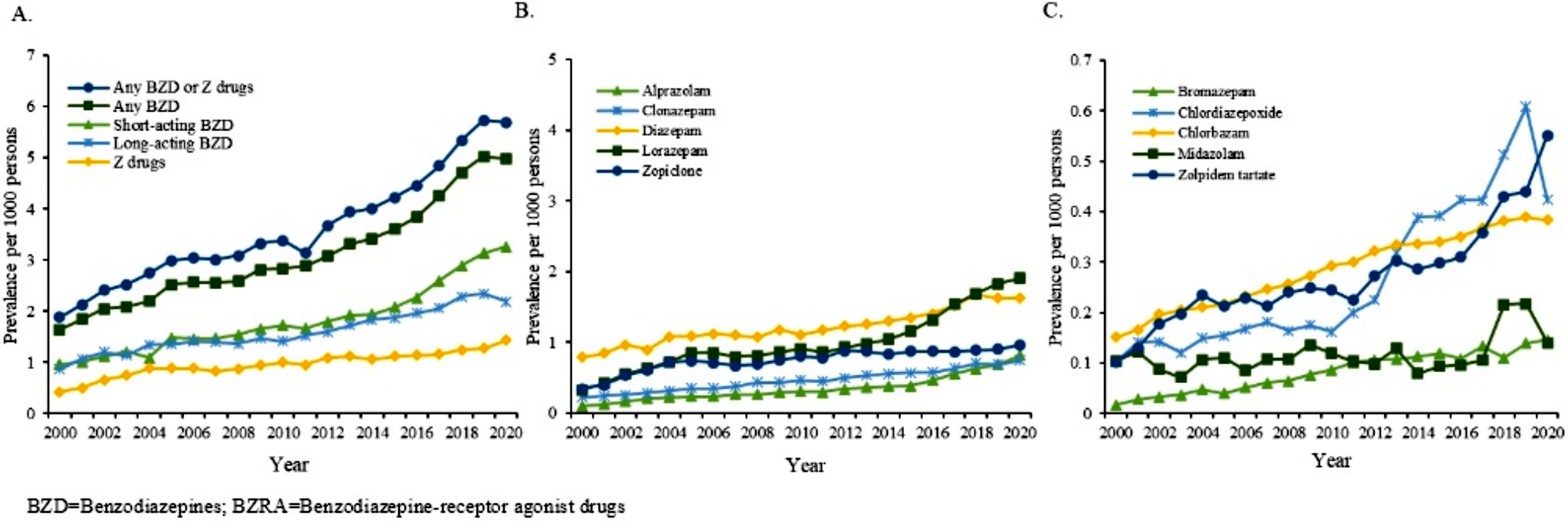
To our knowledge, this is the first population-based study examining the real-world temporal utilization patterns and annual prescription rates of BZRAs, encompassing different BZRA subtypes and individual BZRA medications, among children, adolescents, and young adults in Asia. Three major findings emerged: First, the overall annual prevalence of BZRA use increased, with the highest prescription prevalence observed in the 18–24 age-group, marking a more pronounced increase compared to younger age-groups.; Second, the use of all BZRA subtypes and individual BZRA medications consistently increased over time, except that Z-drug prescription prevalence among children declined; Third, among individual BZRA medications, lorazepam and diazepam were most frequently-prescribed, while alprazolam displayed the steepest increase in prescription.
Our finding highlighted a threefold increase in BZRA utilization. Limited research on BZRA prescribing in younger populations and methodological variations between studies preclude direct cross-study comparison with our findings. Nonetheless, the prescription prevalence of BZRA in our study largely corroborated the results of Taiwan [17], though lower than those reported in Western countries [1, 8, 12, 13, 16]. Likewise, our findings of increasing trends of BZRA prescriptions over time were generally consistent with data in many European countries [1, 13], but contrasted with the declining trend observed in Ireland [12], Australia [16], and Taiwan [17], and the stable trends in Iceland [30] and Denmark [8]. The growth of BZRA utilization adds to the concerns about BZRA use in young persons [5], including the depressant effect on central nervous system, potential drug misuse [14], and cognitive deficits [6]. It is worth noting that, over the study period, the number of children and adolescents with mental-disorder diagnoses in HK increased significantly. For instance, the caseload of child and adolescent psychiatric clinics in HK markedly increased from 18,974 cases to 36,400 cases over the past decade [31], with anxiety and depression being the leading diagnoses. The off-label BZRA prescription (i.e., outside of approved indication or age category) may have become increasingly common locally and globally in recent years. As the risk-benefit ratio of BZRA use has not yet been fully clarified for children and adolescents, it is important to guide clinicians for cautious use of BZRAs in their prescribing practices. Close clinical monitoring of the young population receiving BZRAs is warranted until further research establishing their safety and effectiveness in this population.
