Policy initiatives such as bundled payments and pay-for-performance incentivize hospital leadership to focus on reducing the excessive utilization of hospital resources [23, 24]. These efforts also include reducing LOS [3]. Since intraoperative and immediate postoperative complications can prolong LOS, it is often considered a proxy for the quality of care provided to patients [25]. Consequently, efforts are being made to develop protocols that facilitate shorter hospital stays following surgery for pituitary adenomas [26, 27].
However, in non-neurosurgical literature, it has been found that up to 50% of the variation in extended LOS cannot be explained by hospital complication rates [3]. Moreover, the relationship between LOS and the effectiveness and efficiency of care is not always straightforward [2]. Since non-clinical factors, such as insurance status and discharge disposition, play a significant role in LOS, some authors do not support using LOS as a quality metric for efficient hospital management unless it is appropriately adjusted for non-clinical characteristics [2].
To complicate the issue further, there is no consensus among authors on what should be considered PLOS after ETPS [12, 14,15,16,17]. With this background, we report the impact of various clinical and non-clinical factors on LOS after ETPS using varying definitions for PLOS. To the best of our knowledge, our study is the only single-institution study highlighting the influence of non-clinical factors on LOS after ETPS, while controlling for clinical variables. We believe our study will help stimulate discussions within the neurosurgical community to work towards a consensus on the definition of PLOS and serve as a foundation for developing processes to reduce the influence of non-clinical factors on LOS after ETPS.
Study overview
In our study cohort, the median LOS was 3 days, the 75th percentile of LOS was 4 days, and the 90th percentile was 6 days. We confirmed our primary hypothesis that predictors for PLOS are influenced by the definition used for PLOS.
Upon multivariate analysis, preoperative KPS was negatively associated with PLOS across all definitions. Non-clinical factors, such as non-private insurance and non-home discharge disposition, were also consistently associated with PLOS. Preoperative tumor volume and postoperative hyponatremia were significant predictors of PLOS using the > 75th percentile and > 90th percentile definitions but did not reach significance in the greater than median definition. Lastly, race and cavernous sinus invasion were significantly associated with PLOS > median, while intraoperative CSF leak was only significantly associated with PLOS > 90th percentile.
Patient characteristics
Preoperative KPS was the only factor found to be statistically significant in both univariate and multivariate analyses across all three definitions used in our study. No other preoperative variable was found significant in multivariate analysis across all definitions. This suggests that a patient’s overall functional status and ability to perform activities of daily living directly impact their hospital stay duration. Regarding associated medical comorbidities, hypertension was significant only in univariate analysis when PLOS was defined as > 75th percentile. It was not statistically significant for other definitions or in multivariate analysis. Similarly, Vimawala et al. noted hypertension as a significant predictor in univariate analysis when PLOS was defined as the 90th percentile [16]; however, it was not significant in multivariate analysis. Contradicting our findings, one study did not find a significant impact of hypertension on PLOS defined as > 4 days [14]. BMI was not significantly associated with prolonged length of stay (LOS) under any definition used, which contrasts with findings from a previous study that identified a significant association between BMI and complications such as CSF leaks and infections—factors known to contribute to PLOS [16, 28].
Another comorbid condition found to be significant in univariate analysis was atrial fibrillation when PLOS was defined as > 75th and > 90th percentile. This finding is consistent with Vimawala et al. [16]. While other studies found obstructive sleep apnea on CPAP, bleeding disorders, and insulin-dependent diabetes mellitus to be significant predictors [15, 16], we did not observe any significant differences for diabetes mellitus, obstructive sleep apnea, or anticoagulant use in our cohort across any definitions. Our study lacks details on the type of diabetes, obstructive sleep apnea, and bleeding disorders, which could help explain these differences. We found mFI-5 to be significant only in univariate analysis when PLOS was > 75th percentile (4 days). Similar to our findings, Khalafallah et al. found that each point increase in mFI-5 was associated with an increase in LOS by 1.65 days [29]. Additionally, Vasan et al. found Charlson Comorbidly Index to be significant in univariate analysis using the definition of PLOS > median (3 days) [12]. However, we did not find mFI-5 to be significant in univariate analysis when using the definition of PLOS used by Vasan et al.
Preoperative visual disturbances were found to be significant in univariate analysis for all PLOS definitions. In contrast, preoperative headache was only significant at the 75th and 90th percentile definitions in univariate analysis. None of the other studies have evaluated the impact of these symptoms on PLOS.
