
記住我


Initially, 374 articles were retrieved, with 80 duplicates and 249 exclusions during title and abstract screening. Full-text screening eliminated nine more articles, leaving 36 for inclusion (Fig. 3). In six randomized controlled trials, all showed low selection bias. Among six articles lacking reported allocation concealment, 85.71% had low bias risk due to blinding during intervention. In four articles with blinding in outcome assessment, only 10.53% had low bias risk. All 36 studies had comprehensive outcome data, indicating minimal follow-up bias. Safety/efficacy data across the literature showed a low risk of reporting bias (100%). In 16 controlled studies, 14 revealed no statistically significant baseline differences, minimizing confounding bias. Meta-analysis funnel plot and Egger’s test (P > 0.05) suggested no publication bias (Fig. 4). Robust literature indicators, low bias susceptibility, heightened sensitivity, and high homogeneity collectively establish a robust foundation for this study.
Fig. 3
The literature retrieval strategy and process
The 36 articles, from 28 journals, averaged an impact factor of 2.303 ± 3.501 (maximum 18.9). English articles constituted 19.44%, while 80.56% were in Chinese. Mean citations and views were 5.94 ± 6.73 (maximum 30) and 139.61 ± 72.26 (maximum 304), respectively. 61.11% received research fund support. The literature offered reliable, readable, practical, and impactful information and data.
Fig. 4
Evaluation results of the sensitivity and stability of core data
Case dataFrom October 2011 to May 2022, 1965 ONFH patients (2222 hips) were treated, mean age 40.01 ± 4.90 years (16–70 years), with a disease duration of 10.52 ± 6.57 months (0.5–48 months). Unilateral cases dominated at 87.56%, significantly higher (7.04 times) than bilateral (12.44%) (P = 0.00004). Males comprised 66.21%, twice the female rate (33.79%) (P = 0.00015). Etiological factors included alcohol consumption (39.35%), steroid use (34.05%), idiopathic causes (20.75%), and trauma (5.85%). Alcohol and steroids were significantly higher than idiopathic and trauma (P < 0.05). The ARCO staging distribution was as follows: I (11.12%), II (76.33%), III (12.47%), and IV (0.09%) (Table 1). The study primarily focuses on middle-aged individuals in stage II of ONFH.
Table 1 Included literature and baseline case information Surgical dataSurgery duration averaged 54.52 ± 17.92 min (25–120 min), incision length 2.8 ± 1.0 cm (1–5 cm). Blood loss was 64.42 ± 22.77 ml (10–200 ml), hospitalization lasted 8.80 ± 3.16 days (4–14 days). Post-surgery, crutches were used for 2.95 ± 1.03 months (double support) and 7.07 ± 3.08 months (single support). BR utilization resulted in minimally invasive treatment with a short surgery, small incision, minimal blood loss, and a brief hospital stay.
Follow-up resultsOverall follow-up rate was 98.54%±4.57%, averaging 20.44 ± 10.41 months (3–73 months), stratified as follows: 34.63% for ≤ 1 year, 40.91% for ≤ 2 years, 11.34% for ≤ 3 years, 10.84% for ≤ 4 years, and 2.28% for ≤ 5 years.
Initial postoperative year showed rapid HHS increase, peaking at 82.40 ± 7.69 significant differences were noted at ≤ 3 months and ≤ 6 months compared to the preceding follow-up (P < 0.05). Subsequently, there was a gradual decline in HHS (Fig. 5), with no significant differences in the overall HIR (33.93%) observed across the follow-up periods. The HGR peaked in the first year and gradually decreased (Fig. 6), reaching an overall rate of 83.70% (Tables 2 and 3). BRs positively impacted symptom relief and functional recovery, stabilizing after one year.
Fig. 5
Trend of changes in HHS before and after surgery
Fig. 6
Trend of changes in HIR and HGR postoperative
Table 2 Statistical analysis of the extracted data Table 3 Meta-analysis of the extracted data ( Effect Size + 95%-CI)Radiological stability reached its maximum after 2 years, yielding an overall HSR of 88.91%. FSR declined in the initial four years, culminating in an 84.42% overall rate, with significant differences within the first three years (P < 0.05) (Fig. 7). The overall HRR was 7.97%, with 30.43% in the first year, 65.22% in the second year, and 4.35% in the third year; no replacements occurred thereafter. The efficacy of BRs was evident, achieving hip-preserving outcomes as early as 3 years postoperative.
