This study validates the effectiveness of arthroscopic SCF in patients with stage IIIB and IIIC Kienböck’s disease with satisfactory clinical, radiological, and functional results without the need for bone graft; as fusion was achieved in an average of 7.2 weeks.
This minimally invasive surgery depends on combining the advantages of arthroscopy, dry technique, percutaneous fixation, and not requiring bone graft; all leads to the hoped-for outcome achieved by minimizing surgical insult to the wrist.
Arthroscopy has wide intra-articular exposure of the wrist, causing minimal damage to the ligaments and capsule thus preserving the blood supply to the carpals and preserving joint mobility which leads to more rapid healing [9]. The posterior interosseous nerve is also preserved and the proprioception of the joint is maintained, resulting in less arthritic changes and preferable healing [9, 13, 14].
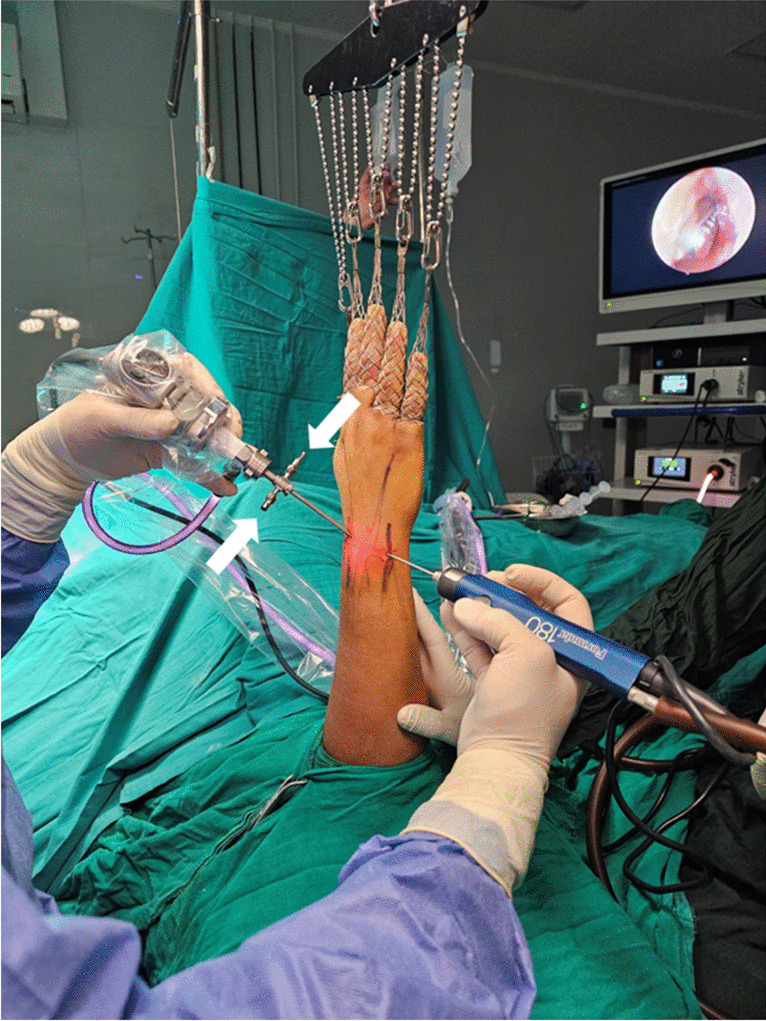
Dry wrist arthroscopy was chosen in this study due to its obvious advantages of good clarity due to the index of reflection of the air, which is inside the joint, being very close to one. Accurate visualization can be lost because of turbulence in the saline [15]. Vertical traction provides the necessary joint distension without the need for saline distension; as the structure of the wrist joint allows for this [9]. The dry technique allows the operation to be performed without fluid extravasation and tension from water is not a concern. The dry technique allows longer procedures as bony landmarks are not blurred by the extravasated fluid, and avoids the complications of extravasated fluid [9].
