Data Source and Ethics Approval
This real-world, retrospective, observational study used anonymized patient data from June 2018 to December 2022, obtained from Medical Data Vision, a hospital-based claims database (Medical Data Vision, Tokyo, Japan) that covers approximately 42 million patients across 474 acute care hospitals in Japan. As all data were anonymized, requirements for ethics approval and informed consent under the Ethical Guidelines for Epidemiological Research in Japan do not apply to this study. Permission was obtained to access and use data by Medical Data Vision.
Data Collection
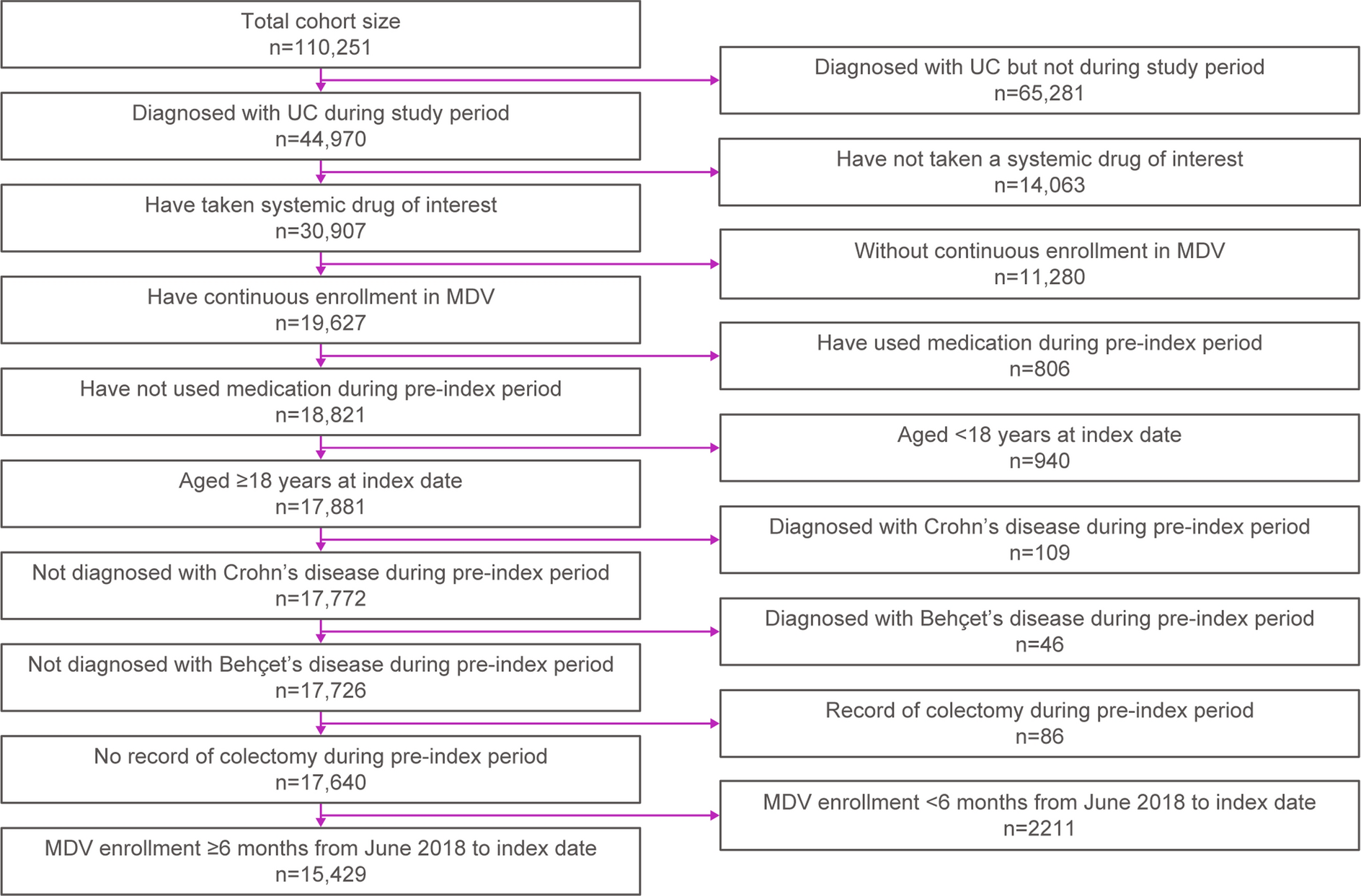
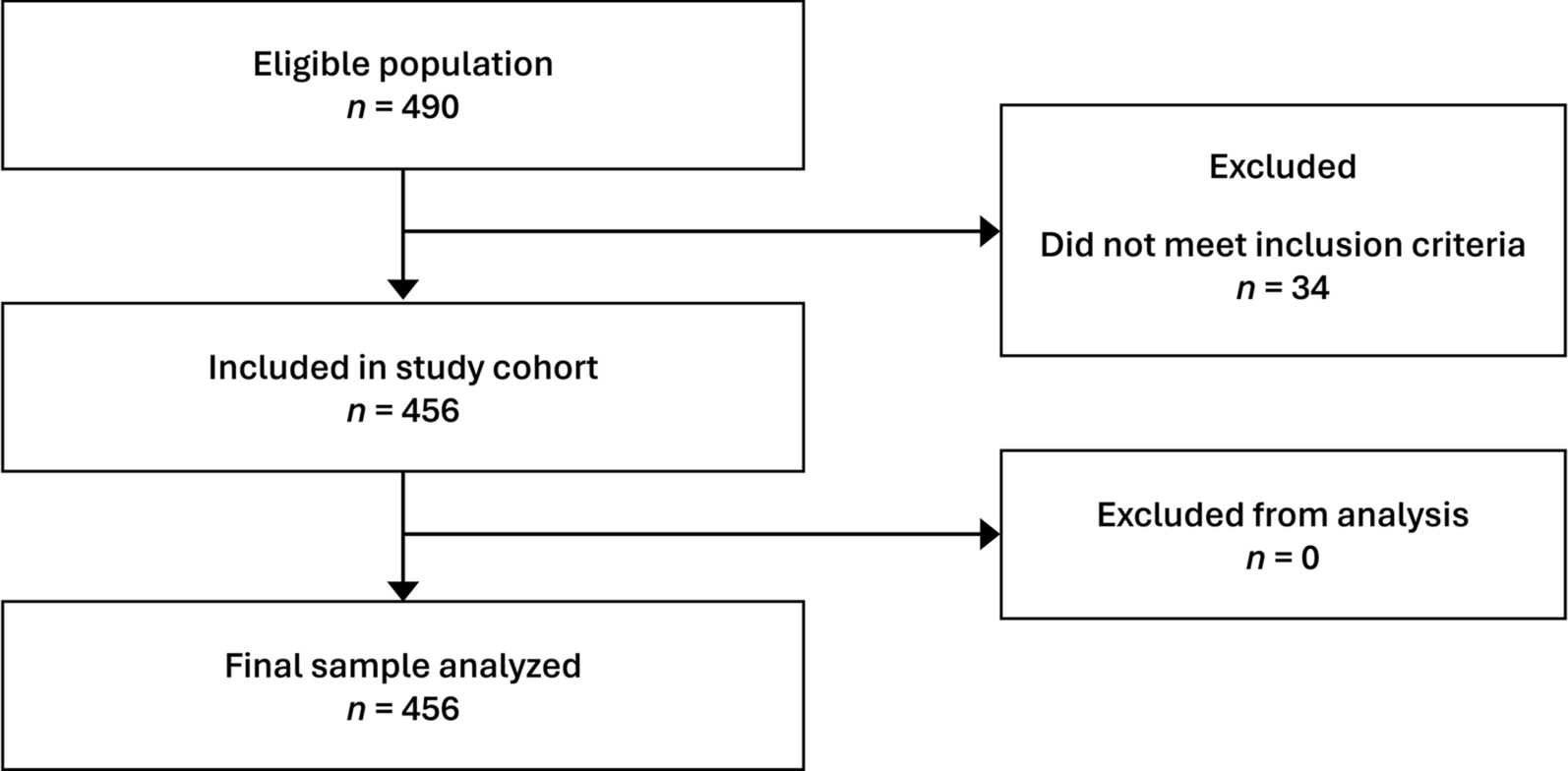
Patients were included if they had a confirmed UC diagnosis (International Classification of Diseases, Tenth Revision [ICD-10]: code K51) during the study period and, within the same month or 1 month before, were treated with an eligible systemic drug therapy: 5-ASA, corticosteroid, cyclosporine, tacrolimus, carotegrast methyl, azathioprine, 6-mercaptopurine hydrate, infliximab, adalimumab, golimumab, ustekinumab, vedolizumab, tofacitinib, filgotinib, or upadacitinib. The first claim of systemic treatment within the study period was defined as the index date. Patients were also required to have had continuous enrollment in the database for ≥ 6 months prior to and ≥ 12 months after the index date. Patients were excluded if they had a claim of systemic treatment during the pre-index period, were aged < 18 years at the index date, or had a confirmed diagnosis of Crohn’s disease or Behçet’s disease or a record of colectomy during the pre-index period.