Fig. 7
Trend of changes in HSR ang FSR postoperative
In the correlation study, lower preoperative HHS significantly correlated negatively with the HIR (r = −0.912), unrelated to postoperative HHS. Postoperative HHS improvement correlated positively with a higher HGR (r = 0.600) and HSR (r = 0.473), unrelated to preoperative HHS. As postoperative HHS increased, FSR rose, and HRR decreased, irrespective of preoperative HHS (Fig. 8). FSR correlated positively with HGR, HSR (r = 0.599, r = 0.542, respectively), and negatively with HRR (r = −0.786,). Hip preservation success increased with overall HIR exceeding 27%, HGR approaching 90%, or HSR surpassing 90% (Fig. 9). Improvement in postoperative symptoms directly influenced clinical outcomes, emphasizing the critical importance of efficacy indicators in assessing hip-preserving outcomes.
Fig. 8
Correlation results between patient symptoms and efficacy indicators. HIR HHS improvement rate, HGR Hip excellent & good rate, HSR Femoral head stability rate, FSR Femoral head stability rate, HRR Hip replacement rate
Fig. 9
Correlation results between FSR and other therapeutic indicators. HIR HHS improvement rate,HGR Hip excellent & good rate, HSR Femoral head stability rate, FSR Femoral head stability rate, HRR Hip replacement rate
Comparative studiesBR for Stage II vs. Stage III of ONFHIn treating 150 hips in Stage II and 82 in Stage III with BRs (average age 42, mean follow-up 22.7 months), both groups showed over 28% increase in final HHS (P < 0.001). Stage II had significantly higher HGR (84.6%) and HSR (90.67%) compared to Stage III (69.7% and 58.54%, respectively) (P = 0.001). Disease progression in Stage II (9.33%) was significantly lower than in Stage III (41.46%) (P = 0.0001). The overall FSR in Stage II (96.0%) was higher than in Stage III (87.8%) (P = 0.019) [17]. The BRs technique exhibits evident efficacy in hip-preservation, with outcomes showing a positive correlation to the stage of the disease.
BR vs. Core Decompression (CD)In a comparative study of Stage I-II patients, both CD and BR treatments were assessed, with 20 hips in each group (average age 35.4 years, mean follow-up 27.5 months). Significant improvements in HHS were observed for both groups, with the BR group showing a higher HIR (25.7% vs. 19.8%, P = 0.038), a greater HGR (95.0% vs. 70%, P = 0.046), and increased HSR (90% vs. 60%, P = 0.032) compared to the CD group [21]. These findings highlight the observed superiority of BRs over CD in terms of symptom improvement and successful hip preservation.
BR vs. Autologous Bone Grafting (ABG)In two studies comparing BR treatment (55 hips) to ABG (51 hips) for stage I to III patients, with follow-up durations of 12 and 29.27 months, both groups showed a significant improvement in the final HHS. One study indicated that the BR group had higher final HHS and HIR than the ABG group (P < 0.05) and a hig
her HGR (P < 0.05) [26]. While the second study reported no significant differences [33]. Although not statistically significant, the BR group showed higher HSR and FSR. Moreover, the FSR for stage II patients was higher than for stage III patients (P < 0.05) (Table 4). These findings confirm that the BR technique significantly outperforms simple ABG in terms of symptoms improvement and hip preservation.
Table 4 Comparison of the therapeutic effects of ceramic rods and bone autograftingBR in combination with Autologous Bone (AB)In a study treating 40 stages II to III ONFH hips, either with BR alone (BR group) or in combination with AB (AB group), with 20 hips in each group, and an average age of 35 years, the mean follow-up was 27.34 months. Both groups demonstrated significant postoperative improvements in HHS compared to preoperative scores (P < 0.05). The BR group exhibited higher HHS at 12 months and final follow-up than the AB group (P < 0.05). However, the AB group had a higher HGR, and HSR (78% and 85%, respectively) than the BR group (70% and 80%, respectively) (P < 0.05). During follow-up, three cases in the BR group and two cases in the AB group underwent total hip arthroplasty. The FSR for stages II and III in the BR group (88% and 67%, respectively) were significantly lower than the AB group (94% and 75%, respectively) (P < 0.05) [35]. This suggests that BR in combination with AB may improve hip-preserving outcomes but with potential risks of worsening symptoms.
