
記住我



Nocturia, one of the most common urinary symptoms, affects 50 million people in the United States, but only 1.5 million receive specific treatment. Approximately 25% of the elderly have ≥2 nocturia episodes nightly. And nocturia is significantly associated with an increased mortality in the adults [1, 2].
A recent meta-analysis demonstrated that hypertension is a determinant of nocturia [3]. “Pressure-natriuresis” causing higher urine output at night than during the day has been considered to be a main mechanism [4]. In the Japan Morning Surge-Home Blood Pressure Study of 4310 patients with one or more cardiovascular risk factors, high evening home systolic blood pressure (BP) was an important indicator of multiple nocturnal voids specifically in the elderly [1].
Atrial natriuretic peptide (ANP) is a hormone produced by cardiac myocytes in the atria. ANP acts as a diuretic by increasing sodium excretion from the kidneys and thus water excretion. Atrial muscle cells contain volume receptors that release ANP in response to increased atrial fluid and wall stretch, which also occurs with the pressure and volume load caused by hypertension. B-type natriuretic peptide (BNP), which affects blood vessels and kidneys, is produced and secreted primarily by the heart, and its release is also regulated primarily by left ventricular volume expansion and pressure overload. Clinical studies have reported significant relationships of ANP [2] and BNP [5] with nocturia in patients with cardiovascular diseases. Therefore, high BP appears to act as the pathophysiology of nocturia.
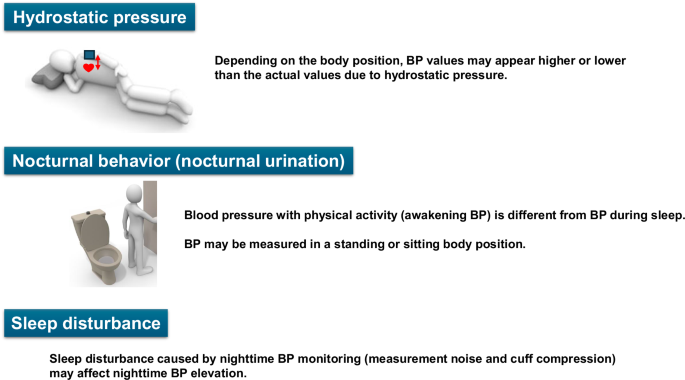
On the other hand, nocturia itself is associated with poor sleep quality that affects daytime functioning and increases the risk of falls at night. Nocturia could lead to sleep deprivation, which causes daytime fatigue and drowsiness. Additionally, the elderly with nocturia who make multiple nocturnal trips to the bathroom are at an increased risk of potentially serious falls [6]. Therefore, nocturia contributes to wakefulness during sleep and excessive hemodynamic changes due to orthostatic stress, which cause increased sympathetic nervous system activity during the night. Because nocturia is associated with cardiovascular disease [2], understanding the pathophysiology of nocturia is important for preventing cardiovascular disease.
The paper by Tabara et al. [7] in this issue of the Journal provides several new insights into the effect of nocturia on nocturnal home BP in the analysis of the Nagahama Study of 2418 community residents. Sleep systolic and diastolic BP in participants who experienced nocturnal urination during the one-week BP measurement period showed a linear increase with the frequency of urination. Furthermore, there was an intraindividual correlations between nocturnal urination frequency and sleep BP independent of baseline BP level [7]. The results in this study are important, as it shows that nocturia itself increased nocturnal BP. From the above, nocturia can be a risk of increased BP, which also leads to nocturia. The relationship between nocturia and hypertension is bidirectional, and create a vicious cycle.
Despite its relative frequency, nocturia is often under-reported, poorly managed, and inadequately treated. Various medications, foods and supplements can affect bladder storage and diuresis. Of these, the association between antihypertensive agents and nocturia is important regarding cardiovascular disease. In a cross-sectional study of 418 males aged 40 years or older, use of calcium channel blockers (CCBs) was associated with nocturia, but use of antihypertensive agents other than CCBs was not [8].
In addition, diuretics use is likely to be the one that deserves the most attention in relation to nocturia with cardiovascular disease. Specifically, in heart failure with high BP, timing diuretic therapy can help reduce nocturia in patients taking short-acting diuretics. Short-acting diuretics are usually prescribed to be taken in morning, but people with nocturia benefit most when taken in afternoon. Even if the patient is given diuretics twice a day, timing the afternoon can help promote urination while awake, and reduce nighttime urination [2, 6]. On the other hand, switching diuretics from morning to bedtime promoted nocturia and increased overnight urinations [9]. From a non-pharmacological perspective, bathing habits are gaining attention as an option for reducing nocturia. While warm water baths could lower nocturnal BP and improve sleep quality, warm water tub baths approximately 1 to 2.5 h before going to bed significantly reduced the prevalence of nocturia in the elderly [10].
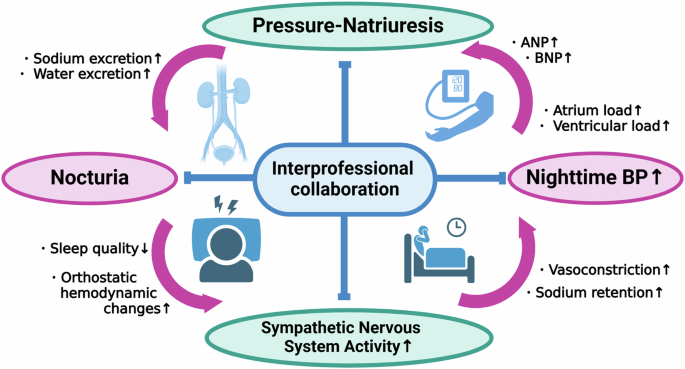
An interprofessional team of nurses, pharmacists, advanced practitioners and physicians could help address this issue in patients with adequate care coordination (Fig. 1). This interprofessional collaboration could improve quality of life, and reduce the risk of complications associated with nocturia, cardiovascular disease morbidity, and mortality [2]. Until now, nocturia frequently remains unrecognized, inadequately treated, and poorly managed. Particularly in the field of cardiovascular disease, there is little awareness of the relationship between nocturia and high BP. In this regard, the results reported by Tabara et al. [7] will generate interest in investigating this complex relationship through well-designed studies and interventions to reduce the burden of nocturia.
Fig. 1
Relationship between nocturia and nighttime BP. BP indicates blood pressure
留言 (0)