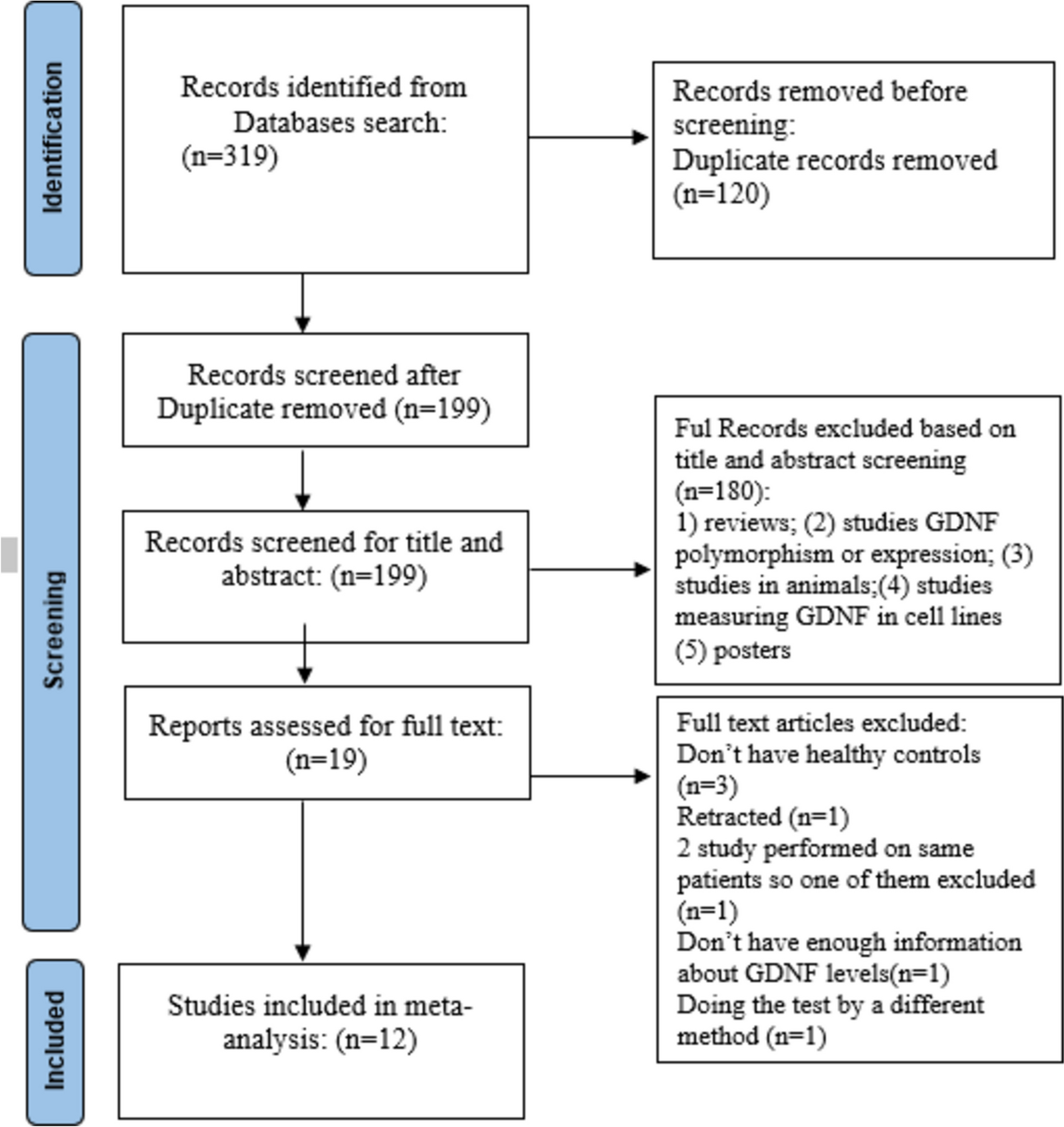
This meta-analysis, which includes 12 studies with over 1,500 participants, examined the role of GDNF in SCZ. Previous research has established the role of GDNF in various mental disorders, including mood disorders [19, 31], anxiety [20], and bipolar disorder [32]. Our analysis extends these findings to SCZ, confirming an association between lower levels of GDNF and the psychiatric condition. This represents the first comprehensive meta-analysis addressing this subject. The high heterogeneity across studies led us to use a random-effects method for pooled estimates. Since heterogeneity can arise from differences in study populations, interventions, outcomes, or methodologies, we estimated effect sizes across subgroups within studies. Additionally, meta-regression analysis was used to better understand the effects of several moderators on the pooled estimates.
