
記住我






The index case presented here illustrates the potential value of routine BRAF studies in the evaluation of suspected RCC. Potential alterations in management following a revised diagnosis to pCP include more frequent follow-up, consideration of revision surgery in the appropriately selected patient, and consideration of BRAF/MEK inhibitor therapy which is currently transforming the treatment paradigm of pCP [5]. However, missed pCP in the RCC setting appears to be an uncommon phenomenon as this occurred in only 1/11 (9%) of the overall retrospective cohort.
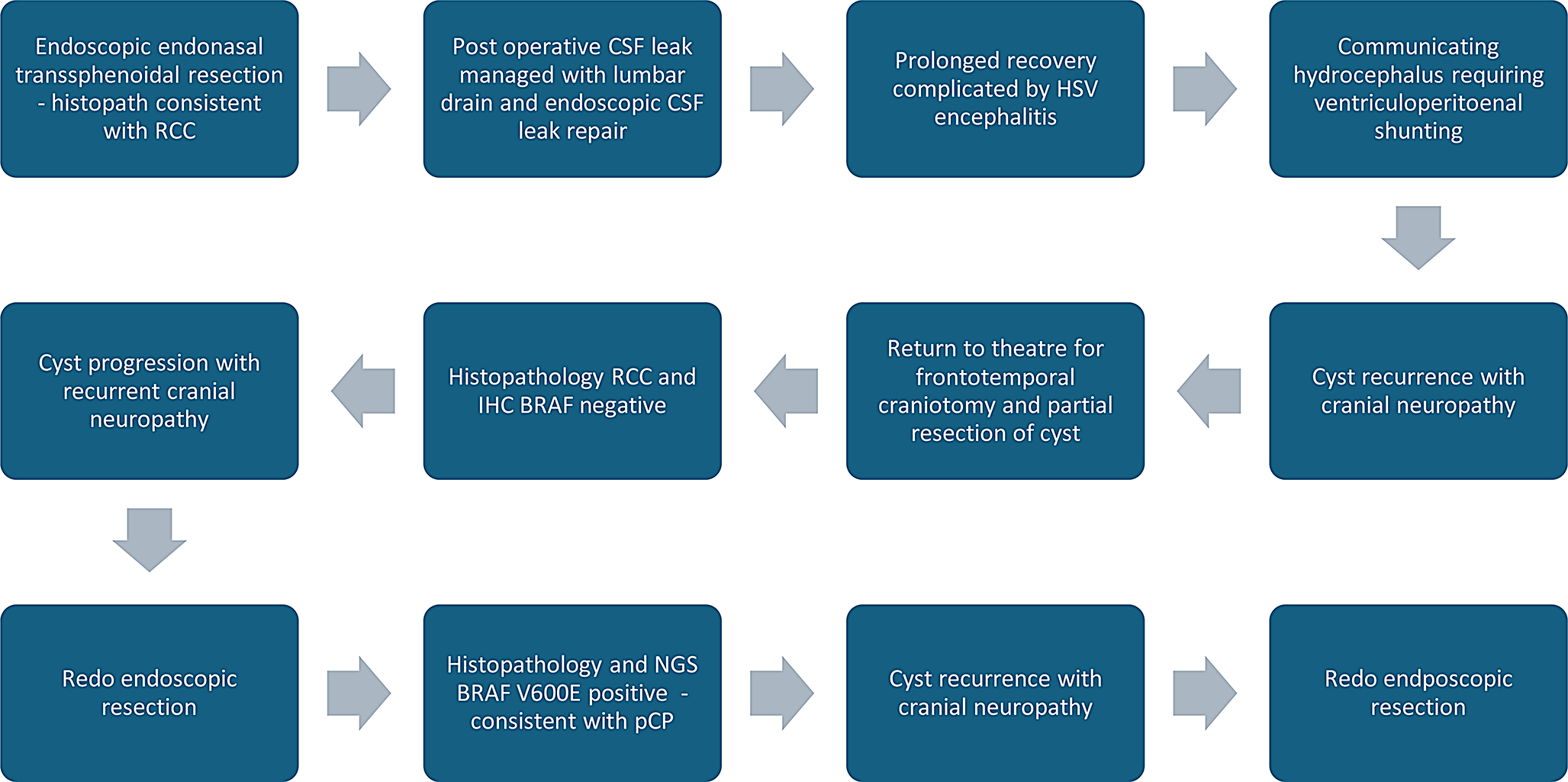
The index case initially demonstrated a cyst lined by cuboidal and columnar epithelium with apical mucin, without cytological atypia or squamous metaplasia. As such, BRAF IHC was not undertaken. At the first revision surgery repeat specimens demonstrated columnar epithelium with apical mucin again without squamous metaplasia but the presence of a neutrophilic infiltrate. BRAF IHC was negative on these specimens. The second revision surgery demonstrated squamous metaplasia that had weak staining to BRAF IHC and NGS detected a BRAF V600E mutation, confirming the diagnosis of pCP (Fig. 2).
It is possible that the patient’s outcome may have been different had a diagnosis of pCP been made earlier in their treatment course. Therefore, it would be reasonable to consider routine BRAF IHC for non PitNET sellar and suprasellar lesions with molecular BRAF testing considered individually.
Fig. 2
Left image is an H&E stain demonstrating portions of squamous lined cys, with underlying fibrous tissue and a minor acute inflammatory infiltrate. Right image is a BRAF V600E stain demonstrating pale staining of the squamous epithelium but focal darker staining of the normal cilia. Both images at 10x magnification
Schweizer et al. examined 33 RCC specimens and 18 pCP specimens and found that 30/33 RCC specimens were negative by BRAF IHC. The three cases with RCC and positive BRAF immunochemistry had unusual clinical courses, with two being re-diagnosed as pCP and one having a past diagnosis of a pCP.
These cases demonstrate the role molecular testing can play in the work-up of non-PitNET lesions of the sella. IHC has a fast turnaround time but interpretation within the CNS and pituitary can be difficult with susceptibility to interobserver variation. NGS is a more specific test, but accessibility has traditionally been an issue. Impediments to NGS testing include increased turnaround time (10–21 days vs. 1–2 days for IHC), cost (1,000–4,000 USD vs. 40–140 USD) and tissue requirements (> 8 formalin fixed paraffin embedded (FFPE) sections vs. 1 FFPE section, and 50ng – 2microg DNA/RNA vs. 50 tumour cells) [11]. These limitations are becoming less significant with more efficient NGS and bioinformatic processes that allow turnaround in a similar time frame to IHC and equivalent costs at certain facilities.
In the present study, both IHC and NGS were available, with complementary advantages. IHC was able to be performed in all cases, whereas there was inadequate tissue for NGS in 3/11 cases. On the other hand, NGS offered definitive results in all cases with adequate tissue with no evidence to suggest a false-positive result (as suspected in the positive IHC result in case 9 which lacked other pCP features such as squamous metaplasia and recurrence) or a sampling error result (as suspected in the initial negative IHC result in the index case).
留言 (0)