Percutaneous fixation results in less soft tissue dissection, less disruption of vascularity, and shorter operative time [16]. Avoiding bone graft has the advantage of avoiding donor site morbidity, increased probability of infection, and chronic pain.
As far as we know, the number of articles on arthroscopic SCF is quite limited; moreover, not requiring bone graft results in even fewer articles, and this study is the largest prospective case series to date.
Nonunion has been reported from zero to 23% with open SCF and from zero to 10% with arthroscopic SCF [3, 17,18,19,20,21]. Similarly, in this study there was only one patient (3.3%) had non-fusion, knowing that he was a heavy smoker. The low incidence of nonunion and rapid fusion, achieved without bone graft, with arthroscopic surgery may be due to the preservation of the soft-tissue attachments and the blood supply to the carpals with a less invasive procedure.
The Lunate was not excised in this study. Rhee PC et al. described in a retrospective study that the presence or absence of the lunate did not significantly affect clinical outcomes in cases of limited carpal fusion for Kienbock’s disease [22]. Koh IH et al. reported that when comparing patients in whom the lunate was removed or not, the VAS and Modified Mayo Wrist Score (MMWS) were significantly improved in both cases, as was the case in this study. Hence, considering the added surgical time of lunate excision, it is thought that maintaining the lunate is preferable [23]
The pioneer of dry arthroscopy Francisco del Piñal presented a technique for dry arthroscopic scaphoidectomy and four-corner fusion. In their series, despite the first operation which lasted four hours, the last two operations were completed in less than two hours. No operations were converted to an open procedure [9]. Comparable to our results, halfway through this study the operative time was around one hour and 20 min, starting the study with an operative time of around three hours, and we did not convert any patient in this study to an open procedure.
Partial wrist fusions, including SCF, improve muscular strength by reducing pain after surgery and allow patients to return to their daily lives [24]. In this study, most patients showed improvements in terms of pain and grip strength. Flexion – extension arc ROM increased compared to the contralateral wrist, though this difference was not statistically significant, while radial and ulnar deviation decreased significantly compared to the contralateral wrist. Bouri et al. found similar results to this study regarding ROM in their systematic review and meta-analysis of the outcomes of open SCF in Kienböck’s disease, except for the ulnar deviation, where there was no significant difference after the surgery [25].
The literature primarily discusses open surgical techniques, meanwhile Leblebiciog˘lu et al., Baur, and Koh et al. performed SCF arthroscopically achieving generally good outcomes close to the result of this study [3, 4, 23]. Those studies used bone graft in contrast to Ertem et al. who did not use bone graft. Ertem in his study included 11 patients with Kienböck’s disease with a statistically significant difference in Mayo wrist score of post-operative third and sixth months and pre- and post-operative Quick Disabilities of Arm, Shoulder and Hand scores [19].
The most frequent complication of wrist arthroscopy was the failure to achieve the procedure (1.16%), and nerve lesions (1.17%) as stated by Leclercq C et al. Other complications include cartilage lesions, complex regional pain syndrome, wrist stiffness, and tendon lacerations with total complication incidence of wrist arthroscopy in about 5.98% of procedures done [26]. However, no complications described above were seen in this study.
This study has few limitations. The relatively short period for follow-up does not assess rates of delayed radiological and functional results such as long-term incidence of radioscaphoid arthritis. Thus, longer follow-up is needed. There also was no control group assessing the difference in outcomes compared to open SCF, so further prospective cohort studies are required. This study is meaningful in that it was done on a large number of patients to show that arthroscopic SCF can produce satisfactory results even without bone graft.
Arthroscopic SCF may be a quite challenging procedure initially, but we hope it will be standard practice, just like in our hospital, as it achieved significant improvement in pain and wrist function doing so with arthroscopy and without the need for bone graft or excision of the lunate.



留言 (0)