Our findings indicate that patients with SCZ exhibit significantly lower circulating GDNF levels compared to healthy controls. This reduction is particularly pronounced in untreated patients and appears to correlate with the dosage of antipsychotic medication. The majority of evidence supports a negative association between GDNF levels and SCZ, while some studies have reported conflicting results [25,26,27]. These discrepancies may arise from variations in sample size, patient demographics, and the complex functions of neurotrophic factors in psychiatric conditions.
The meta-regression analysis suggests that combined estimates remain unaffected by variations in the average age of case and control groups, indicating that included studies likely employed age-matching techniques to reduce the impact of confounding variables. Notably, our analysis found higher GDNF levels in studies involving European samples, which may reflect differences in genetics, nutrition, and lifestyle among populations[33,34,35].
We did not find a relationship between the age of onset and GDNF levels, a finding supported by several studies [7, 10, 12, 23]. This suggests that while GDNF has protective roles for neurons, it may not directly influence the onset of SCZ. Other unknown factors could contribute to disease onset, warranting further investigation.
Additionally, we identified a significant correlation between GDNF levels and disease duration; specifically, longer disease duration is associated with lower GDNF values. This finding aligns with several studies [7, 10] but contradicts others [23, 26], potentially due to small sample size or methodological differences. Furthermore, our study found that GDNF levels were lower in non-medicated subjects compared to those receiving antipsychotic treatment. This highlights the potential impact of these medications on GDNF levels and suggests that antipsychotics may confer neuroprotective effects beyond symptom management by modulating neurotrophic factors.
The relationship between daily antipsychotic dosage and GDNF levels further corroborates the notion that antipsychotics play a significant role not only in managing psychiatric symptoms but also in promoting neuroprotection through the modulation of neurotrophic factors [7]. Given the observed associations between GDNF levels and cognitive function, there is potential for GDNF to serve as a bioecological marker for both diagnosis and treatment response in SCZ.
As a biomarker, GDNF could provide insights into disease progression and therapeutic efficacy. For instance, lower serum GDNF levels might indicate a more severe illness state or poorer treatment responses [7]. Conversely, increases in GDNF levels following antipsychotic treatment could reflect neuroprotective effects and improvements in cognitive function [27]. Therefore, monitoring GDNF levels could enhance personalized treatment approaches for individuals with SCZ.
A study involving mice with a heterozygous GDNF mutation indicated impaired cognitive performance in water-maze tasks [36], underscoring GDNF's role in cognitive function. Additionally, reductions in psychiatric symptoms during antipsychotic treatment was linked to a gradual increase in GDNF levels [7], proposing that GDNF may play a role in both the etiology and pharmacotherapy of SCZ.
Despite our findings supporting a significant association between GDNF levels and SCZ, the relationship between GDNF levels and specific symptom domains remains complex. Our analysis did not identify a direct correlation with total PANSS scores, consistent with findings from two studies [8, 10]. This suggests that while GDNF may influence certain aspects of SCZ, it does not directly correlate with all symptom dimensions assessed by the PANSS. However, some studies have reported correlations between GDNF levels and negative subscales of PANSS [12, 23], indicating a nuanced relationship influenced by variables such as race, treatment type and dosage, and patient age.
Limitations and future directions
Several limitations should be considered when interpreting our findings. First, the extent to which GDNF can cross the blood–brain barrier remains unclear, limiting our ability to directly link peripheral GDNF levels to central nervous system processes. Second, the limited number of studies and the heterogeneity of patient populations may have influenced the observed effects. Third, most research is cross-sectional, limiting insights into how GDNF levels change over time in relation to treatment response.
Importantly, potential publication bias must also be acknowledged as a limitation. The tendency for studies with positive results to be published more frequently than those with negative or inconclusive findings can skew our understanding of the true relationship between GDNF levels and SCZ. Future research should aim for comprehensive reporting practices that include all results—regardless of outcome—to provide a more accurate picture of this relationship.
Future research should focus on clarifying the precise mechanisms linking GDNF to SCZ, investigating potential therapeutic implications of GDNF modulation, and exploring its role as a biomarker for disease progression and treatment response. Additionally, examining relationships between GDNF and other biomarkers, such as inflammatory markers and neuroimaging findings, may provide further insights into SCZ's pathophysiology.




留言 (0)