Patient satisfaction after TKA is one of the most important issues facing doctors and patients. Different prosthesis designs lead to varied knee kinematics and result in discrepant satisfaction rates. Despite efforts to mimic the motion of the natural knee, paradoxical anterior movement is still a common phenomenon after TKA and leads to various discomforts, such as pain caused by patellofemoral impact during flexion, which reduces patient satisfaction and joint function scores. PS prostheses may exhibit this phenomenon during normal walking, deep squatting, and other activities. MP prosthesis theoretically prevents paradoxical anterior movement [6, 9, 13].
Both PS and MP designs have shown good results in follow up studies when patients outcomes were evaluated through radiography or specific health status measures for knee OA, including American Knee Society Score, Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC), Oxford Knee Score. As already stated, MP prosthesis showed knee kinematics closer to physiological condition, reduction of polyethylene wear process and better clinical outcomes, compared to PS design. Steinbrück et al. in an in-vitro study, showed reduced contact pressure on the medial compartment for the MP prosthesis when compared to the PS prosthesis at different flexion degrees. Contrasting results were found regarding knee flexion–extension range of motion (RoM), with some authors claiming a significant RoM increment for MP design compared to PS design, while other authors showed no difference between these prostheses [14, 15].
The trend for OKS in our study is the same in both groups, but with higher mean values in the MP group. The trend of WOMAC pain, stiffness and disability score is the same in both groups, but with higher mean values in the PS group at one year and two years. KSS clinical and functional score is the same in both groups, but with higher mean values in the MP group. The most important score is forgetten joint score which is favourable for the MP group in our study.
Multiple studies have reported favourable outcomes for the MP, with satisfactory results at medium to long-term follow-up. Fan et al. reported improvements in the ROM and pain scores at five year follow-up. Bordini et al. also reported good outcomes of the MP-TKA, having a ten year survivorship estimate of 96.6%, higher than all other cemented TKA. The highly conforming design of the MP-TKA may contribute to reduced polyethylene wear and osteolysis, resulting in improved survivorship [16,17,18].
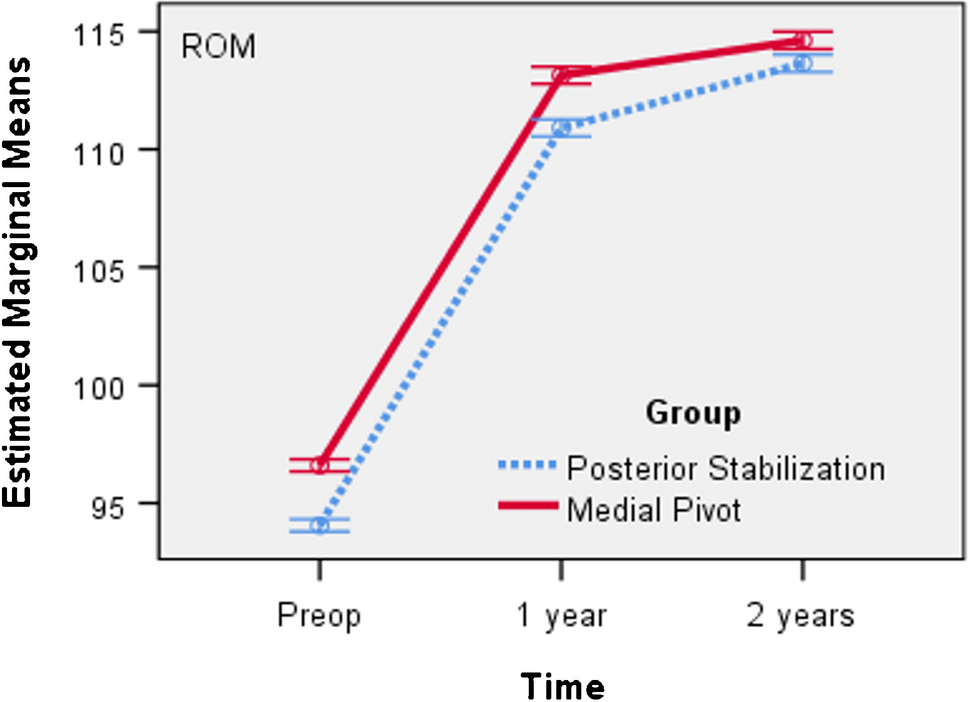
The MP motion is important for the prevention of patellofemoral complications because it reduces the patellofemoral contact pressure, suggesting that restoration of normal tibiofemoral kinematics may result in a decreased risk of patellofemoral problems, such as anterior knee pain. One randomized controlled trial (RCT) showed a greater ROM with a medially conforming ball-and-socket prosthesis compared with the PS-TKA at both one year and two year follow-up. The trend of ROM is the same in both groups, but with higher mean values in the MP group. Contrary, another study reported a worse outcome for an MP-TKA compared with a mobile-bearing prosthesis [19].
FJS provides a better measure of high-end functionality post arthroplasty. Patients' expectations of outcomes after surgery have dramatically changed over the last years, as patients are now expecting higher levels of functionality after TKA. The FJS has been validated in several studies. Very few studies have used the FJS to compare a fixed bearing TKA with a mobile-bearing TKA. Several studies have been carried out comparing the MP-TKA with the PS-TKA using other patient-reported outcome measures. These include the WOMAC, SF-36, Knee Society Score (KSS), and Oxford Knee Score [20,21,22].
At present, there are a few studies on the use of the FJS, which has the advantages of a tool with high structural validity and high reliability for repeated testing, with the upper limit effect of the FJS being lower compared to WOMAC. In previous studies, patients in the MP group had a higher final FJS score than the PS group, because a high degree of stability is required when the knee joint is straightened from the flexion state. In contrast, the cam mechanism of the PS prosthesis will produce higher contact stress, which leads to knee instability, thereby affecting the ability of the knee joint to change from high flexion to straight extension. Therefore, the FJS score in the PS group was lower than that in the MP group [7, 23, 24].
