
記住我


In children with disproportionate short stature, measurements are used to determine and track growth, both from the perspective of monitoring general health and development, and for recording responses to clinical treatment. It is recommended that practitioners track at least height, weight, and head circumference of children against standardized diagnosis-specific charts (e.g., achondroplasia [4, 19,20,21,22,23,24] or other short stature conditions [25,26,27,28,29]; Supplementary Table S2). Plotting weight and height immediately after measurement allows for re-measuring any individual points that appear to be outliers, to confirm their accuracy. If height and weight are used to calculate BMI, care should be taken to only make comparisons to BMI-for-age curves that are diagnosis-specific (e.g., achondroplasia [30]), as average stature BMI norms are inappropriate for this population.
Although it is not the focus of this commentary, we also recommend that anthropometric measurements and pubertal development (Tanner stage) are collected in combination with other developmental and health indicators that may also be potential indicators of response to clinical treatment. Indicators that should be considered include: developmental profile of the child, relative to diagnosis-specific charts [e.g., the Screening Tool for Everyday Mobility and Symptoms (STEMS) for skeletal dysplasia [31] or achondroplasia-specific development [32, 33]]; stamina and pain; and activities of daily living and independence skills.
To use growth and developmental charts, the child’s age should be determined and recorded correctly. In infants aged < 12 months, record the age in months, correcting for gestational age in the case of pre-term births. For children aged ≥ 12 months to ≤ 3 years, record age in months. For children aged > 3 years, record age in years and months.
The World Health Organization recommends measuring body length in children < 2 years old and standing height in children > 2 years old, unless unable to stand independently [34]. In children with disproportionate short stature, we recommend measuring both length and height in children aged ≥ 2 to ≤ 3 years. Note that, during this transition phase, there can be ~ 1-cm difference between body length and standing height measurement [35].
Outside of genetic disorders of skeletal growth, there is a strong genetic influence on height [36]. Thus, parental height may still have some influence on the height of children and adolescents with disproportionate short stature; for example, height variability in children with achondroplasia is strongly correlated with parental height [8]. Parental heights should be measured and recorded, particularly if one of the parents (or another family member) has the same form of disproportionate short stature as the child.
If a child with disproportionate short stature has pronounced genu varum/valgum and/or tibial bowing, or spinal deformities such as lordosis, kyphosis, or scoliosis, these may influence the accuracy of measurements. Therefore, the progression of these conditions must be followed over time. Although spinal deformities are best assessed via imaging, a simple lumbar spine lordosis measurement may be achieved by measuring the distance from the wall to the point of maximum lordosis. Scoliosis can also be assessed by letting the patient bend forward with their hands together and knees straight. If the back is tilted, there is a high possibility of scoliosis. Radiographic assessments must be performed on these patients [37, 38].
As children become older and with measurement experience, their capacity to cooperate with the anthropometrist during measurements will improve. However, any child may be or become uncooperative, particularly if tired. Therefore, the local SOP should include strategies for uncooperative or tired children, such as performing measurements at the beginning of each appointment, giving children short movement breaks between measurements, and providing small incentives (e.g., stickers) for each measurement achieved.
Specific Considerations for AchondroplasiaBoth overweight/obesity and underweight are of concern in all children. In those with achondroplasia, there are specific complications to consider. Weight loss, poor weight gain, or being underweight for age may be indicators of severe complications, such as cranio-cervical compression [4]. Head circumference measurement allows for monitoring of potential complications of achondroplasia, such as hydrocephalus, and should be measured regularly at least up to 5–6 years of age [8], and measurement every 1–2 years thereafter, up to adulthood, should be considered. Children with achondroplasia may have atypical range of motion in some joints, such as elbow contractures and/or hyperextended knees; however, accurate measurement of the range of motion requires a special instrument (a goniometer) and specialized training.
In children with achondroplasia, we encourage the measurement of sitting height/crown–rump length and arm span (Table 1). Sitting height and arm span are useful measurements for patients newly undergoing pharmacologic therapy for short stature, as these enable the monitoring of changes in body proportions.