Outcomes
Demographic variables collected included age, sex, and disease extent at the index date, and Charlson comorbidity index (CCI) score during the pre-index period, which was calculated using a validated method [15]. Outcomes of interest for the primary objectives included treatment classes at each line of therapy, with each line defined by the initiation of a treatment regimen for ≥ 30 days until that regimen’s modification (i.e., discontinuation, switch, add-on, reduction, or restart); number of lines of therapy; number of patients discontinuing, switching, adding-on, reducing, or restarting treatments; number of patients prescribed a course of corticosteroids (defined with a ≥ 60-day gap between courses); and number of patients suboptimally treated with corticosteroids. Treatment discontinuation was defined as no prescription of the index treatment during the 60 days after the period covered by the previous prescription, with no further treatment line initiated. Treatment switch was defined as the prescription of a new treatment during the period covered by the last prescription or during the following 60 days, but with the same total number of drugs in the index regimen. Treatment add-on was defined as the prescription of a new treatment during the period covered by the last prescription or during the following 60 days, with a greater number of drugs in the subsequent regimen than in the previous regimen. Treatment reduction was assessed for patients receiving ≥ 2 treatments and was defined as discontinuation of ≥ 1 treatment. Treatment restart was defined as initiating a subsequent line of therapy using the same regimen as in the previous line. For the line of therapy analysis but not for the other objectives, patients with inpatient records only were excluded from analysis.
Outcomes for the secondary and exploratory objectives included HCRU, costs, and presence of EIMs pre- and post-index. HCRU was described by the number of UC-related outpatient visits, UC-related hospitalizations, UC-related surgeries, and cytapheresis use within 1 year from the index date. Mean direct costs in Japanese yen were adjusted for inflation with 2022 as the reference year (based on the calendar year average of the Consumer Price Index) and are reported per person per month (PPPM) for UC-related inpatient visits, UC-related outpatient visits, and UC medication, measured separately and in total. HCRU and costs are reported for the overall population as well as for patients who moved to advanced therapy within 1 year of their index date and who did and did not experience suboptimal treatment with corticosteroids.
Patients who experienced EIMs at baseline and those who developed EIMs during the study period are reported, and treatment patterns before and after observation of an EIM code are described.
Statistical Analyses
This study was primarily descriptive in nature. Categorical variables are described with counts and frequencies, while mean values and standard deviation (SD) are given for continuous variables. P values for differences in HCRU and costs between patients who did and did not receive suboptimal treatment with corticosteroids were derived using Fisher’s exact test for categorical variables and Wilcoxon rank sum test for continuous variables.
Univariate logistic regression analyses were used to identify factors associated with suboptimal treatment with corticosteroids in patients who moved to advanced therapy within 1 year of their index date, such as age, sex, CCI score, disease extent, treatment changes (including adding a thiopurine in a subsequent line of therapy), cytapheresis use, or UC-related hospitalization.
Statistical analyses were conducted using R Statistical Software (version 4.2; R Foundation for Statistical Computing, Vienna, Austria).





留言 (0)