BR in combination with Enriched bone marrow Stem Cells (ESC)In a study treating 29 hips with BR alone and 22 hips with BR in combination with ESC (average age 37.70 years, mean follow-up 24 months), the ESC group’s final HHS was higher than the BR group (P = 0.041). The respective success rates were 72.73% and 44.83% (P = 0.052), whereas failure rates were 4.5% and 17.2% (P = 0.340). Kaplan-Meier analysis did not show a significant difference in FSR (P = 0.203), but a trend indicated higher rates in the ESC group. Spearman rank correlation linked postoperative HHS and HRR [34]. This suggests that BRs in combination with ESC may contribute to symptom improvement, although there is insufficient evidence to support an enhancement of overall efficacy.
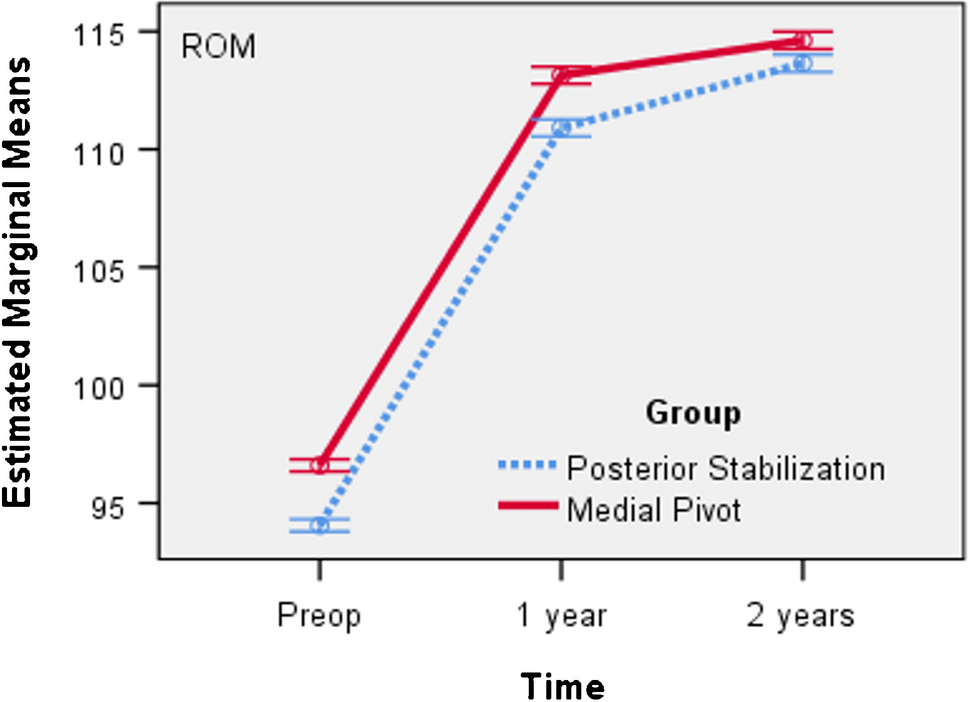
BR in combination with Platelet-Rich Plasma (PRP)In six studies [18, 20, 30, 32, 37, 38], 210 hips received BR treatment, and 221 hips received BR combined with PRP in stage I to II ONFH patients, averaging 42.67 years old with a mean follow-up of 25.22 months. In both groups, HHS peaked within two years, significantly improving at six months and one year compared to preoperative scores (P = 0.0012 and P = 0.0003, respectively), and the differences gradually diminished thereafter (Fig. 10). At three to 24 months, the PRP group showed higher HHS and HIR than the BR group (P < 0.05). The HGR, HSR, and FSR were comparable between groups, with a slightly higher HRR in the BR group (P = 0.0333) (Fig. 11). These findings suggest that the combination of BR with PRP contributes to the improvement of symptoms and diminishes the need for joint replacement.
Fig. 10
Comparison of HHS results between CR and PRP
Fig. 11
Comparison of efficacy between CR and PRP postop.(2 years)
BR in combination with Traditional Chinese Medicine (TCM)In four studies [14, 19, 25, 39], BRs were investigated for treating 170 hips, and a combination of BRs and TCM was used for 207 hips in ONFH management. Average age was 38.15 years, with a mean 12.69-month follow-up. HHS evaluation showed both groups peaked within the first year, maintaining stability thereafter. Over the three to 18 months follow-up period, the TCM group demonstrated higher HHS and a superior final HIR compared to the BR group (P < 0.05) (Fig. 12). However, no significant distinctions were observed in the final HGR, HSR, HRR and FSR (Fig. 13). These findings suggest that the incorporation of TCM alongside BRs may offer benefits in terms of symptom improvement, yet no conclusive evidence supports an enhancement in overall efficacy.
Fig. 12
Comparison of HHS results between CR and TCM
Fig. 13
Comparison of efficacy between CR and TCM postop. (18 months)
留言 (0)