Table 1 Recommended measurements in a clinical settinga for people with achondroplasia at different life stagesSitting height/crown–rump length are used along with standing height/body length to calculate the upper-to-lower body segment ratio as [5]:
$$}\text\frac}-\text}$$
(1)
OR
$$\text\frac}-\text}$$
(2)
Sitting height is also used in the sitting height-to-height ratio, another metric used to assess body proportionality is:
Another option to quantify the upper-to-lower body segment ratio in a patient who is able to stand is to measure the lower segment with a tape measure and subtract that value from the standing height. One end of the tape measure should be held at the top of the symphysis pubis while it is extended perpendicular to the ground at the sole of one foot. The patient should be standing evenly on both feet, with feet a minimal distance apart while still comfortably balanced [39].
Reference charts for these recommended measurements, as well as for other disproportionate short stature disorders, are listed in Supplementary Table S2. Additional anthropometric measurements that may be considered for some conditions are described briefly in Supplementary Table S3.
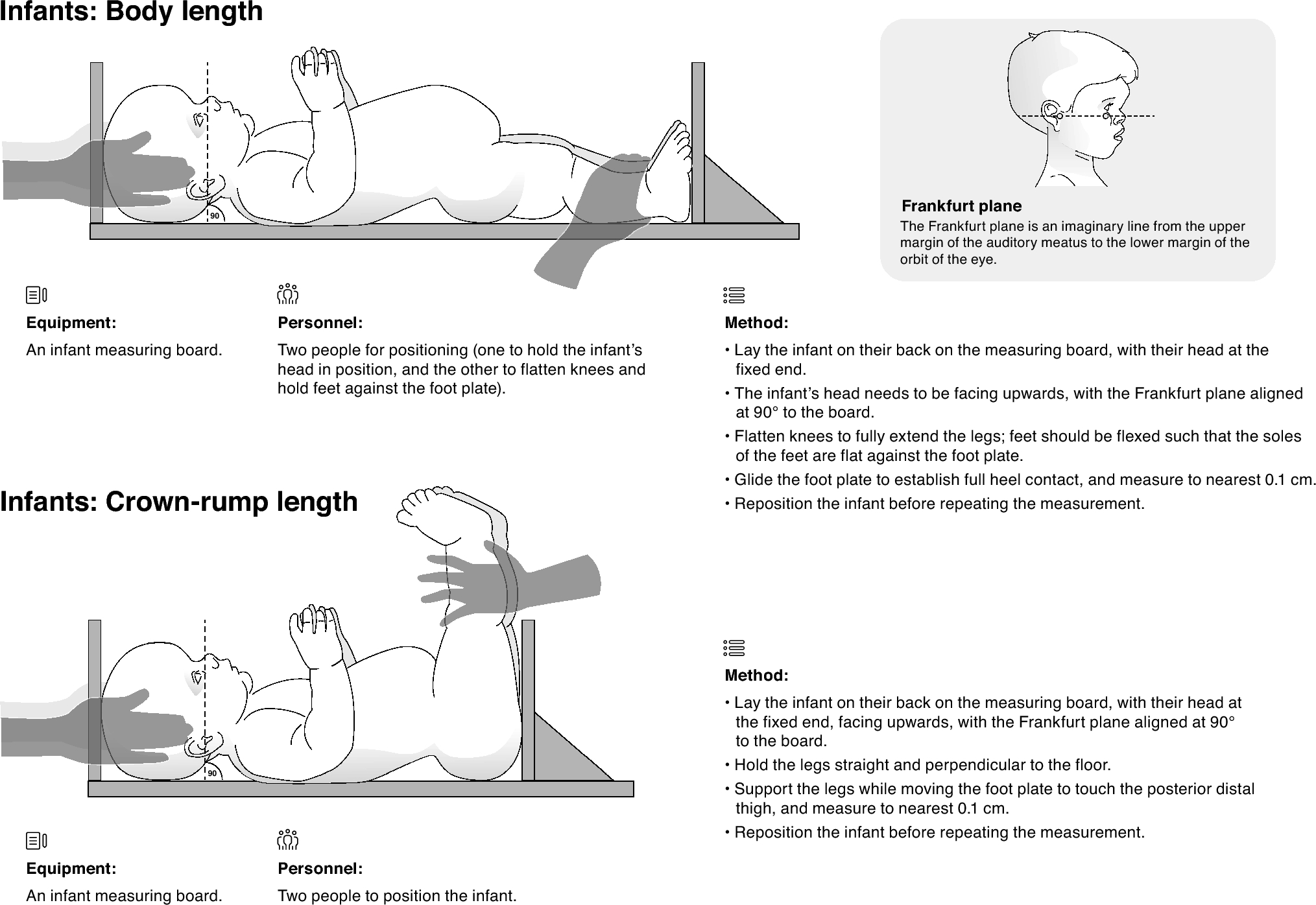
InfantsDuring infancy, regular measurements will include head circumference, weight, body length, and crown–rump length. Measurement techniques for infants are described and illustrated in Figs. 1 and 2. The measurements of infants require a minimum of two people, and it is often preferable that a parent/carer is involved in the measurement process; however, this should be at the discretion of the anthropometrist. A recorder can assist in measurements with guidance from the anthropometrist. Ideally, the recorder should also be familiar with the SOP, but this is not required.