Young adults had doubled the prescription prevalence of adolescents and quadrupled those of children over the study period, along with a slightly more pronounced increase. This trend might indicate enhanced recognition and diagnosis of anxiety disorders among young adults, who are clinically eligible for BZRA prescription treating acute anxiety [3, 4]. However, research on the effectiveness and long-term safety of BZRAs in this young population remains insufficient [5]. Additionally, the transitional age from adolescence to young adulthood is at heightened risk of drug misuse. Further efforts are needed to ensure judicious and evidence-based prescribing of BZRAs in this transitional age group [14].
We found that all BZRA subtypes and individual BZRA medications consistently increased over time, aligning with previous studies [13, 17]. Notably, Z-drug use exhibited an overall increasing trend over time, but with a decline in use in children. This is, however, generally consistent with findings of studies conducted in the Western countries indicating more controlled usage patterns of Z-drugs in children and adolescents [11, 16]. The decrease in Z-drug use in children might partly be attributable to an introduction of melatonin for insomnia in children in recent years [32]. The lack of approval and limited treatment guidelines for pediatric use of Z-drugs also restrict their utilization in children [33]. The familiarity of clinical use for and availability of benzodiazepines, along with a better understanding of their pharmacokinetics in children, may contribute to clinicians’ preference in using benzodiazepines to Z-drugs in pediatric cases [34]. Furthermore, a wider range of treatment indications beyond insomnia, including anxiety and epilepsy, for benzodiazepines in children, might account for their higher overall utilization rates relative to Z-drugs, which are primarily indicated for insomnia [35]. Regarding individual BZRA medications, diazepam was among the most commonly-prescribed, consistent with Western studies [12, 16]. It was explained by the clinical guidelines that diazepam has FDA-approved dosing for generalized anxiety disorder and neurological conditions in children and adolescents [3]. Consistent with prior research [10, 17], lorazepam, a short-acting BZRA, was prescribed as frequently as diazepam in our sample. For adults, but not in children and adolescents, lorazepam is indicated for generalized anxiety disorder, while depression and anxiety represented the most commonly-assigned diagnosis for BZRA-users in our sample. Moreover, our study data covered participants from both inpatient and outpatient settings, including specialised centres where lorazepam is commonly administered for acute conditions. Alprazolam demonstrated the sharpest increase in utilization, possibly due to recent findings suggesting its effectiveness in reducing anxiety in younger age groups [15].
Owing to the limited existing data, further research is warranted to get insight into the mechanisms as well as the risk and protective factors that shape the current prescribing patterns. Our findings underscore the necessity to develop strategies to avoid potentially harmful prescribing practices of BZRAs. Effective interventions should involve prescribing clinicians, including but not limited to primary and specialised care in paediatrics, internal medicine, and psychiatry, focusing on education, feedback, and peer support [5]. International guidelines recommend prioritizing non-pharmacological treatment for depression, anxiety, and insomnia in young persons [3, 4]. Research should explore the integration of BZRA with various modalities of psychotherapy to facilitate development of effective interventions and psychiatric service delivery for this age-groups. Moreover, more well-designed clinical studies are warranted to investigate the safety and efficacy of these BZRA for young persons.
This study has several limitations. First, our data did not contain information about the prescribing duration, precluding us from further evaluating the utilization patterns of short-term versus long-term BZRA use. Second, similar to other pharmaco-epidemiological studies, patients’ adherence to prescribed BZRAs could not be assessed, hence actual drug use of our study population may be overestimated. Third, although we obtained data on patients’ recorded diagnoses (which, albeit is limited by a proportion of missing data), we were not able to ascertain the precise indication for initiating BZRA treatment on an individual basis, thereby precluding us from examining the prevalence of off-label BZRA use. Fourth, we did not have data regarding the BZRA prescribing specialties, therefore the potential differential relationships between prescribing specialities and specific age categories of the study population could not be explored. Fifth, data of other psychotropic medications was not available. Hence, we were not able to investigate the patterns and extent of polypharmacy with different psychotropics in our sample. Sixth, as our dataset only obtained prescription data till 2020, the current study was not able to cover a more extensive period of the COVID-19 pandemic and therefore precluded us from comprehensively assessing the changes in BZRA utilization patterns across the pandemic era.
In conclusion, this first population-based study on the BZRA prescribing patterns in Asia adds to the growing concerns about BZRA use among young populations. It is critical to improve prescribing practices through close monitoring of BZRA utilisation in young persons, strengthening the adherence to BZRA prescribing guidelines among psychiatrists, primary care practitioners, and other non-psychiatric specialists, as well as improving communications between non-specialised care and psychiatric services in the management of anxiety and depression in children and youths.




留言 (0)