Adenoma characteristics
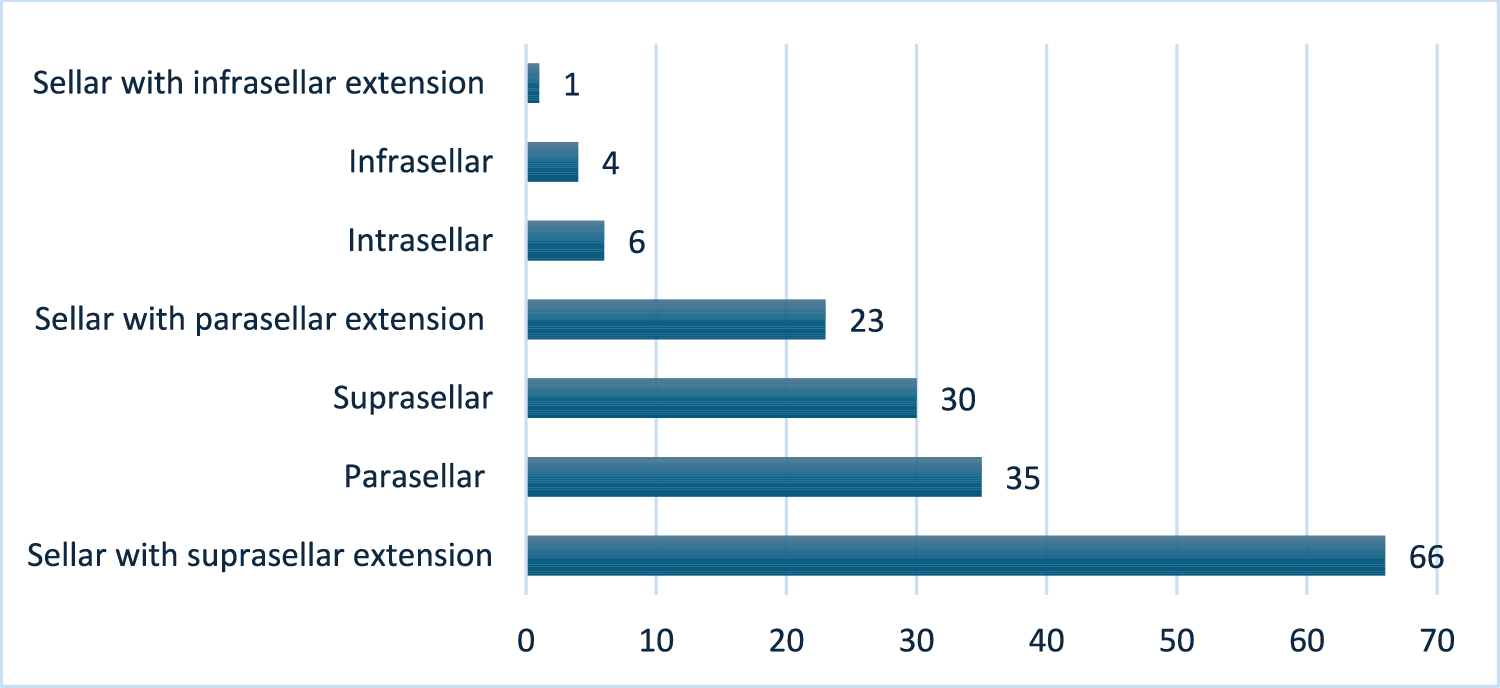
Cavernous sinus invasion, preoperative tumor volume, and chiasm compression were significantly associated with PLOS in univariate analysis across all PLOS definitions. However, in multivariate analysis, cavernous sinus invasion was the only tumor characteristic that significantly associated with PLOS defined as > median LOS. When the definition of PLOS was changed to > 75th and > 90th percentile, cavernous sinus invasion was no longer significant on multivariate analysis. Instead, preoperative tumor volume emerged as a significant predictor of PLOS under these definitions. Similar to our findings, Devarajan et al. found that maximum tumor dimension was a significant predictor of PLOS defined as > 4 days in multivariate analysis [14]. This author also noted that previous radiation therapy a was significant factor in univariate analysis [14]. However, we were unable to confirm this finding in our study. This discrepancy may be due to the higher percentage of patients with prior radiation therapy in their study cohort compared to ours (2.9% vs. 1.23%) [14].