Fig. 1
Anthropometric measurement techniques for infants with achondroplasia: body length and crown–rump length
Fig. 2
Anthropometric measurement techniques for infants with achondroplasia: head circumference
Toddlers and School-Aged ChildrenDuring the toddler years, the transition is made from measuring body length to measuring standing height, and from measuring crown–rump length to measuring sitting height. In addition, this is usually the age in which arm span is first measured. Measurement techniques for standing height, sitting height, and arm span are described and illustrated in Figs. 3 and 4.
Fig. 3
Anthropometric measurement techniques for toddlers and school-aged children with achondroplasia: standing height and sitting height. Note that the same techniques are also used for these measurements in adolescents and adults who are able to stand independently
Fig. 4
Anthropometric measurement techniques for toddlers and school-aged children with achondroplasia: arm span. Note that the same techniques are also used for these measurements in adolescents and adults who are able to stand independently
Standing height should only be measured in children who can stand independently for more than 1 min, which may exclude individuals with significant kyphosis or scoliosis, and is likely to be at an older age in children with achondroplasia. Sitting height can be measured once a child without significant kyphosis or scoliosis can sit erect unsupported.
For all measurements that will be taken regularly, it is advisable to choose measurement methods that can be maintained over time. For example, young children with achondroplasia may be able to stand with their feet together when standing height is measured, but, as they age, they may require a wider base for balance. For this reason, we recommend that standing height is measured with feet shoulder-width apart from the time standing height is first measured. It is also recommended when measuring standing height that the heels, buttocks, shoulders, and head are all in contact with the wall. If this is not possible, then a minimum of two contact points is recommended (head and buttocks), and the other points should be as close as possible to the wall.
AdolescentsGenerally, measurement protocols in adolescents will be the same as those for younger children (Table 1). However, in patients who have undergone leg lengthening procedures, problems may arise with some measurements. For example, if the calf muscles and Achilles tendons become tight, the heels of the patient may not touch the ground when standing straight, making it difficult to measure standing height. Moreover, during the leg lengthening process, an accurate weight measurement is not possible due to the fixation device (internal or external). In these patients, it may be useful to track measurements of waist and hip circumference during any period in which it is not possible to measure weight (see Fig. 5 and 6 for waist and hip circumference measurement techniques). However, we note that high-quality population norms for waist or hip circumference in adolescents with achondroplasia are not currently available.
Fig. 5
Anthropometric measurements for adults with achondroplasia: umbilical waist circumference [adapted from National Health and Nutrition Examination Survey (NHANES): Anthropometry Procedures Manual. 2021; https://wwwn.cdc.gov/nchs/data/nhanes/public/2021/manuals/2021-Anthropometry-Procedures-Manual-508.pdf]
Fig. 6
Anthropometric measurements for adults with achondroplasia: maximal hip circumference
An adolescent pubertal growth spurt is generally not present in children with achondroplasia and other short stature conditions [5, 22, 28].
Additional measurements that may be considered in adolescents are upper arm length and upper arm circumference (see Adult sections), knee to foot height, and tibial length (Supplementary Table S3).
留言 (0)