Hossain et al. found a statistically significant difference in the physical elements of the SF-36 and Total Knee Function Questionnaire scoring systems, favouring the medially conforming ball-and-socket prosthesis over the PS-TKA [19]. Pritchett compared patient preference between five types of TKA design in patient with staged bilateral TKA. MP TKA was shown to have higher preference over PS TKA (76.2 vs 9.5%), cruciate retaining (CR) TKA (76 vs 12%) and mobile-bearing (MB) TKA (61.4 vs 30.1%) [25].
A retrospective study on two groups of patients by Samy reported superior FJS in MP TKA than in PS TKA (59 vs 44) at one year. The FJS in his study was somehow quite low in both groups. There were very few other studies reporting FJS as the outcome [7]. Batra et al. have found significantly better patient satisfaction and expectations in the MP group as compared to the PS group throughout the follow-up period. This study demonstrated superior sagittal knee kinematics in MP knee as compared to PS knee. The knee kinematic activity represents both the tibio-femoral and the patella-femoral joint and it involves standing from a sitting position: a routine daily activity which requires reasonable amount of mid-flexion stability. We found biomechanical instability two times more frequent in PS group than in MP group [26].
The Australian Orthopaedic Association National Joint Replacement Registry has revealed that the MP prosthesis has a higher rate of revision TKA compared with other types of prosthesis. Loosening and patellofemoral pain were the main modes of failure leading to revision, with 1.6% and 1.2% for the primary Advance MP prosthesis compared with 0.9% and 0.4% for all other types of TKA [27].
According to Papagiannis et al.’s kinematic and kinetic analysis, early outcomes could not demonstrate any notable functional and wear advantages between the two groups. Likewise, Benjamin et al.’s study revealed comparable functional grades for both PS and MP groups. However, a level I RCT by Kim et al. showed strong preferences for the non-MP implants as they obtained smaller ranges of knee motion, less patient satisfaction, and a higher complication rate in fixed bearing MP prostheses in their early outcome, despite similar long-term fixation and survival rates of both MP and PFC Sigma prostheses in their subsequent report [19, 28]. As acknowledged by Shakespeare et al. we also found most MP knees to be inherently stable, which was an objective assessment of stability by conventional methods of evaluation of achieving equal medial and lateral gaps through 0° to 90° flexion intraoperatively [29].
Nisar et al. found no significant differences in KSS or WOMAC scores when comparing MP-TKA to PS-TKA. MS TKA having no clear advantage/disadvantage in clinical or patient outcome measures, when comparing to all other implant designs, may be a result of a medial pivot motion in TKA not correlating with improved clinical outcome. Studies correlating intra-operative medial pivot patterns with post-operative outcomes have been conflicting. Nishio et al. demonstrated patients with a medial pivot pattern identified using intraoperative CT-based navigation achieved better post-operative outcomes. However, Warth et al. used intra-operative digital sensor technology to correlate intra-operative kinematic patterns with post-operative outcomes. The authors observed no difference in post-operative outcomes between those patients with a medial pivot pattern and those without [30, 31].
Macheras et al. found that the function of the knee greatly improved after TKA using MP in 325 patients, as assessed by the Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC), Short Form (SF)−12, and Oxford Knee scores25. Karachalios et al. found that the 15-year cumulative survival rate of MP reached 97.7% and that the average ROM was 117 (85–130). These studies had the longest follow-up published in literature. There was also no preference in our study in prosthesis selection in relation with the deformity type, varus or valgus, similar with other findings from literature [9, 32, 33].
Persistent pain after TKA is still the major problem affecting the improvement of satisfaction in our study and the number of patients with pain in anterior knee area was double in the PS group comparative with MP group. We found a significant correlation between pain or ROM and patient satisfaction. Pain in the anterior knee can be caused by dysfunction of the patellofemoral joint in the anterior knee region, abnormalities in the patellar trajectory, and high contact stress of the patellofemoral joint after surgery. The PS prosthesis requires an intercondylar box to accommodate the column, and when the knee joint changes from flexion to extension, the patella will touch the intercondylar box. The long-term consequences are hyperplasia of the fibrous tissue nodules, which get in contact with the intercondylar box of the PS prosthesis, and cause pain in the anterior part of the knee during the extension to 30–40°. After oral administration of nonsteroidal anti-inflammatory analgesics for two months, the symptoms gradually disappeared, without adversely affecting postoperative functional recovery [34].
The phenomenon of clicking sound after knee arthroplasty is quite common. The main reason is that small nodules of the fibrous synovial hyperplasia at the superior junction of the quadriceps tendon and patella are stuck in the intercondylar fossa during movement of the knee joint. The box restricts the upward movement of the patella. When the small nodule pops out of the intercondylar box, the patella suddenly moves upwards and produces a snapping sound. The average time for the clicking sound to occur for the first time is five to 11 months. In the MP group, three patients with postoperative clicking sound was observed, while 65 patients with clicking presented in the PS group, which occurred mainly during the process of knee joint flexion to extension.
There is no difference for infection rate between the two groups. We annalysed superficial infection which was treated with oral antibiotics, early infection which needed washing and insert exchange and late infection which imposed two stage revision surgery.
Based on the findings of the present study, the choice between MP and PS TKA is still open to surgeons’ own preference. Both designs give comparable satisfactory clinical results. The incidence of postoperative complications in general is lower than the overall level, which shows that the two types of prostheses are safe and reliable. Since patient satisfaction is also affected by many other factors apart from implant design, the relative significance and the interplay between different factors may be the direction of future research.



留言 (0)