
記住我






Heart failure with preserved ejection fraction (HFpEF) represents a distinct form of heart failure, characterized by a left ventricular ejection fraction ≥50%. Its prevalence is increasing, with recent reports indicating it constitutes nearly or more than 50% of all heart failure cases. In contrast to heart failure with reduced ejection fraction (HFrEF), for which established pharmacological treatments, including the “fantastic four”—angiotensin receptor-neprilysin inhibitors (ARNIs) / angiotensin-converting enzyme (ACE) inhibitors/angiotensin II receptor blockers (ARBs), β-blockers, mineralocorticoid receptor antagonists (MRAs), and sodium-glucose cotransporter 2 (SGLT2) inhibitors—are well-recognized, the therapeutic landscape for HFpEF remains inadequately defined. Presently, only SGLT2 inhibitors are endorsed by clinical guidelines as an effective treatment for HFpEF. The pathophysiology of HFpEF is exceedingly intricate and heterogeneous, encompassing not only diastolic dysfunction but also a spectrum of pathological cardiac and extracardiac contributors, such as atrial fibrillation, chronotropic incompetence, obesity, and renal dysfunction. Despite significant progress, the precise mechanisms underlying HFpEF remain to be fully elucidated, underscoring an urgent need for the development of more effective therapeutic strategies.
Although both HFpEF and HFrEF fall under the umbrella of “heart failure,” they exhibit distinct characteristics. One notable difference is the predominance of females in HFpEF. Women constitute over 50% of HFpEF cases [1], a proportion significantly higher than the 20–30% observed in HFrEF. Moreover, sex-specific differences in clinical phenotypes have been documented in HFpEF. Female patients are more frequently associated with pronounced diastolic dysfunction and tend to experience worse prognoses [2]. Additionally, responses to pharmacological treatments, such as mineralocorticoid receptor antagonists (MRAs) [3] and angiotensin receptor-neprilysin inhibitors (ARNIs) [4], reportedly vary between male and female HFpEF patients. This underscores the necessity for further basic research to elucidate the underlying pathophysiological mechanisms and to develop optimized therapeutic strategies for female HFpEF patients.
Numerous rodent models have been developed to replicate the clinical features of HFpEF [5]. These include single-factor murine models, such as leptin-deficient mice, high-fat diet-induced models, and angiotensin II (Ang II) infusion models, as well as multifactorial models like the combination of uninephrectomy with aldosterone infusion, high-fat diet with L-NAME, or high-fat diet with Ang II infusion. Similarly, various rat models have been established, including Zucker diabetic fatty rats, Dahl salt-sensitive rats, spontaneously hypertensive rats, and aging models using Fisher F344 or F344/Brown Norway F1 rats. Among these, the Dahl salt-sensitive rat is one of the most extensively studied models for HFpEF. This model, a mutant of the Sprague-Dawley rat with heightened sodium sensitivity, develops left ventricular diastolic dysfunction when fed a high-salt diet. While these models have facilitated significant advancements in understanding HFpEF pathophysiology and exploring potential therapeutic strategies, the majority have been developed using male animals. Consequently, in vivo research on the pathophysiological characteristics of female HFpEF and sex-specific differences in HFpEF remains limited, highlighting a critical gap in this field of study.
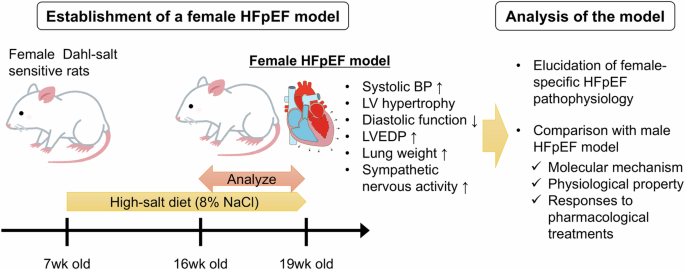
The study conducted by Nakashima et al. sought to establish a female HFpEF model using female Dahl salt-sensitive rats to address existing research gaps [6]. Female rats were fed a high-salt diet containing 8% NaCl from 7 weeks of age and were analyzed between 16 and 19 weeks of age. Rats subjected to the high-salt diet exhibited significantly elevated systolic blood pressure, increased left ventricular (LV) weight, and echocardiographic evidence of LV hypertrophy compared to control rats. Additionally, cardiomyocyte cross-sectional area and the expression levels of hypertrophic marker genes were markedly higher in the high-salt group. Although systolic function remained unaltered, echocardiographic assessments revealed impaired LV diastolic function and elevated LV filling pressures. Hemodynamic analyses demonstrated increased LV end-diastolic pressure and reduced LV relaxation in the high-salt diet group. Furthermore, normalized lung weight was significantly elevated, and renal function was notably impaired, supporting the manifestation of HFpEF in these female Dahl salt-sensitive rats. The authors also observed a significant enhancement in sympathetic nervous system activity in the high-salt diet group, as indicated by elevated plasma norepinephrine concentrations and an increased number of c-fos-positive neurons in the rostral ventrolateral medulla. These findings provide compelling evidence for the development of HFpEF in this novel female animal model.