Operative characteristics
Upon univariate analysis, only duration of surgery was found to be a significant factor across all definitions of PLOS. No other intraoperative factor was significant when using a definition of PLOS > median. However, upon changing the definition to > 75th and > 90th percentile, intraoperative CSF leak, EOR, residual tumor volume, and use of lumbar drain were found to be significantly associated with PLOS. Other authors also noted duration of surgery and intraoperative CSF leak to be significantly associated with PLOS on univariate analysis [14, 16]. On the other hand, on multivariate analysis, none of the intraoperative factors were found to be significant across all definitions. One factor, intraoperative CSF leak, was a significant predictor of PLOS when defined as > 90th percentile. Our findings align with those of Vimawala et al., who also found that intraoperative CSF leak was the only intraoperative factor significantly associated with PLOS > 90th percentile [16].
Postoperative outcomes
Hyponatremia was identified as a significant clinical factor associated with PLOS in univariate analysis across all definitions used. However, upon multivariate analysis, it was a significant predictor of PLOS only for the definitions of > 75th and > 90th percentiles. Other single-institution studies did not analyze this parameter but noted postoperative CSF leak as a significant factor in both univariate and multivariate analyses for PLOS > 4 days and > 90th percentile. In our study, postoperative CSF leak was not a significant factor with PLOS > median but was significant on univariate analysis for PLOS > 75th and > 90th percentiles. Upon multivariate analysis, postoperative CSF leak was significant only when using the PLOS > 90th percentile definition. Contrary to other studies, we did not find diabetes insipidus to be a significant predictor of PLOS [14, 16]. Studies in neurosurgical literature also show non-neurosurgical complications such as pulmonary embolism, deep vein thrombosis, and urinary tract infections to impact LOS [30, 31]. We found the rates of only deep vein thrombosis to be significantly different between non-PLOS and PLOS when defined as > 75th percentile. However, we did not find a significant difference in these variables within our cohort in any of other definitions evaluated.
Non-clinical predictors of PLOS
Along with preoperative KPS, non-private insurance and non-home discharge disposition were the only factors that were consistently significant across all definitions on both univariate and multivariate analyses. Similar to our results, in a study based on the NIS database, Vasan et al. found Medicaid to be a significant factor associated with PLOS defined as > median stay (3 days) [12]. A study from non-neurosurgical literature, involving 313,144 patients from the National Trauma Database, noted that patients with Medicaid had a significantly longer LOS compared to those with private insurance [2]. This study also noted that discharge disposition had the greatest effect on LOS, with patients discharged to nursing homes and rehabilitation facilities experiencing longer LOS [2]. This data clearly highlight role of non-clinical parameters in patients’ hospital stays.
Additionally, low income was significant across all definitions on univariate analyses but only for PLOS > median for multivariate analyses. This correlates with another study that found lower income to be associated with frailty [30]. Presumably, patients with lower income face greater barriers to assessing timely healthcare, causing to delayed hospital visits, increased frailty, and more advanced disease presentation which in turn contributes to PLOS. When using the definition of PLOS > median, we found that race was significantly associated with PLOS in both univariate and multivariate analyses, while ethnicity was significant only in univariate analysis. Both race and ethnicity were not statistically significant in either univariate or multivariate analyses when the definitions of PLOS > 75th percentile and > 90th percentile were used. Using the NIS database and defining PLOS as > median (3 days), Vasanth et al. showed that female, Black, and Hispanic patients were more likely to experience PLOS [12]. Similarly, an analysis of the NSQIP database involving 11,510 patients undergoing craniotomies for tumors found that African American and Hispanic patients experienced PLOS [31].
Limitations and strengths
Our study is inherently limited by its retrospective nature. To overcome these limitations, we included only patients with complete records available. Additionally, it is a single-institution study. Therefore, validation in larger cohorts and multi-institutional collaborations is needed.
Despite these limitations, to the best of our knowledge, we report the largest single-center series showing the predictors of PLOS in patients undergoing ETPS for PA and how these predictors vary by the definition of PLOS used. Compared to generic database efforts to characterize predictors of PLOS, our study has significant granular data regarding preoperative characteristics, tumor characteristics, and postoperative outcomes which are not always readily available in various databases. As such, we believe that our results highlight clinical predictors common across various definitions of PLOS as well as the significant role of non-clinical variables in PLOS. None of the single-institution studies have evaluated the impact of these non-clinical factors on PLOS.









留言 (0)