While female Dahl salt-sensitive rats have been reported as models for hypertension, their use as a model for female HFpEF has been exceedingly rare. Consequently, the female HFpEF animal model developed in this study holds significant potential for advancing our understanding of the pathophysiology underlying female HFpEF and the sex-specific differences in HFpEF phenotypes. Previous clinical and preclinical research has proposed several mechanisms contributing to sex differences in diastolic function, including variations in calcium handling, protein kinase A activity, the renin-angiotensin-aldosterone system, and the nitric oxide synthase pathway [7]. However, the in vivo implications of these mechanisms on diastolic function and their influence on therapeutic responses remain largely unexplored due to the absence of suitable in vivo models. The female HFpEF model established in this study is anticipated to facilitate investigations into these unresolved issues, thereby offering new insights into sex-specific HFpEF pathophysiology and treatment responses.
A key significance of this study lies in its being the first to demonstrate heightened sympathetic nervous system activity in a female HFpEF model. While enhanced sympathetic nervous system activity is well-established as a critical therapeutic target in HFrEF, its role in HFpEF remains incompletely understood. Previous research has indicated increased norepinephrine production in the hearts of HFpEF patients compared to controls, suggesting augmented sympathetic activity in HFpEF [8]. However, the therapeutic efficacy of β-blockers in HFpEF patients has been inconsistent across studies, with some reports even suggesting deleterious effects [9, 10]. These inconsistencies may reflect the heterogeneity inherent to HFpEF, where sympathetic nervous system activity may vary widely among patients. The finding in this study that enhanced sympathetic activity is observed in a female HFpEF model raises the possibility of sex-specific differences in sympathetic nervous system activity, particularly in the context of HFpEF. Another hypothesis, as discussed by the authors, is that β-blockers may be insufficient in suppressing sympathetic nerve activity in HFpEF patients. This intriguing issue warrants further investigation using this model.
Several considerations must be addressed when extrapolating findings from this model to clinical HFpEF patients. First, the heterogeneity of clinical HFpEF must be acknowledged. Not all HFpEF patients exhibit overt diastolic dysfunction akin to this model. Indeed, approximately one-third of patients admitted with acute decompensated HFpEF reportedly lack echocardiographic evidence of diastolic dysfunction [11]. Recent phenotyping studies utilizing machine learning have classified HFpEF patients into diverse subgroups, including phenotypes characterized by hypertension and diastolic dysfunction, as well as those without apparent hypertension [12]. Appropriate patient stratification is therefore essential when applying findings from this model to the clinical context. Second, the disease progression in this model partially differs from that of clinical HFpEF. Dahl salt-sensitive rats are known to transit to systolic dysfunction following the diastolic dysfunction phase, which is relatively uncommon in clinical HFpEF [13]. These distinctions underscore the importance of careful interpretation and application of findings from this model to advance our understanding of HFpEF pathophysiology and therapeutic strategies.
In conclusion, the study by Nakashima et al. successfully established a female HFpEF rat model, which holds significant potential for advancing basic research into the female-specific pathophysiology of HFpEF and facilitating comparative studies with male counterparts (Fig. 1). Given the heterogeneity among clinical HFpEF patients, both basic investigations utilizing this model and clinical studies aimed at precise phenotyping of female HFpEF patients are crucial for deepening our pathological understanding and improving the prognosis of HFpEF, particularly in female patients.
Fig. 1
Establishment and analysis of a female HFpEF animal model. HFpEF heart failure with preserved ejection fraction, BP blood pressure, LV left ventricular, LVEDP left ventricular end-diastolic pressure
留言 (0)